
Abstract
BACKGROUND AND PURPOSE: Nonconvulsive status epilepticus (NCSE) is associated with a mortality rate of up to 18%, therefore requiring prompt diagnosis and treatment. Our aim was to evaluate the diagnostic value of perfusion CT (PCT) in the differential diagnosis of NCSE versus postictal states in patients presenting with persistent altered mental states after a preceding epileptic seizure. We hypothesized that regional cortical hyperperfusion can be measured by PCT in patients with NCSE, whereas it is not present in postictal states.
MATERIALS AND METHODS: Nineteen patients with persistent altered mental status after a preceding epileptic seizure underwent PCT and electroencephalography (EEG). Patients were stratified as presenting with NCSE (n = 9) or a postictal state (n = 10) on the basis of clinical history and EEG data. Quantitative and visual analysis of the perfusion maps was performed.
RESULTS: Patients during NCSE had significantly increased regional cerebral blood flow (P > .0001), increased regional cerebral blood volume (P > .001), and decreased (P > .001) mean transit time compared with the postictal state. Regional cortical hyperperfusion was depicted in 7/9 of patients with NCSE by ad hoc analysis of parametric perfusion maps during emergency conditions but was not a feature of postictal states. The areas of hyperperfusion were concordant with transient clinical symptoms and EEG topography in all cases.
CONCLUSIONS: Visual analysis of perfusion maps detected regional hyperperfusion in NCSE with a sensitivity of 78%. The broad availability and short processing time of PCT in an emergency situation is a benefit compared with EEG. Consequently, the use of PCT in epilepsy may accelerate the diagnosis of NCSE. PCT may qualify as a complementary diagnostic tool to EEG in patients with persistent altered mental state after a preceding seizure.
Nonconvulsive status epilepticus (NCSE) is defined as a change in behavior and/or mental processes from baseline associated with continuous epileptiform discharges in the electroencephalography (EEG) in the absence of convulsive symptoms.1 In unselected patients, it is associated with a mortality rate of up to 18%.2 Notably both subtle status epilepticus (SSE), a subtype of NCSE that develops from generalized convulsive status epilepticus (GCSE), in which motor symptoms become less florid,3 and NCSE in coma indicate a bad prognosis.1 Mortality is reported to be mainly dependent on the underlying etiology and age.4 Furthermore, NCSE has been shown to be an independent predictor of high mortality and morbidity and the occurrence of refractory status epilepticus.5–7 There is evidence that 2 hours after the clinically successful cessation of convulsive activity, EEG demonstrates persistent epileptic seizure activity in 48% of patients, fulfilling, in 14%, the criteria of NCSE.5 Because NSCE is difficult to differentiate from other postictal conditions on a clinical basis, the current criteria for the diagnosis require EEG seizure activity. The estimated time from the patient's approval for emergency EEG to its first available interpretation is approximately 3 hours.8 This delay is far beyond what is considered acceptable in the treatment of status epilepticus.9
Because epileptic activity causes an increased metabolic demand in the involved cerebral cortex, which is accompanied by temporarily increased regional brain perfusion,10,11 measuring cerebral perfusion has become a widely accepted method for localizing the zone of ictal activity.10,12 In NCSE, hyperperfusion is reported to be confined mainly to the affected cortex without significant white matter involvement13,14 and focal cortical hyperperfusion tends to encompass widespread areas of the affected hemisphere if consciousness is reduced.15,16 Thus, we investigated retrospectively 19 patients after a preceding epileptic seizure with persistent altered mental status with perfusion CT (PCT) and EEG. We hypothesized that regional cortical hyperperfusion can be measured by PCT in patients with NCSE and is not a feature of postictal states and that visual analysis of the perfusion maps during emergency conditions is concordant with post hoc quantitative analysis. The value of PCT in the diagnostic work-up of NCSE is discussed.
