
Abstract
BACKGROUND AND PURPOSE: There are few comparative studies regarding morphologic changes after kyphoplasty and vertebroplasty. The purpose of this study was to compare restoration of vertebral body height and wedge angle and cement leakage with kyphoplasty and vertebroplasty in osteoporotic compression fractures.
MATERIALS AND METHODS: Forty patients (57 vertebrae) were treated with kyphoplasty, and 66 patients (124 vertebrae) were treated with vertebroplasty. Cement leakage into the disk space and paravertebral soft tissues or veins was analyzed on immediate postoperative CT scans. The height and wedge angle were measured before and after treatment and analyzed with the Mann-Whitney U test and χ2 test.
RESULTS: Kyphoplasty and vertebroplasty both improved vertebral body height and the wedge angles (P < .05). However, these differences were not statistically significant when the 2 techniques were compared (P > .05). There were 18% of the kyphoplasty group and 49% of the vertebroplasty group that showed cement leakage into the paravertebral soft tissues or veins (P < .01). Cement leakage into the disk space occurred in 12% of the kyphoplasty group and in 25% of the vertebroplasty group (P < .01). However, no complications related to cement leakage were noted.
CONCLUSIONS: Both kyphoplasty and vertebroplasty achieved the same degree of height restoration and improvement of the wedge angle. Kyphoplasty resulted in less cement leakage into the disk space and paravertebral soft tissues or veins than vertebroplasty.
Percutaneous vertebroplasty is a minimally invasive procedure that provides pain relief and stability for osteoporotic compression fractures.1-10 The main goal of vertebroplasty is to relieve pain for patients in whom conservative treatment has failed. Restoration of vertebral body height is a secondary goal, and previous studies have shown that vertebroplasty can achieve some height restoration.11-15 Kyphoplasty is an alternative minimally invasive interventional method to vertebroplasty in which expandable balloons are used to restore height and to create a void in the central portion of a vertebral body before cement injection.16-31
An experimental study on cadaveric material has shown better height restoration with kyphoplasty than with vertebroplasty.16,31 However, only a few clinical studies have compared the 2 techniques.29,30,32 One clinical study showed better restoration of vertebral height and kyphotic angle with kyphoplasty,29 but this study measured vertebral height and wedge angle on plain radiography, which can be difficult to interpret in patients with osteoporosis. They did not evaluate for cement leakage.
Cement leakage into the paravertebral soft tissues or veins is generally asymptomatic. Cement leakage into the disk space is controversial because some studies have shown an increased risk for subsequent fractures of adjacent vertebral bodies,33,34 whereas others have claimed that cement leakage into the disk space is of no clinical significance.10,35
It is hypothesized that the use of expandable balloons in kyphoplasty would result in better height restoration than in vertebroplasty in which the cement is injected directly into the fractured and collapsed vertebral body. In kyphoplasty, the cement is injected under low pressure with use of balloons that allow cement to have higher viscosity than is typically used in vertebroplasty. It is hypothesized that these features of kyphoplasty would result in better height restoration and less cement leakage. The purpose of this retrospective study was to compare kyphoplasty and vertebroplasty with respect to the restoration of vertebral body height and improvement of the wedge angle as well as the incidence of cement leakage in patients with painful osteoporotic compression fractures.
Materials and Methods
Approval for this retrospective study, in compliance with the Health Insurance Portability and Accountability Act of 1996, was obtained from the Institutional Board of Research Associates with a waiver of informed consent.
Subjects
This study was based on 106 patients with painful osteoporotic compression fractures who had not responded to conservative treatment in a pain clinic or at an orthopedic clinic. Patients with pathologic fractures from known cancer were excluded. These patients were treated with either vertebroplasty or kyphoplasty at our institution from 2001 to 2007. The first 66 patients (124 vertebrae) were treated with vertebroplasty, whereas the last 40 patients (57 vertebrae) were treated with kyphoplasty. We retrospectively reviewed a clinical and imaging data base of these patients, who were treated by the same neuroradiologist. To avoid a learning curve effect, we did not include the first 12 patients treated with vertebroplasty at our institution.
In the vertebroplasty group, there were 45 women and 21 men, ranging in age between 45 and 93 years (mean age, 77 years). A total of 124 vertebral bodies were treated in 93 sessions. The locations and numbers of the treated vertebral bodies were as follows: T6 (n = 1), T7 (n = 5), T8 (n = 5), T9 (n = 8), T10 (n = 11), T11 (n = 16), T12 (n = 15), L1 (n = 30), L2 (n = 10), L3 (n = 11), and L4 (n = 12).
In the kyphoplasty group, there were 29 women and 11 men, ranging in age between 45 and 97 years (mean age, 75 years). A total of 57 vertebral bodies were treated in 47 sessions. The locations and numbers of the treated vertebral bodies were as follows: T7 (n = 2), T9 (n = 2), T10 (n = 1), T11 (n = 3), T12 (n = 12), L1 (n = 13), L2 (n = 10), L3 (n = 10), and L4 (n = 4).
