
SUMMARY:
A 7-year-old boy presented with angle-closure glaucoma, initially presumed to be idiopathic. A ciliary body mass was later detected on MR imaging, suggestive of medulloepithelioma but pathologically proved to be diffuse infiltrating retinoblastoma. We discuss the patient management and review the literature, with emphasis on the role of CT and MR imaging in evaluating pediatric angle-closure glaucoma and in influencing the management of patients with retinoblastoma and medulloepithelioma.
Retinoblastoma is the most common intraocular tumor in children. Ninety-five percent of cases occur in patients younger than 5 years with a mean age of 18 months.(1) Medulloepithelioma occurs in older children, with mean age of 4 years.(2,3) As opposed to retinoblastoma, which typically arises in the sensory retina, medulloepithelioma almost always occurs in the ciliary body and is the primary consideration for an anterior segment mass in pediatric patients.(1–3)
The most frequent alternative diagnosis for a pediatric anterior segment mass is diffuse infiltrating retinoblastoma. Compared with conventional retinoblastomas, this variant typically occurs in older pediatric patients, overlapping the age group of medulloepithelioma.(2,4,5)
Given that both can elevate intraocular pressures, imaging plays an important role in identifying neoplastic etiologies in children with angle-closure glaucoma. Furthermore, MR imaging defines the local extent of such lesions, profoundly impacting management.
Case Report
A 7-year-old boy presented with left orbital pain, decreased vision, and findings of cataracts and angle-closure glaucoma with unrevealing funduscopic examination and orbital sonography. Six months after undergoing an Ahmed anterior chamber shunt surgery procedure for presumed idiopathic angle-closure glaucoma, he developed a white anterior chamber mass, initially believed to be a hypopyon from presumed granulomatous uveitis. He then underwent a nonconjunctival-disrupting procedure with fine-needle aspiration. Cytologic analysis revealed small malignant cells with scant cytoplasm, positive for synaptophysin and chromogranin immunostains, yielding a preliminary diagnosis of retinoblastoma.