Materials and Methods
Study Population
We retrospectively studied 19 patients admitted to the emergency department or the Department of Neurology of our institution. All patients presented with a witnessed preceding clinical epileptic seizure and persistent altered mental status. Unenhanced contrast-enhanced brain CT and PCT were performed during the routine diagnostic work-up of these patients at the request of the referring physician to rule out an acute stroke or structural brain lesions as the cause of the seizure and altered mental status and/or neurologic deficit. In all patients, EEG was performed within 2 hours after the CT scanning. For analysis, patient data were identified by using the Department of Radiology admission log. Medical records were reviewed after patient discharge. We recorded demographic data (sex, age), medical history (epilepsy, neurologic comorbidities), and the clinical characteristics (seizure classification, focal neurologic deficits, worst Glasgow Coma Scale [GCS] score, respiratory deficits leading to mechanical ventilation); survival was assessed by evaluation of the discharge logs. The study was approved by the local ethics committee.
CT
Recordings.
All CT studies were performed on a LightSpeed Ultra 8-section multisection scanner (GE Healthcare, Milwaukee, Wis). The CT protocol included unenhanced CT scanning with 5-mm transverse sections angled along the canthomeatal line over the whole brain. Subsequently, 2 contiguous 10-mm slabs of the brain were selected; they were placed to cover brain areas adjacent to structural lesions. In patients without structural abnormalities, section position was selected at the level of the rostral border of the basal ganglia. A dynamic contrast-enhanced cine scan (display FOV, 200 mm; matrix, 512 × 512; 80 kV; 200 mA; 1 s/rotation) was obtained after a bolus injection of 40 mL of high-molecular contrast medium (Iomeron 400; Bracco, Milan, Italy). Injection was performed with a power injector through a 20-gauge catheter into a superficial vein at the antecubital fossa of the forearm with a flow rate of 4 mL/s. Two simultaneous dynamic adjacent CT scans of 10-mm thickness each were obtained. Total acquisition time was 45 seconds with a temporal resolution of 1 second. After bolus administration, all patients with intracranial lesions underwent transverse CT scanning of 5-mm thickness through the whole brain in the same orientation as that of the initial nonenhanced series.
Data Analysis
Perfusion Maps and Visual Analysis.