Vertebroplasty Technique
Vertebroplasty was performed through a transpedicular approach with use of two 13-gauge bone biopsy needles (Osteo-Site; Cook, Bloomington, Ind) placed in the anterior one third of the vertebral body. Once the needles were placed in the vertebral body, liquid and powder polymethylmethacrylate (Cranioplastic; Codman, Raynham, Mass) were mixed with 12 g of barium sulfate (Bryan, Woburn, Mass) to a doughlike consistency (thicker than toothpaste). Under biplane fluoroscopic guidance, the cement was injected through the needles. The injection continued until the vertebral body was filled toward the posterior 25% of the vertebral body or until there was leakage. No unique postural maneuver to retain the alignment was used before or during the procedure. After the cement injection, the patient remained prone on the angiographic table until the cement was hardened (approximately 15 minutes); the patient was then transferred to a stretcher.
Kyphoplasty Technique
Kyphoplasty was also performed through a bipedicular approach by placement of working cannulas bilaterally with use of standard kyphoplasty equipment (KyphX; Kyphon, Sunnyvale, Calif). Through the working cannula, a drill was used to create a tract for the balloon into the center of the vertebral body. Twenty-mm balloons were used. In a few cases with small vertebral bodies, we used 15-mm balloons. We used the cement mixed according to the manufacturer's recommendations. The injection also continued in the same manner as in vertebroplasty. We usually injected the cement approximately 10 minutes after the start of mixing.
All vertebroplasty and kyphoplasty procedures were done by the same operator with biplane fluoroscopy, local anesthesia, and with the patient under moderate sedation. All patients were discharged to home approximately 2 hours after the procedure.
Imaging Technique
We performed preoperative MR imaging with a 1.5T imager. At a minimum fast spin-echo sagittal T2-weighted and sagittal spin-echo T1-weighted images were obtained. In many cases, additional sequences were also available. We obtained postoperative CT scans by using a single section or 4-, 16-, or 40-detector row CT scanners, which were reformatted at 2- to 3-mm section thickness in 3 orthogonal planes.
Image Assessment
The raw MR and CT data were transferred to a workstation (Advantage Windows 4.1; GE Healthcare, Milwaukee, Wis). Preoperative vertebral height was measured in the anterior, central, and posterior portions in the midsagittal plane. Measurements were done by the first author (A.H.). One adjacent nonfractured vertebral body was also measured on preoperative MR images and on postoperative CT scans to validate the measurements. The presence of cement leakage into the adjacent intervertebral disk and veins was defined as any contrast beyond the cortical margin of the vertebral body seen on postoperative CT scans.
Statistical Analysis
Statistical analysis was performed with commercially available software (SPSS 16.0J for Windows; SPSS, Chicago, Ill). The statistical significances of changes in vertebral body height and wedge angle with each treatment were evaluated with the paired t test. The statistical significances of changes in vertebral body height and wedge angle with the 2 treatment techniques were evaluated with the Mann-Whitney U test. The statistical significance of the difference in cement leakage between the 2 treatment techniques was evaluated with the χ2 test. The statistical significances of the vertebral body height and the wedge angle of the control vertebrae were evaluated with the paired t test. A P value of less than .05 was considered to indicate a statistically significant difference.
Results
The mean preoperative vertebral body height and wedge angle were not statistically different when the 2 groups were compared (P > .05; Tables 1, 2). Vertebroplasty and kyphoplasty both improved vertebral body height in the anterior, central, and posterior portions and also at the wedge angles (P < .05; Tables 1 and 2). However, these differences were not statistically significant when these 2 techniques were compared (P > .05).
Mean vertebral body height (mm) before and after treatment with kyphoplasty (n = 57) and vertebroplasty (n = 124)
Mean wedge angle (°) before and after treatment with kyphoplasty (n = 57) and vertebroplasty (n = 124)
Cement leakage into the disk was more prevalent in the vertebroplasty group (25.0%) than in the kyphoplasty group (12.3%; P < .01; Table 3, Figs 1 and 2). Cement leakage into the paravertebral soft tissues or veins was also more prevalent in the vertebroplasty group (49.2%) than in the kyphoplasty group (17.5%; P < .01; Table 3). However, no complications related to cement leakage were noted.

