
Abstract
SUMMARY: Coiling is increasingly used as treatment for intracranial aneurysms with favorable short-term outcome. Concern exists about long-term reopening and the inherent risk of recurrent subarachnoid hemorrhage (SAH), and long-term imaging follow-up is advocated. It is unknown for how long and how often coiled aneurysms need to be followed and what subgroups carry a higher or lower risk for reopening. Recently, new data have become available that concern the designation of an optimal long-term follow-up protocol. Three studies focused on a special subgroup, the coiled aneurysms that are adequately occluded at 6 months. This subgroup comprises about 80% of all coiled aneurysms. In these aneurysms, the risk of reopening that needs retreatment during the next 5–10 years is very low. In addition, the risk of recurrent SAH is almost zero, even lower than that after clipping. Within the first 5 years after coiling, the incidence of the development of de novo aneurysms or enlargement of existing untreated aneurysms is low, with an extremely low risk of recurrent SAH from these aneurysms. These data suggest that aneurysms that are adequately occluded at 6 months after coiling, in general, do not need prolonged imaging follow-up in the next 5–10 years. More data are needed to identify possible subgroups with adequately occluded coiled aneurysms at 6 months that behave differently on longer follow-up, such as giant aneurysms, partially thrombosed aneurysms, or patients with a positive family history.
Endovascular treatment with coils has become an established treatment technique for both ruptured and unruptured intracranial aneurysms.1,2 Coiling has several shortcomings. Not all aneurysms can be occluded completely at first treatment; this possibility leaves the patient at risk for early recurrent hemorrhage in case of a recently ruptured aneurysm. Another drawback is the potential for reopening with time of an initially adequately occluded aneurysm as a result of coil compaction, aneurysm growth, or dissolution of an intraluminal thrombus. Reopening occurs in approximately 20% of coiled aneurysms, and half of these aneurysms are retreated. The remaining aneurysms are not retreated because of unfavorable geometry for additional coiling or because retreatment is not judged to be indicated in the clinical context.
Possible risk factors for reopening of a coiled aneurysm with time are large aneurysm size, the presence of intraluminal thrombus, low packing attenuation, initial incomplete occlusion, longer follow-up, and a wide neck. From published data, the robustness and power of the separate contributions of these risk factors remain obscure due to differences in study design, aneurysm selection, and method of follow-up.3–12 As a consequence, it is unknown for how long and how often coiled aneurysms need to be followed and whether certain subgroups carry a higher or lower risk for reopening. Recently, several long-term follow-up studies of patients with coiled intracranial aneurysms have been published that contribute to defining an optimal long-term follow-up protocol for individual patients to prevent future subarachnoid hemorrhage (SAH). Most of these studies come from the Netherlands, a small and densely populated country with a well-organized health care system, which allows tracing and recruiting patients for long-term follow-up relatively easily.
Why Patients with Coiled Aneurysms Need Imaging Follow-Up
The most important reason for imaging follow-up is the fact that reopening after coiling has a 20% frequency. An incompletely occluded aneurysm exposes the patient to a risk for recurrent SAH in the long term, and retreatment is advocated.
The second reason for imaging follow-up is the increasing awareness that an aneurysm might be an expression of a general disease of the intracranial arteries and not a once-in-a-lifetime event. Many patients presenting with an aneurysm have multiple aneurysms. With modern 3D imaging, these additional aneurysms are detected with increasing frequency.13 When possible, additional aneurysms are treated, but many are not, mostly because of small size and a presumably low rupture risk. However, these small aneurysms can grow; and because the risk of rupture increases with size, prolonged imaging follow-up is advocated to detect growth. In addition, on diseased intracranial arteries, new aneurysms can develop later that can also become a source of recurrent SAH.
Little is known about the pace of growth of untreated additional aneurysms and the frequency and timing of the development of new aneurysms and, thus, the need for and timing of long-term imaging follow-up for these aneurysms.
Timing of Reopening of Coiled Aneurysms and Implication for Timing of Follow-Up
An important issue is the timing of the occurrence of reopening after coiling. Do all reopenings develop within the first 6 months or can aneurysms still reopen after a longer period of stable adequate occlusion? Moreover, can an aneurysm that is adequately occluded at 6 months still reopen at a later point in time and, if yes, at what point in time?