All CT perfusion scans were processed by using software developed in-house by J.S. (Perfusion Evaluation, Version 3.617), which allows computation of perfusion maps of CT and MR imaging data. The image-processing algorithm for the computation of regional cerebral blood flow (rCBF), regional cerebral blood volume (rCBV), and mean transit time (MTT) maps is based on a deconvolution algorithm published by Ostergaard et al.18 The algorithm requires the user to locate a set of pixels in an artery that feeds the brain tissue under investigation. With the use of the arterial input function, which is derived from the set of arterial pixels, a deconvolution is carried out that allows the computation of the rCBF, rCBV, and MTT maps. Perfusion maps were independently interpreted by 3 experienced neuroradiologists (R.W., F.v.B., C.O.) not aware of the EEG results.
Segmentation and Quantitative Analysis.
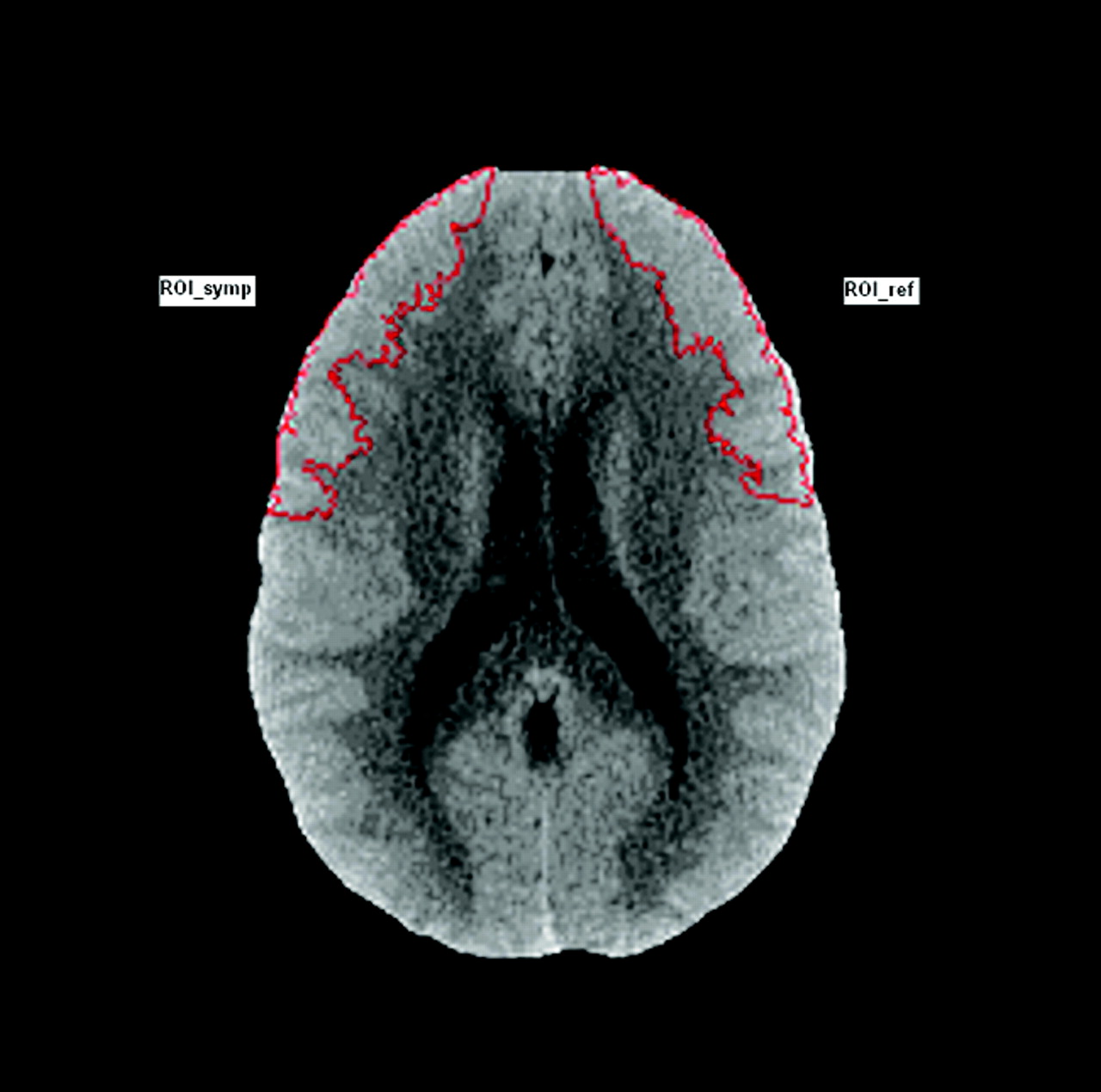
To establish a quantitative basis for evaluation, we used a semiautomatic segmentation program (Perfusion Evaluation, Version 3.6) to separate the cortex and white matter. The segmentation was performed by a threshold algorithm, for which the user predefined the minimum and maximum pixel-intensity threshold value. To obtain a sufficient signal-intensity-to-noise ratio for accurate discrimination of cortical tissue from deep white matter, the first 6 acquisitions of the PCT series before contrast agent arrival were averaged. Regions of interest (ROIs) covering the symptomatic cortical region were defined as contralateral to the side of the clinical symptoms and/or adjacent to a structural lesion if present; in cases with no lesions, the frontal cortical region was selected (ROI_symp). A corresponding region of interest in the unaffected cortical region of the other hemisphere was defined (ROI_ref) (Fig 1). For each ROI, the rCBV, rCBF, and MTT values were calculated. Asymmetry indices (AI) for rCBV, rCBF, and MTT of each individual perfusion were defined as follows:  Calculation of AI provides results independent of interindividual perfusion differences and intraindividual differences of perfusion in different vascular territories. Hyperperfusion was defined as AI > 10 in rCBF; and hypoperfusion, as AI < −10.19,20
Calculation of AI provides results independent of interindividual perfusion differences and intraindividual differences of perfusion in different vascular territories. Hyperperfusion was defined as AI > 10 in rCBF; and hypoperfusion, as AI < −10.19,20

Semiautomatic segmentation of the cortical region.