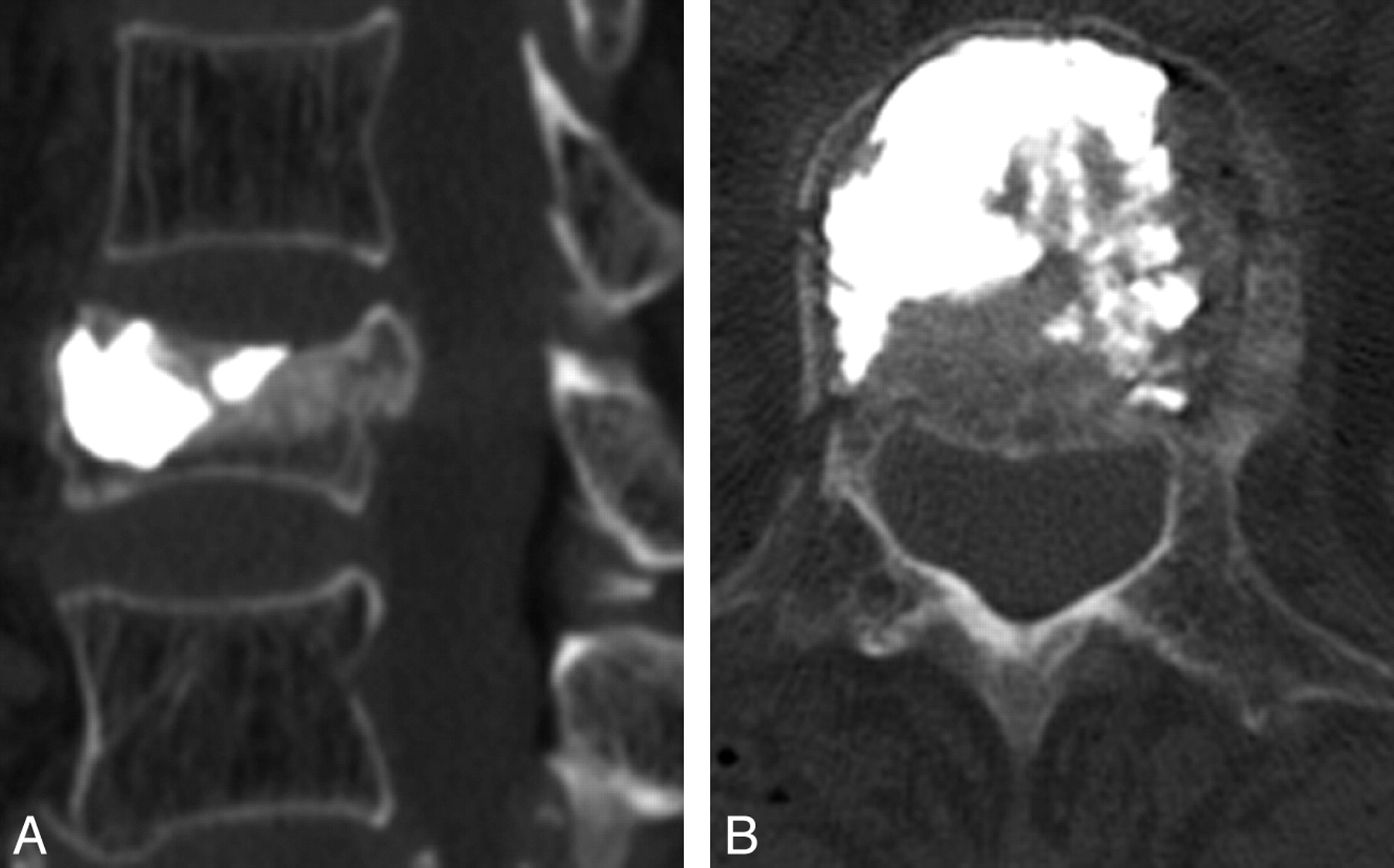
A 75-year-old woman with compression fractures at T12 and L1, which were treated with vertebroplasty. A, Postoperative CT scan with sagittal re-formation shows intradiskal cement leakages at L1-L2 disk space (arrow). B, Postoperative axial CT shows cement leakage into the paravertebral vein at T12 on the left (arrow).

An 85-year-old woman with a compression fracture at L1, which was treated with kyphoplasty. A, Postoperative CT scan with sagittal re-formation shows no intradiskal cement leakage from the L1 vertebral body. B, Postoperative axial CT scan again shows no cement leakage from the L1 vertebral body.
Cement leakage (%) into disk spaces and paravertebral soft tissues/veins during kyphoplasty (57 vertebrae) and vertebroplasty (124 vertebrae)
The average discrepancy in the height of the control vertebrae between the preoperative MR imaging and the postoperative CT examinations was 0 mm (range, 0–1.3 mm). The average discrepancy in wedge angle between the preoperative MR imaging and the postoperative CT examinations was 0° (range, 0–2.0°). There were no statistically significant differences in these measurements (P > .05), indicating that the measurements were valid.