In several studies, more first-time aneurysm recurrences after coiling were found with longer follow-up during the first years after coiling, and prolonged imaging follow-up was recommended to detect more first-time recurrences.4–6,12 At closer look, interpretation of these studies was impeded by a wide variety in time intervals of follow-up angiography, so late-detected reopening had possibly developed earlier. In contrast to the conclusion of these studies, in a series of 126 patients with fixed angiographic follow-up intervals at 6 and 18 months after coiling, all reopened aneurysms were found at 6-month angiography.3 Aneurysms that were adequately occluded at 6 months remained so at 18 months, and no first-time recurrences were detected after 6 months.
The discrepancies of the conclusions in these follow-up studies are confusing in clinical practice: If more first-time recurrences are found with longer follow-up, prolonged imaging follow-up would be mandatory to detect these late-onset recurrences. On the other hand, if adequately occluded aneurysms at 6 months do not reopen later, extended follow-up is not necessary. To elucidate this problem, long-term follow-up studies have been performed focusing on patients with coiled aneurysms that were adequately occluded at 6-month angiographic follow-up. Sprengers et al14 selected, from a cohort of 607 patients with 661 aneurysms coiled between 1994 and 2002, 104 patients with 111 adequately occluded aneurysms at 6 months. These 104 patients underwent 3T MR angiography (MRA) 5–11 years after coiling to assess the stability of adequate aneurysm occlusion (LOTUS I). Three of 111 aneurysms showed minor reopening, and 1 aneurysm (that initially contained intraluminal thrombus) showed major reopening and was retreated. These findings indicate that when an aneurysm is adequately occluded at 6 months, the chance of a reopening needing retreatment in the next 5–11 years is very low, and they confirmed the findings of the initial study.3 In the meantime, the study continues. Another 160 patients have been recruited for LOTUS II, and preliminary results are in concordance with LOTUS I.
In another study, Schaafsma et al15 assessed the incidence of recurrent SAH in the long term after coiling in 283 patients (overlapping the patients included in LOTUS I) with coiled ruptured aneurysms that were adequately occluded at 6 months. The incidence of recurrent SAH was compared with the incidence of recurrent SAH after clipping of a ruptured aneurysm. After a mean follow-up of 6.3 years, 1 patient had a recurrent SAH from the coiled aneurysm (0.4%) and 2 patients had a possible recurrent SAH. Within the first 8 years after coiling, the cumulative incidence of recurrent SAH was 0.4%. This was significantly lower (hazard ratio, 0.2) than the cumulative incidence of 2.6% that was found in a cohort of 748 patients with ruptured aneurysms that were clipped.
These studies indicate that in the subgroup of patients with coiled aneurysms that are adequately occluded at 6 months, the risk of first-time reopening needing retreatment in the first 5–10 years after coiling is extremely low and the risk of recurrent SAH was 5 times lower than that after clipping. For this large subgroup (approximately 80% of all aneurysms with imaging follow-up), prolonged imaging follow-up is not necessary.
The data also show that virtually all aneurysm reopenings develop in the first 6 months after coiling.
Development of De Novo Aneurysms and Growth of Additional Aneurysms
Patients with intracranial aneurysms are at risk for development of de novo aneurysms later in life. Recently, several large studies assessed the incidence of de novo aneurysm formation, growth of additional aneurysms, and recurrent SAH in patients with treated aneurysms.16–23 Several studies used CT angiography to detect de novo aneurysm formation and growth of existing untreated aneurysms in the long term after surgical clipping of a ruptured aneurysm. In a study of 610 patients,18 after a mean interval of 9.1 years, 19 definitive de novo aneurysms were found in 14 patients and 42 probable de novo aneurysms, in 34 patients. This finding corresponds to a cumulative incidence of de novo aneurysm formation between 2.3% and 10% and an annual incidence between 0.37% and 1.20%. Of 19 de novo aneurysms, 18 (95%) were <5 mm. In the same study, 4 of 18 (22%) existing aneurysms had enlarged slightly in the first 5 years of follow-up, and 13 of 53 (25%), in the first 10 years. In another study,16 the incidence of recurrent SAH was assessed in 752 patients with previously clipped ruptured aneurysms. In the first 10 years after initial SAH, the cumulative incidence of recurrent SAH was 3.2%. Of the 18 patients with recurrent SAH in this study, the SAH was caused by a regrowth at the clip site in 4, by a de novo aneurysm in 10 (4 certain and 6 possible de novo), and by an additional aneurysm in 4. The mean interval between the initial SAH and the recurrence was 6.5 years (range, 0.2–17 years). Within the first 3 years after clipping, no recurrent SAH from a de novo or regrowth aneurysm was found.