The AI values for rCBF, rCBV, and MTT of the different patient groups were compared by using an unpaired Mann-Whitney U test. The significance of group differences of patient data was analyzed by using nonparametric statistical analysis (Fisher exact test, 2-sided; Mann-Whitney U test) with the commercial statistics software Statistical Package for the Social Sciences, Version 14.0 (SPSS, Chicago, Ill).
EEG
EEG was recorded via 19 surface electrodes placed according to the international 10–20 system within 2 hours after the CT scanning by using a standard software package (NicOne, Nicolet Biomedical; Viasys Healthcare, Madison, Wis). The EEG recordings were independently analyzed by a certified electroencephalographer (A.N.), who was unaware of the PCT results.
Definitions of NCSE and Postictal State
Episodes were classified as NCSE if the subject exhibited changes in behavior and/or mental processes lasting longer than 30 minutes without clinical signs of overt convulsive activity and if the EEG showed continuous or intermittent ictal activity consisting of rhythmic discharges (spikes, sharp waves, or slow wave discharges).5 A classification as NCSE allowed the presence of subtle movements and isolated jerks.21 Patients in NCSE with initial GTCS were classified as having SSE; patients without GTCS, as having complex partial status epilepticus; and patients with coma due to central nervous system disorder with NCSE, as having coma with NCSE.1
Episodes were classified as postictal if after a preceding seizure, the subject did not present with persistent ictal semiology (eg, myoclonus) and no ictal activity was present on EEG.
