
Abstract
SUMMARY: MR imaging automated spine survey iterative scan technique (ASSIST) provides an automated subminute, submillimeter, in-plane resolution survey of the entire spine in 2 contiguous sagittal fast gradient-echo breath-hold series with computer labeling of vertebrae and disks. The technique was prospectively tested in 13 school-aged children for a wide range of clinical indications. In all cases, imaging was successful without requiring repeated sequencing. In all but 1 patient manifesting prominent scoliosis, automated labeling was concordant with neuroradiologist assignments.
Although it is widely acknowledged that radiographic exposure should be reduced as much as possible, particularly in the sensitive pediatric population, exposure to diagnostic ionizing radiation continues to increase.1 MR imaging holds promise for improved noninvasive, radiation-free screening and evaluation of children. However, traditionally long MR imaging scan times, occasionally necessitating sedation with attendant risks, and related high examination costs have limited its more widespread usefulness and substitution for conventional radiographs and CT scans.2-4 An automated spine survey iterative scan technique (ASSIST) to provide subminute, submillimeter, in-plane resolution MR imaging screening of the entire spine with computer labeling of disks and vertebrae has shown promise in adults5 and has been recently modified to serve a broader population and wider range of imaging parameters.6 We tested the modified ASSIST in school-aged children as a rapid nonionizing alternative to radiographs or CT scanning and as an optimized localizer for more focused MR imaging when required.
Materials and Methods
We obtained institutional review board approval and informed parental consent and child assent. The entire spine was autoimaged at 3T in 2 contiguous 35-cm FOV sagittal stations (11 sections, 4-mm skip 1 mm), using out-of-phase fast gradient-echo (FGE) sequencing (TR, 57 ms; TE, 1.4 ms; flip angle, 30°; bandwidth, ± 62.5 kHz; matrix, 512 × 352; breath-hold, 21 sec), zoom gradients, and a commercial 8-channel spine array coil (GE Healthcare, Waukesha, Wis). Sequencing provided 70-cm (SI), 35-cm anteroposterior, and 5.4-cm left to right coverage. Between March and July 2007, a total of 13 school-aged subjects (age range, 7–18 years; mean age, 13 years, 5 females; 8 males; and height range, 3 feet 6 inches [107 cm; Fig 1C] to 6 feet 1 inch [185 cm; Fig 1E]) were studied with ASSIST for a wide range of indications including scoliosis (Figs 1D, G). In 9 subjects, iterative decomposition of water and fat with echo asymmetric and least-squares estimation (IDEAL)7 (Fig 2) and/or limited conventional spine sequencing was also performed. Images were independently evaluated by a neuroradiologist (K.L.W.) with Certificates of Added Qualification and run through ASSIST analysis software5,6 for automated vertebral and disk numbering.

Midline sagittal ASSIST (from left to right). A, A 7-year-old boy with ADHD demonstrating mild motion artifacts. B, A 9-year-old boy with Asperger syndrome. Diaphragmatic contour (arrow) is well defined, suggesting good breath-hold. C, A 10-year-old girl with developmental delay and short stature. Diaphragmatic contour (arrow) is well defined, suggesting good breath-hold. D, A 12-year-old girl with prominent scoliosis. Examination resulted in autolabeling failure. E, A 16-year-old adolescent boy with mild Scheuermann disease at T6-T8 (arrows) and L4 superior endplate deformity (arrow). F, A 17-year-old adolescent boy with lumbarized S1 (L6) vertebrae (closed arrow) and enlarged pituitary gland (open arrow). G, An 18-year-old woman with mild kyphoscoliosis.