These studies demonstrate a relatively high cumulative incidence of 2.3%–10% of de novo aneurysm formation in the first 10 years. Although more de novo aneurysms were found with longer follow-up, the timing of the first presence of these aneurysms remains unknown. A subgroup of 65 patients with exact 5-year MRA follow-up after coiling was selected from LOTUS, to assess whether de novo aneurysms develop in the first 5 years after coiling.24 In 65 patients, 1 small de novo aneurysm had developed within the first 5 years. Of 19 additional untreated aneurysms, 1 had grown slightly and 18 were unchanged. No therapy for these aneurysms was judged to be indicated. In another MRA follow-up study of 26 patients at a mean of 4.1 years after therapeutic carotid artery occlusion, no de novo aneurysms were found despite increased hemodynamic stress in the circle of Willis after carotid occlusion.25
The results of these studies indicate that in the first 5 years after coiling, both the risk of de novo aneurysm formation and the risk of the growth of existing untreated aneurysms are very low. As a consequence, the risk of SAH from such aneurysms is extremely low. It seems safe to refrain from imaging follow-up to detect de novo aneurysms and growth of existing aneurysms in the first 5 years.
The Subgroup of Adequately Occluded Aneurysms at 6 Months and the Next 5 to 10 Years
Patients with aneurysms that are adequately occluded at 6 months after coiling (approximately 80% of all coiled aneurysms) apparently form an important subgroup. In the first 5–10 years after coiling, the coiled aneurysm remains stably occluded and does not rebleed. In addition, in all patients with aneurysms, the risk of de novo aneurysm formation and significant enlargement of additional untreated aneurysms is low, with, subsequently, an extremely low risk of SAH from these aneurysms. This low risk seems particularly true for the first 5 years and probably also for the first 10 years. Therefore, prolonged imaging follow-up within the first 5–10 years after coiling does not seem beneficial in patients with aneurysms that are adequately occluded at 6 months, both in terms of preventing SAH and for detection of aneurysms that need treatment.
In clinical practice, this implies that the first imaging follow-up at 6 months is a crucial point in time: When the coiled aneurysm is adequately occluded, the patient may be considered cured. Whether patients might benefit from screening beyond the 5- to 10-year interval is not yet elucidated. A consideration in offering very late follow-up imaging is that from the patient's perspective, screening may work in a 2-sided manner: In patients with fear of new aneurysms, it may increase quality of life when no such aneurysms are found but it may have a negative impact when new aneurysms are detected that remain untreated.22