Results
Clinical, EEG, and perfusion data of the patients are summarized in on-line Tables 1 and 2. The patients in the NCSE group were older than those in the postictal group (67.8 versus 44.0 years, P = .015); no significant differences were found for sex, worst GCS, presence of previously diagnosed epilepsy, and the need for artificial ventilation. In all patients with NCSE, a neurologic comorbidity was present, compared with 3/10 in the postictal group (on-line Tables 1 and 2).
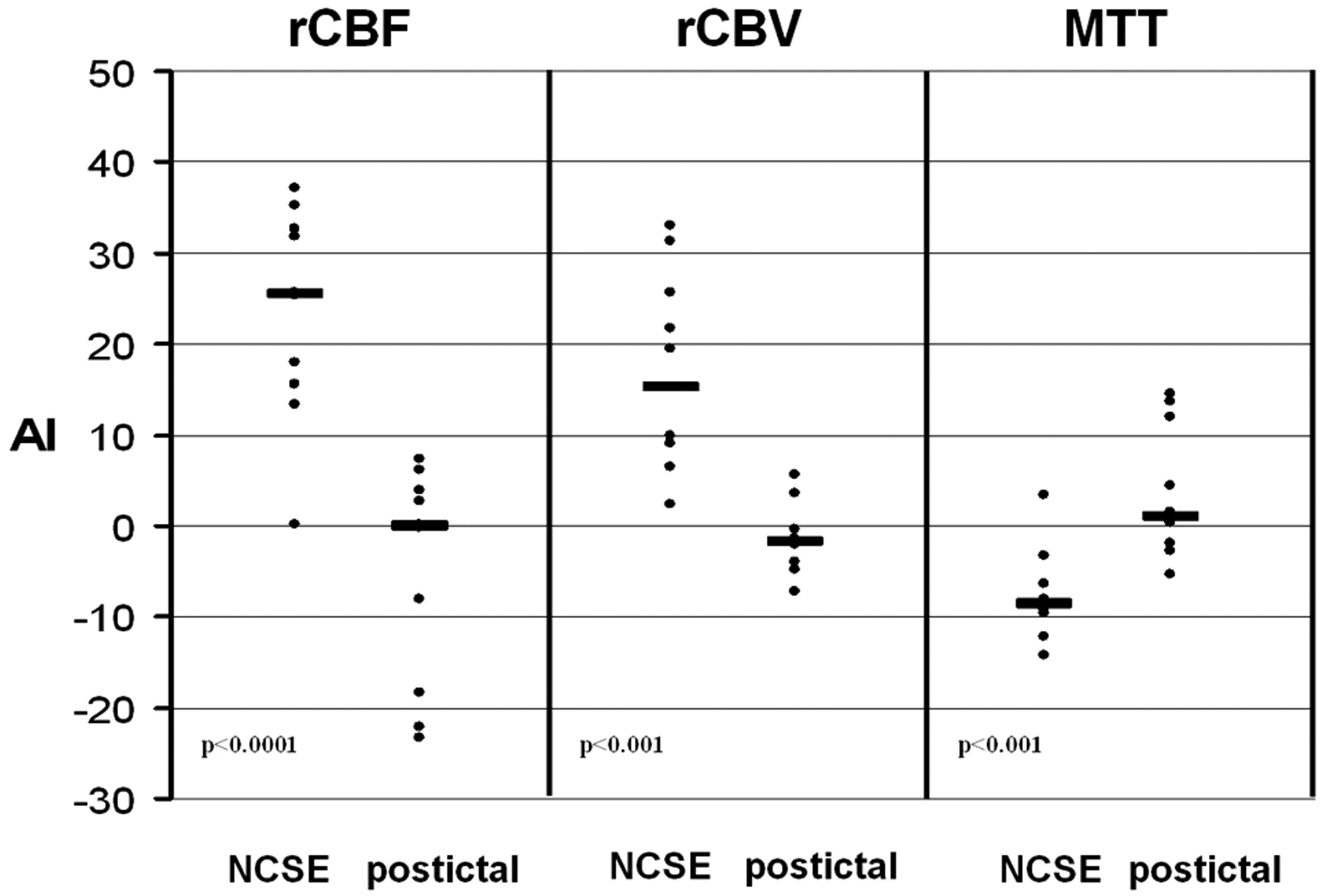
Fatal outcome was 44% in the NCSE group versus 10% in the postictal group; due to the small sample size, this difference did not reach statistical significance. Quantitative analysis of perfusion parameters for rCBF, rCBV, and MTT of the NCSE and postictal group is summarized in Fig 2. The intergroup differences were highly significant for all parameters (rCBF, P < .0001; rCBV, P < .001; MTT, P < .001).

Group comparison between patients in NSCE and postictal state demonstrates significantly higher rCBF, rCBV, and shorter MTT in NCSE-versus-postictal states.
NCSE
In 9 patients, the diagnosis of NCSE was based on clinical criteria and EEG findings.
Quantitative analysis of PCT showed regional cortical hyperperfusion corresponding to the patients’ neurologic deficits or jerks in 8/9 patients. The lateralization was confirmed by EEG in all patients. In patient 1.6 with chronic left parietal hemorrhage, symmetric rCBF values were obtained outside the insult. EEG recordings revealed focal seizure activity in the left frontal lobe.