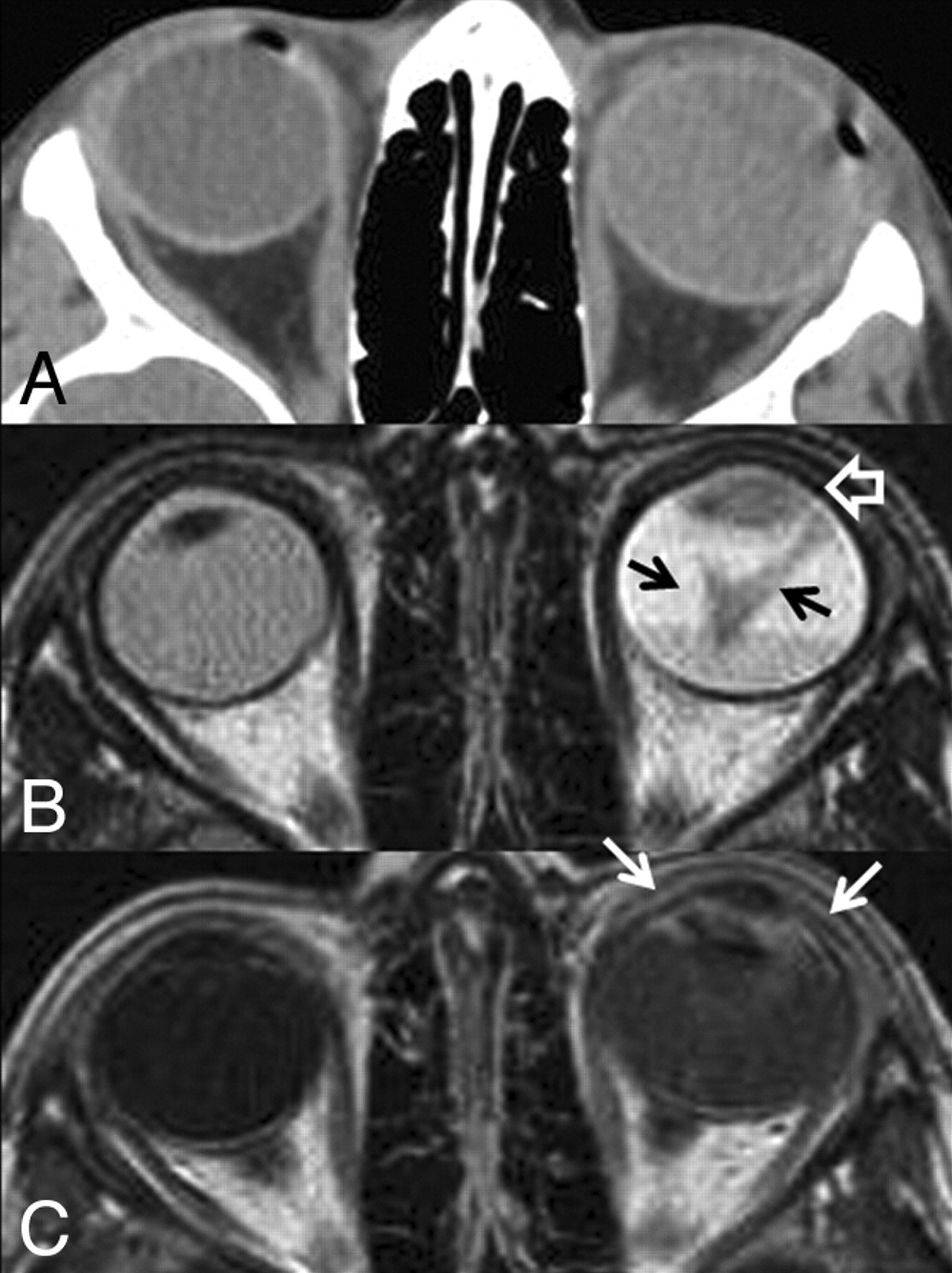
CT and MR imaging of the orbits demonstrated a noncalcified diffuse infiltrating mass involving a detached retina and anterior segment in the left globe (Fig 1), suggesting either advanced medulloepithelioma or diffuse infiltrating retinoblastoma. The patient subsequently underwent enucleation, providing a final pathologic diagnosis of retinoblastoma (Fig 2).

A, CT scan of the orbits. The left globe is asymmetrically enlarged and is hyperattenuating compared with the contralateral right globe, reflective of glaucoma and total retinal detachment, respectively. No calcifications are present. B, Axial T2-weighted MR image. There is total retinal detachment with a large fluid-fluid level. The detached retina is irregular and diffusely thickened (black arrows), and there is an irregular intermediate-signal-intensity mass involving the ciliary body and iris circumferentially (open white arrow). C, Axial T1-weighted postcontrast MR image. There is diffuse enhancement of the thickened detached retina and the anterior segment mass (white arrows). This constellation of findings is consistent with diffuse infiltrating retinal neoplasm extending into the anterior ocular segment. There is no evidence of optic nerve invasion or extrascleral extension.

Histologic section of the enucleated left globe. A, Photomicrograph (hematoxylin-eosin [HE] stain) of the whole-mount specimen at original magnification ×2. The ciliary body is diffusely infiltrated with neoplastic cells with round basophilic nuclei. The cells form rosettes around central lumens, known as Flexner-Wintersteiner rosettes, which are characteristic of retinoblastoma. B, Photomicrograph (HE stain) of the whole-mount specimen at original magnification ×40. The neoplastic cells have round basophilic nuclei with scant cytoplasm and are arranged in a rosette around a central lumen.