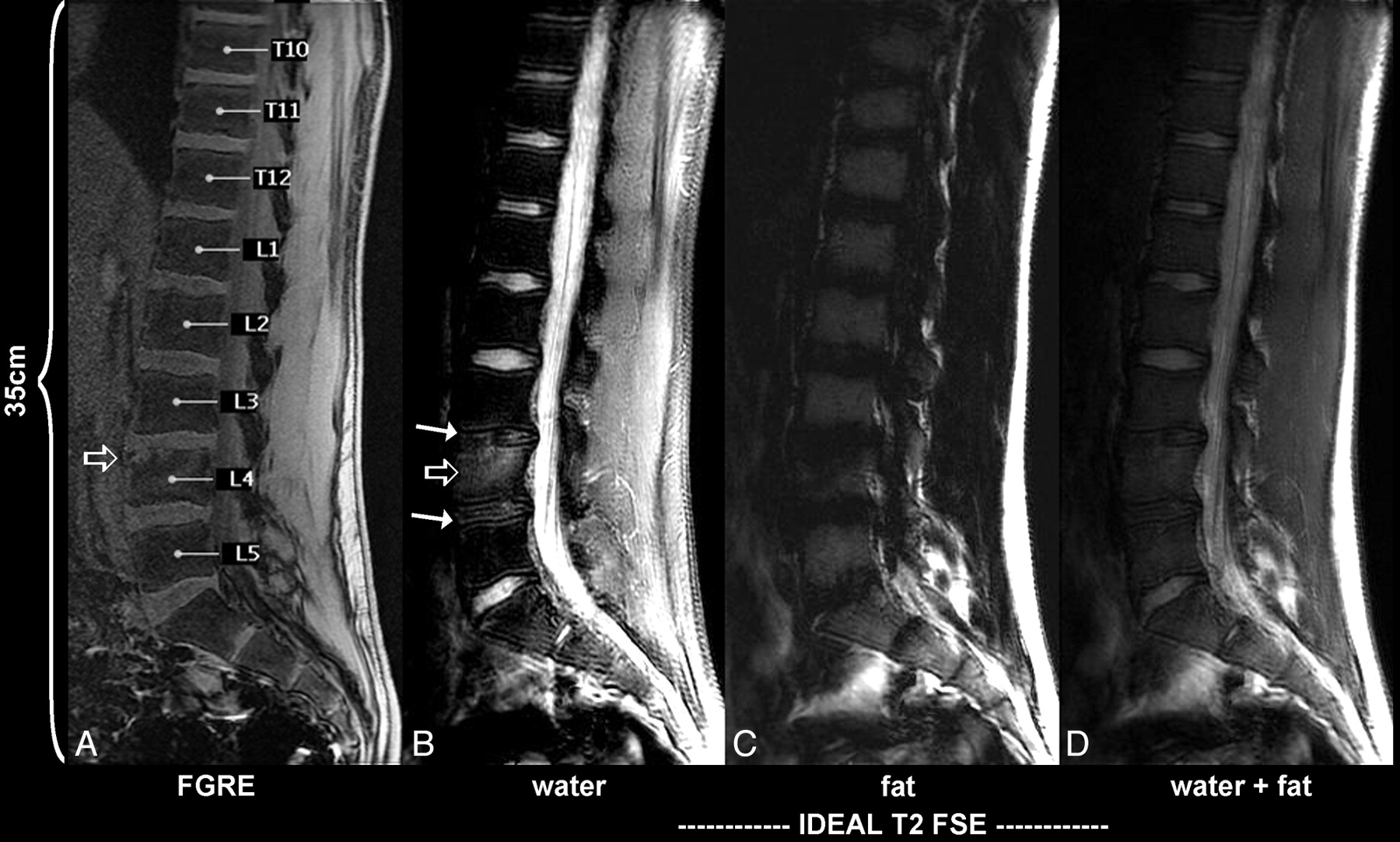
Midline sagittal ASSIST lower station in a 16-year-old adolescent boy (same subject as in 1E). From left to right, autolabeled out-of-plane FGE (TR, 57 ms; TE, 1.4 ms; flip angle, 30°; bandwidth, ± 62.5 kHz; matrix, 512 × 352; breath-hold, 21 sec), IDEAL T2 FSE (TR, 2050 ms; TE, 61.7 ms; ETL, 9; bandwidth, ± 25 kHz; matrix, 512 × 288; 3.33 minutes).
Results
In 12 (92.3%) of 13 total spine studies, computer ASSIST labeling was concordant with independent neuroradiologist assignments, including 2 children exhibiting 25, rather than the typical 24, mobile presacral vertebrae. In 1 of these 2 children, who had undergone ASSIST as part of a rapid total brain and spine survey, pituitary enlargement was retrospectively appreciated (Fig 1F). This, however, was far better depicted and characterized on rapid brain examination (not illustrated), with subsequent laboratory testing leading to the unsuspected diagnosis of primary hypothyroidism with secondary reactive pituitary hyperplasia.
ASSIST labeling failed in the child with greatest scoliosis (37° dextrocurvature centered at T6 [Fig 1D]) but was successful in all other cases. For example, in an 18-year-old woman, ASSIST detected 16° dextroscoliosis, maximal at T12-L1, and 35° kyphosis centered at T7. The kyphosis was measured from the superior endplate of T4 to the inferior endplate of T9 (Fig 1G). Motion artifacts, albeit mild, were most notable in the youngest child, a 7 year and 8-month-old boy with attention deficit/hyperactivity disorder (ADHD; Fig 1A). In contradistinction, the next 2 youngest subjects, ages 9 years 6 days (Figs 1B and 3) and 10 years 8 days (Fig 1C), exhibited limited motion and demonstrated successful breath-holding, the breath-holding documented by sharp diaphragmatic contours (Figs 1B, C, arrows). As subjectively assessed by the neuroradiologist, good contrast was achieved between the vertebrae, disks, CSF, and neural tissue (Figs 1A–G).