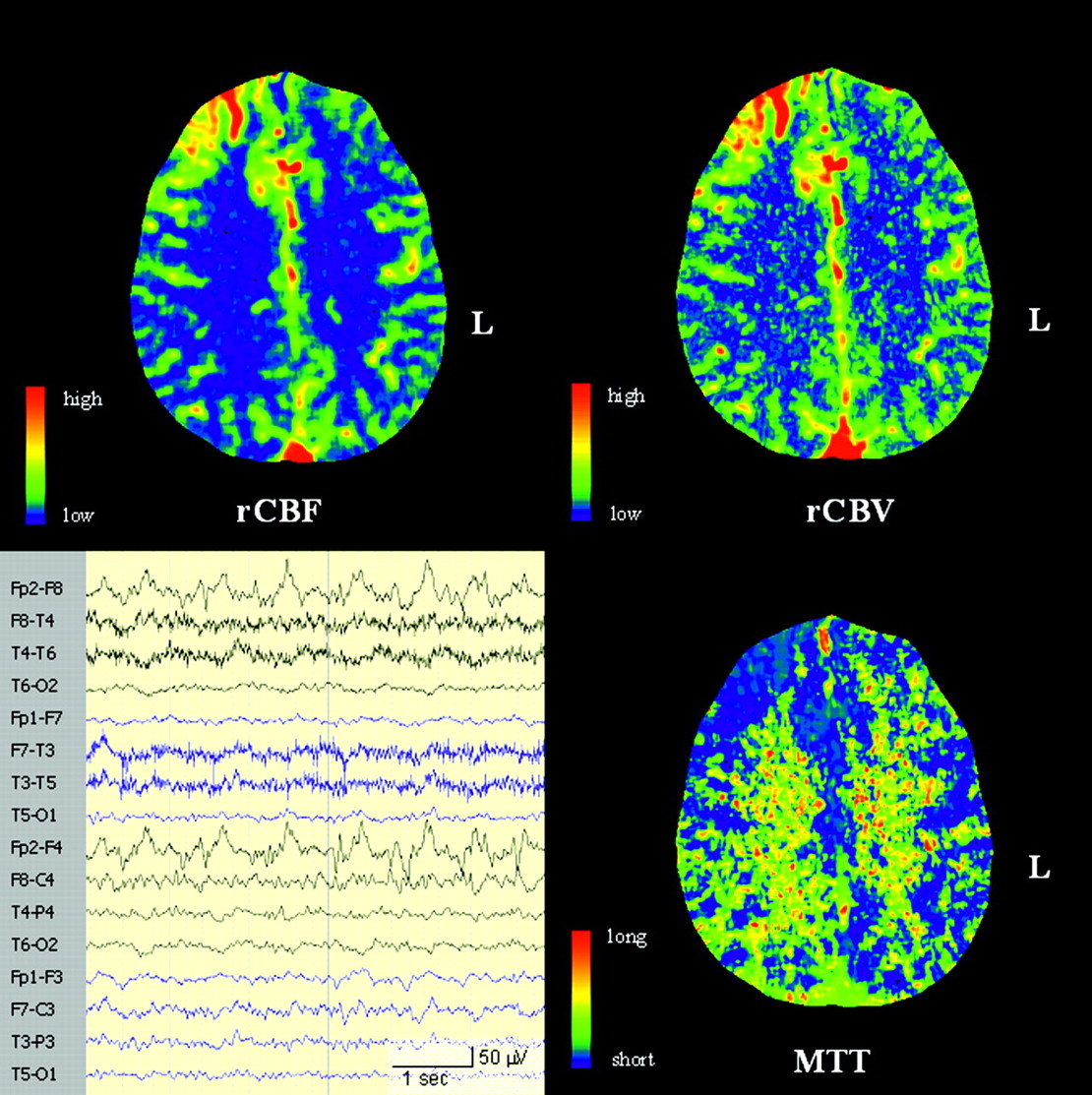
Visual analysis allowed the identification and lateralization of a regional hyperperfusion in 8/9 patients. The inter-rater concordance was 100% among the 3 independent readers. Perfusion maps revealed hyperperfusion in the gray matter, sparing the adjacent deep white matter and outlying boundaries of vascular territories (Fig 3). In patient 1.9, the insular hyperperfusion identified by quantitative analysis was not visible during ad hoc visual analysis of the parametric maps. In accordance with the quantitative analysis, the hyperperfusion of patient 1.6 could not be identified visually, either.

Cortical hyperperfusion frontal right during NCSE. Bottom left: EEG shows right frontal spike-and-wave activity (patient 1.3).
Postictal State
All 10 patients in the postictal group presented with initial GTCS. At admission, jerks were not a feature, and EEG did not show seizure activity in any of the subjects. Quantitative analysis revealed a regional hypoperfusion in 3/10 patients. In these patients (2.1, 2.2, and 2.3), the lateralization fit their respective clinical deficits and EEG. The remaining 7 patients showed symmetric brain perfusion values. In the visual analysis, none of the 10 patients showed signs of regional hyperperfusion. Reduced regional perfusion was detected in the 3 patients (2.1, 2.2, and 2.3) with lateralizing signs. The distribution of the regional hypoperfusion differed from that of the NCSE in that both cortical and subcortical regions were involved (Fig 4). Again, the inter-rater concordance was 100% among the 3 independent readers.