Discussion
Glaucoma in the first decade of life should be thoroughly evaluated for an ocular neoplasm. Up to 17%–22.8% of patients with retinoblastoma have increased intraocular pressures typically due to iris neovascularization.(6,7) However, with diffuse infiltrating retinoblastoma subtypes, glaucoma can result from neoplastic seeding of the trabecular meshwork in the anterior chamber, causing outflow obstruction of the aqueous humor.(6)
Retinoblastoma has 4 different growth patterns: endophytic growth toward the vitreous, exophytic growth toward the choroid, mixed exophytic and endophytic growth (most common), and diffuse infiltrating growth. Diffuse infiltrating retinoblastoma is rare, accounting for only 1%–2% of all cases,(1,8) and is characterized by plaquelike thickening of the retina without a discrete mass lesion. Patients often present when pseudoinflammatory complications occur once the lesion infiltrates into the anterior segment, and the condition may be misdiagnosed as uveitis and iritis.(5,8,9) When tumor involves the ciliary body, it can mimic a hypopyon, which can delay the diagnosis if anterior chamber paracentesis or tissue sampling is not performed.(5)
Secondary glaucoma from iris neovascularization actually occurs more frequently with medulloepithelioma, occurring in 60% of cases.(3) Medulloepitheliomas are typically malignant nonhereditary embryogenic neoplasms of the medullary epithelium almost always occurring in the ciliary body.(2,3) This neoplasm is divided into nonteratoid (60%) and teratoid (40%) histologic subtypes. Teratoid medulloepitheliomas are composed of heteroplastic tissue elements, which can include hyaline cartilage, skeletal muscle, and brain tissue.(2)
Anterior segment retinoblastoma and medulloepithelioma are nearly indistinguishable on imaging. Compared with conventional retinoblastomas, diffuse infiltrating retinoblastoma has an atypical imaging appearance, reflective of its growth pattern. On MR imaging, there is often retinal detachment without a discrete mass lesion. Diffuse irregular and nodular thickening of the detached retinal leaflets is evident, with abnormal enhancement that often extends to the anterior ocular segment (Fig 1).(8)
CT is not helpful in distinguishing these neoplasms because both may or may not calcify. Although 95% of conventional retinoblastomas calcify, diffusely infiltrating subtypes tend not to calcify.(1,5,8) Most medulloepitheliomas also do not calcify; however, calcifications do occur in 30% of teratoid subtypes (Fig 3).(2,3) Both neoplasms are hyperintense to the vitreous on T1-weighted images and hypointense on T2-weighted images and enhance either uniformly or heterogeneously.(2) The most reliable feature for distinguishing these 2 neoplasms is location. If the mass is confined to the ciliary body, then it is most likely a medulloepithelioma.(1) Anterior segment retinoblastomas typically have diffuse infiltration of the retina, iris, and ciliary body.(1,8) However, advanced cases of medulloepithelioma can infiltrate the retina and cause retinal detachment, so anterior-segment tumors that show diffuse infiltration cannot be reliably distinguished radiologically.(1)

Teratoid medulloepithelioma. A, Noncontrast axial CT scan shows a densely calcified mass of the ciliary body in the anterior segment of the right globe. Teratoid medulloepitheliomas can contain dystrophic calcifications due to the presence of hyaline cartilage tissue elements. B, Axial T1-weighted fat-saturated postcontrast MR image shows an enhancing mass of the ciliary body corresponding to the area of calcification on the CT scan. The mass is confined to the ciliary body; therefore, medulloepithelioma is more likely than diffuse infiltrating retinoblastoma. Alternative diagnoses for a ciliary body mass in pediatric patients include pyogenic granuloma, juvenile xanthogranuloma, mesoectodermal leiomyoma, and ciliary body cyst.
The role of imaging is not necessarily to make a specific pathologic diagnosis but rather to confirm the presence of an anterior segment mass and determine the local extent of the lesion. The presence of extrascleral or optic nerve invasion has significant prognostic and therapeutic implications for both retinoblastoma and medulloepithelioma. Tumors that are confined to the globe have excellent prognoses with 90%–95% 5-year survival after enucleation or focal therapy.(1,2,10) The globe is devoid of lymphatic tissue; therefore, metastatic disease is rare without episcleral or optic nerve involvement. When either neoplasm extends into the conjunctiva or extrascleral orbital soft tissues, the rate of metastatic disease and recurrence increases dramatically.(1,10–12) Metastatic disease for both neoplasms most commonly presents with diffuse subarachnoid seeding, resulting from optic nerve invasion, specifically with extension posterior to the lamina cribrosa.(12) On MR imaging, abnormal optic nerve enhancement that is contiguous with the tumor is indicative of postlaminar tumor infiltration.(10) Although limited in sensitivity for microscopic optic nerve invasion, this finding is 100% specific.(10) Patients with episcleral or optic nerve extension have poor overall prognoses and are often treated with orbital exenteration and chemotherapy as opposed to enucleation alone.(12)
References
- Received December 27, 2008.
- Accepted after revision January 28, 2009.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}