Discussion
This study compared vertebroplasty and kyphoplasty performed by the same operator in 2 groups of similar patients. In accordance with several previous studies,11-15,17,26 we have shown that both kyphoplasty and vertebroplasty can restore some vertebral body height and improve wedge angle. We saw improvements in vertebral body height of 1.5 and 1.4 mm and improvements in wedge angle of 3.0 and 2.7° with kyphoplasty and vertebroplasty, respectively. In a previous study on cadaveric material, Hiwatashi et al31 showed kyphoplasty to restore vertebral body height slightly better than vertebroplasty (93% vs 82%). Other authors have also reported a greater height restoration in kyphoplasty than in vertebroplasty.16 However, the difference in height restoration between the 2 techniques is generally small, and it is unclear if this small difference in height restoration has clinical significance. Proponents of kyphoplasty have reported a height restoration from 3 to 5 mm with reduced kyphotic deformity by 3 to 14°.17-26 Other studies have shown that vertebroplasty also can restore vertebral height and improve the wedge angle to approximately the same extent.11-14 In our study, the difference between the 2 techniques was not significant in this respect. Compared with cadaveric studies, the surrounding soft tissue including disks, vertebrae, ligaments, or muscles may reduce the amount of expansion.
The clinical importance of the correction of the vertebral body during kyphoplasty and vertebroplasty remains unclear. Previous studies have failed to show the relationship between height restoration and pain relief during cement augmentation therapy.36,37 McKiernan et al36 have reported that height restoration achieved at vertebroplasty did not result in additional pain relief or improved quality of life. Feltes et al37 have also reported excellent pain management with kyphoplasty without restoration of vertebral body height. A randomized study comparing the results of kyphoplasty and vertebroplasty seems to be justified.
This study showed that kyphoplasty resulted in less leakage of cement into the disk and paravertebral soft tissues or veins. This result is in accordance with a previous study that had shown that cement extravasation can be seen in up to 88% of vertebroplasties1-10 but up to 33% of kyphoplasties.10,19-28 With 1 exception,30 other studies have also shown more frequent cement leakage with vertebroplasty than with kyphoplasty.38,39 The less frequent cement leakage with kyphoplasty is probably because the injection technique uses more viscous cement and the cavity is treated with kyphoplasty balloons. Thus, kyphoplasty creates a void in the bone into which the thick cement is injected under low pressure. This technique is different from vertebroplasty because with vertebroplasty, cement is injected directly into the bone under higher pressure. The cement leakage into the paravertebral soft tissues or veins was asymptomatic in all of our patients and was probably of no clinical significance. However, symptomatic cement leakage has been reported, resulting in worsening of spinal stenosis and pulmonary embolism.30,40,41
The sequela of cement leakage into the disk space is controversial. A few studies33,34 have reported an increased incidence of subsequent fractures of adjacent vertebral bodies when there is cement in the disk. This is probably related to the amount of cement in the disk because Syed et al35 have reported that a small amount of cement in the disk does not increase the risk for adjacent fractures. We are working on a separate study on the incidence of subsequent fractures of adjacent vertebral bodies after vertebroplasty and kyphoplasty.
One limitation of this retrospective study was the lack of randomization of the patients in the 2 groups. There is a good reason to believe that these 2 groups are comparable because the study was done during 2 consecutive periods in the same department, by the same operator, and by the same referring clinicians. We treated the first 66 patients with vertebroplasty and then treated the next 40 patients with kyphoplasty. To avoid a learning curve effect, we did not include the first 12 patients treated with vertebroplasty at our institution. We did not record the exact amount of cement injected but, instead, attempted to do an optimal filling of each vertebral body treated on the basis of the fluoroscopy image during the procedure. The difference in imaging modalities with preoperative MR imaging and postoperative CT scans after the procedure does not seem to be an issue because the preoperative and postoperative measurements of the untreated vertebral bodies were virtually the same. To avoid excessive radiation, we did not perform preoperative CT examinations routinely in this study population.
Conclusions
Both kyphoplasty and vertebroplasty achieved some restoration of vertebral body height and improved the wedge angle, but there was no appreciable difference between the 2 techniques. Kyphoplasty resulted in a lower incidence of cement leakage into the disk and the paravertebral veins compared with vertebroplasty; however, no complications related to cement leakage were observed.
Footnotes
This study was supported in part by research grants from the Ministry of Education, Culture, Sports, Science and Technology (19790879) and the Japan Radiological Society (KJ-18-3).
References
- Received October 22, 2008.
- Accepted after revision November 5, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Effect of Kyphoplasty on Mortality in Symptomatic Vertebral Compression Fractures: A Review
- Analysis of Related Factors on the Deformity Correction of Balloon Kyphoplasty
- In Not Only Vertebroplasty but Also Kyphoplasty, the Resolution of Vertebral Deformities Depends on Vertebral Mobility
- Significance of Dynamic Mobility in Restoring Vertebral Body Height in Vertebroplasty
- Vertebral Augmentation for Compression Fractures Caused by Malignant Disease