Widespread hypoperfusion over the right hemisphere in a postictal state encompassing carotid and basilar vascular territories. Bottom left: EEG shows a diffuse right hemispheric slowing (patient 2.3).
Discussion
This series investigated the diagnostic value of PCT in patients presenting with a preceding epileptic seizure and a persistent altered mental state in the differential diagnosis of NCSE versus postictal states. We demonstrated that regional perfusion changes, as recorded with PCT, allow the differentiation between NCSE and postictal conditions. The feasibility and safety of PCT for the evaluation of epileptic seizures has been demonstrated previously.22 In contrast to our pilot study, which investigated solely quantitative regional perfusion asymmetry as a discriminator, this time we have focused on the visual analysis of perfusion maps, testing whether the diagnosis can be made ad hoc by reading parametric perfusion maps during emergency conditions. In our cohort, the mortality in the NCSE group was higher than that in the published reports,2,4 probably due to the selected population with severe neurologic comorbidities. Nevertheless, the high mortality in NCSE indicates that procedures for immediate therapeutic and prognostic implications are needed. The broad availability and short processing time of PCT is an advantage compared with EEG.8 Therefore, the use of PCT in epilepsy may reduce the time to diagnose NCSE. Results of PCT may prompt a diagnostic application of antiepileptic drugs, in particular if EEG is not available, and an immediate evaluation of the underlying process.
Quantitative Analysis
Quantitative post hoc analysis of PCT was concordant with the clinical and EEG data in all except 1 patient in our cohort. These results indicate that PCT-derived cortical perfusion maps discriminate NCSE and a postictal state. Thus, we have confirmed our previous results22 and the findings of a recent case study23 that investigated cortical hyperperfusion as a discriminating feature of NCSE. Some reports have found a persistence of cortical hyperperfusion after EEG cessation of epileptic seizures,24,25 but such effects tend to switch rapidly (within 90 seconds of seizure end) into neocortical hypoperfusion26 and have been excluded in our series because the time from cessation of convulsions to PCT ranged from 30 to 90 minutes.
Visual Analysis in NCSE
PCT provides instantaneous results on altered brain perfusion in emergency situations. In our study, ad hoc qualitative analysis performed by visual inspection of the parametric perfusion maps identified regional hyperperfusion in 78% of patients with NCSE. In 2 patients with NCSE, visual analysis did not detect any perfusion changes in favor of ongoing seizure activity: In patient 1.9, quantitative analysis showed regional hyperperfusion in the left perisylvian regions, which was not confirmed by visual inspection, probably due to the overlap of cortical hyperperfusion and of abundant arteries in the adjacent Sylvian fissure. In patient 1.6, despite a clearly lateralized and focal frontal status epilepticus on EEG, no perfusion changes were detected. This might reflect the fact that NCSE is a highly dynamic process including periods with generalized or without active ongoing seizure activity, indicating a limitation of the PCT technique mapping only 45 seconds of cerebral perfusion. Although the PCT approach presented here is limited by the anatomic coverage along the craniocaudal axis of, at maximum, 40 mm, new CT scanners are capable of covering ≥100 mm. The use of MR perfusion measurements, offering coverage of the entire brain parenchyma, is limited due to safety issues in patient monitoring in the scanner and by a limited availability in emergency conditions.
Visual Analysis in Postictal States
In our series, PCT demonstrated hypoperfusion, mainly visible on MTT maps, during a postictal state in 3 patients with a focal neurologic deficit (Todd paresis), which is in keeping with previous results.22,27 Beyond hypoperfusion, the pattern of perfusion alterations differed from those of NCSE in that both cortical and subcortical regions were involved. Subcortical hypoperfusion is in agreement with previous single-photon emission CT (SPECT) studies.26,28 The absence of regional postictal hypoperfusion in 7 patients without lateralizing signs might reflect the fact that the altered mental state in these patients was caused by a diffuse functional impairment of the associated cortex in postictal states after a primary generalized seizure29 or due to the sedation effects of antiepileptic drugs, but not to focal postictal brain exhaustion. Similar observations have been confirmed by SPECT studies, in which visual inspection of postictal hypoperfusion has a very low sensitivity12,24 and is not helpful in delineating the irritative zone. Although the results of PCT in the setting of patients with epilepsy seem to be most valuable in identifying whether there is a regional hyperperfusion indicating ongoing seizure activity, a regional hypoperfusion may still be of diagnostic relevance in patients with lateralizing clinical signs.