Left of midline sagittal ASSIST upper station (10 mm) in a 9-year-old boy (same subject as in 1B). Note vertically oriented neurocentral synchondrosis visualized on this image from T2 (upper arrow) to T11 (lower arrow).
Developmental changes were evident throughout the age spectrum studied, with short stature and reduced vertebral dimensions8 noted in a 10-year-old girl (Fig 1C) with a bone age of 6 years 2 months documented by conventional radiography (not illustrated). The neurocentral synchondrosis, a cartilaginous growth plate closing last in the midthoracic region,9 was best appreciated in our second youngest subject as a vertically oriented line spanning contiguous thoracic vertebrae (Fig 3) and exhibiting high signal intensity relative to the marrow signal intensity, the latter suppressed by out-of-phase imaging to a greater degree than in other preadolescent subjects (Fig 1B versus Figs 1A, C).
Where performed, further characterization of pathologic features was achieved with T2-weighted fast spin-echo IDEAL ASSIST as illustrated by the case of a 16-year-old adolescent boy presenting with lower back pain (Figs 1E, 2). Although mild lower thoracic Scheuermann disease and an anterior L4 superior endplate deformity can be appreciated on FGE ASSIST, L3–4 and L4–5 disk desiccation and L4 marrow edema are more readily identified and characterized with IDEAL sequencing, particularly the water-decomposed image (Fig 2B).
Discussion
For automated scan prescription simplicity and ease in directly comparing children of different ages and stature, all parameters including FOV were kept the same. However, if desired, smaller children might be more effectively studied with proportionately smaller FOVs for greater in-plane resolution or for reduced scan time, with phase-encoding steps proportionately reduced. The reduced scan time option might prove particularly advantageous for younger children who have limited breath-hold capacity. If the child is adequately positioned and is not significantly scoliotic, sagittal section thickness might also be reduced and still provide full left-to-right spine coverage with 11 sections. In addition, total spine surveys in children under 4 feet (122 cm; Figs 1A, C) might be possible with a single large FOV (eg, 48 cm), rather than 2 contiguous 35-cm stations as described herein. Reducing anteroposterior phase-encoding steps to 256 and anteroposterior FOV to 25 cm might then afford a submillimeter, in-plane resolution total spine survey in a single 16-second breath-hold.
Our study demonstrates that children as young as 9 years can hold their breath on demand and remain still within the magnet for 2 consecutive 21-second intervals. The lower age limit for successful 21-second breath-holding, however, is indeterminate because our study size was small and the youngest subject (age 7 years) had untreated ADHD and demonstrated significant motion artifacts on the brain MR imaging screen preceding ASSIST.
Although rapid, opposed-phase FGE ASSIST may provide indeterminate tissue characterization, making it difficult, for example, to differentiate a hemangioma, which typically contains fat, from a more worrisome fatty marrow-replacing lesion because both may appear relatively hyperintense on an out-of-phase FGE sequence. In addition, depending on relative fat and water marrow content, pathologic features or anatomic structures of interest, such as the cartilaginous neurocentral synchondrosis, well depicted against a background of low signal intensity marrow (Fig 3), may be obscured or even demonstrate reversed contrast. In contradistinction to opposed-phase ASSIST, conventional T1- and T2-weighted spin-echo sequencing typically displays the synchondrosis as having relatively low signal intensity compared with bone marrow.9
To improve tissue contrast and discrimination without requiring additional sequencing or time, we have recently tested an investigational 3D dual-echo spoiled gradient-echo fat-water decomposition breath-hold version of ASSIST10,11 (ASSIST DE) in adults.6 Given promising results in adults and our success with breath-hold ASSIST in school-aged children, we are now exploring ASSIST DE in the school-aged pediatric population.
Conclusions
ASSIST is a promising MR imaging technique for pediatric imaging, affording a rapid, automated, high-resolution survey of the entire spine with computer labeling of the vertebrae and disks. More comprehensive testing is warranted.
Acknowledgments
We thank GE Healthcare for providing the investigational IDEAL software. We also thank the dedicated staff at WestImage, especially Joy Bohnert, RTR (MR), for her helpful expertise in ASSIST and IDEAL sequence implementation. Illustrations by Chris Malott.
Footnotes
K.L.W. and J.L.W. have proprietary interests in ASSIST, US Patent Pending.
This study was funded by the State of Ohio, Childcare Grant.
Previously presented at: Annual Meeting of the American Society of Neuroradiology, June 3, 2007, Chicago Ill.
References
- Received August 25, 2008.
- Accepted after revision October 28, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}