Comparison with PCT in Other Pathologies
In this series, we evaluated a new indication for PCT for the differentiation of NCSE and postictal states. In clinical routine, PCT is already a highly valuable and standardized tool in other conditions (eg, in stroke). Comparing the findings of PCT in epilepsy and stroke, however, reveals some well-defined differences. First, the quantity of focal perfusion changes differs between NCSE and stroke: In NCSE, mean focal rCBF change accounts for an AI of 23% (SD, 11.6; max, 37%) and, in a postictal state with lateralizing signs, for 21% (SD, 2.55; max, 23%; Fig 2), which is in keeping with previous SPECT studies.12,24 In contrast, in stroke, the core of an infarction shows an rCBF reduction exceeding 80% compared with the other hemisphere,30 and the defined threshold for a penumbra requires a minimal rCBF reduction of 34%.31
Second, the distribution of focal perfusion changes differs between NCSE and stroke: Concordant with the concept of cortical generation of epileptic activity and with previous MR imaging and CBF-SPECT studies,13,14 ictal hyperperfusion is predominantly present in the cortex and may encompass multiple vascular territories (Fig 3).32,33 Acute stroke presenting with epileptic seizures or status epilepticus at onset has been reported,34 but we did not encounter such etiologies in our series. Furthermore, PCT has been used for prognostic issues in traumatic brain injury.35 Typically, its corticosubcortical decrease in rCBF35,36 allows a differentiation between traumatic brain injury and NCSE. Several other studies have demonstrated the correlation between microvessel attenuation and increased rCBV and blood flow in high-grade tumors with PCT.37 The different morphologies and perfusion patterns of NCSE and brain tumors, however, should not provide any diagnostic problem apart from subjects in whom perfusion changes due to epileptic seizures and neovascularized brain tumors coincide. Hyperperfusion in other pathologies, such as encephalitis38 and abscesses,39 has been sporadically reported but did not omit the adjacent white matter.
Conclusions
In our cohort, regional cortical hyperperfusion could be depicted in 78% of patients with NCSE by visual interpretation of parametric perfusion maps during emergency conditions. The presence of a cortical hyperperfusion is a valid predictor of ongoing seizure activity, whereas the absence of perfusion alterations may not help to differentiate ictal from postictal states. Because of its broad availability and short processing time, PCT may qualify as a complementary diagnostic tool to EEG in patients with persistent altered mental state after a preceding seizure. Although the use of PCT for predicting patient outcome or guiding clinical management has not been established, its contribution to extract focal perfusion changes in epilepsy is clearly encouraging. Because the present retrospective study is limited by its small number of patients, a multicenter prospective study on an unselected cohort of patients is currently in preparation to estimate the exact impact of PCT as a diagnostic tool in NCSE.
Footnotes
indicates article with supplemental on-line tables.
References
- Received October 9, 2008.
- Accepted after revision November 7, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cortical Hyperperfusion on MRI Arterial Spin-Labeling during the Interictal Period of Patients with Migraine Headache
- Acute Ischemic Stroke or Epileptic Seizure? Yield of CT Perfusion in a "Code Stroke" Situation
- Can perfusion CT unmask postictal stroke mimics?: A case-control study of 133 patients
- Cerebellar Hypoperfusion in Migraine Attack: Incidence and Significance
- Electrographic status epilepticus and long-term outcome in critically ill children
- Teaching NeuroImages: Ictal hyperperfusion
- Nonconvulsive seizures are common in critically ill children
- Nonconvulsive seizures among critically ill children: Look and you shall find
- Evaluation of CT Perfusion in the Setting of Cerebral Ischemia: Patterns and Pitfalls