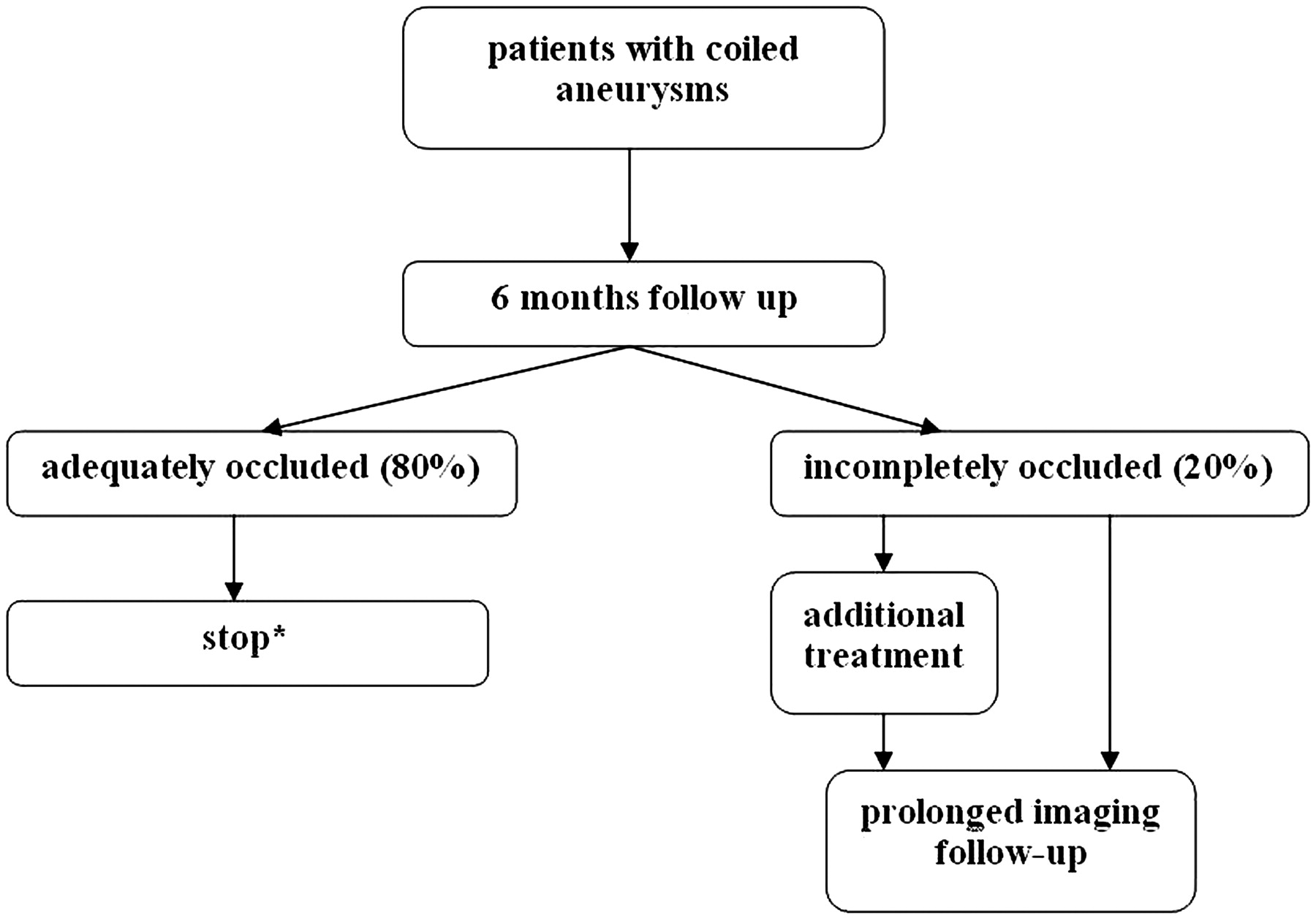
Although the results of the recent studies suggest that patients with adequately occluded aneurysms do not need prolonged follow-up, not enough data are available and larger studies, preferably with fixed follow-up intervals, are needed to identify subgroups of patients with adequately occluded coiled aneurysms at 6 months that behave differently and might benefit from screening within or at 5 years. For example, partially thrombosed aneurysms may reopen for the first time beyond the 6-month interval.8,11,26 Perhaps, also very large and giant aneurysms should be followed further despite adequate occlusion at 6 months. In these subgroups, regular MRA follow-up (every 1–3 years) may be considered. More frequent and prolonged follow-up might also be considered in patients with increased risk, such as young patients with multiple aneurysms, patients with a positive family history, or patients with proved growth of additional aneurysms. A proposed imaging follow-up scheme is provided in Fig 1.

Proposed imaging follow-up scheme after coiling of intracranial aneurysms. *For possible exceptions, see text.
Conclusions
For the large subgroup of patients with coiled aneurysms that are adequately occluded at 6 months, prolonged imaging follow-up is not needed because the risk of SAH from reopening of the coiled aneurysm, development of de novo aneurysms, or growth of existing untreated aneurysms is extremely low. Further studies are needed to identify subgroups of aneurysms that behave differently.
References
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
- Article
- Abstract
- Why Patients with Coiled Aneurysms Need Imaging Follow-Up
- Timing of Reopening of Coiled Aneurysms and Implication for Timing of Follow-Up
- Development of De Novo Aneurysms and Growth of Additional Aneurysms
- The Subgroup of Adequately Occluded Aneurysms at 6 Months and the Next 5 to 10 Years
- Conclusions
- References
- Figures & Data
- Info & Metrics
- Responses
- References
Related Articles
Cited By...
- Voxel based analysis of recurrence dynamics in intracranial aneurysms after coiling
- Inter- and Intrarater Agreement on the Outcome of Endovascular Treatment of Aneurysms Using MRA
- Clinical and Imaging Follow-Up of Patients with Coiled Basilar Tip Aneurysms Up to 20 Years
- Temporal Evolution of Susceptibility Artifacts from Coiled Aneurysms on MR Angiography: An In Vivo Canine Study
- An approach to recurrent aneurysms following endovascular coiling
- Counterpoint: Has the Last Word Been Said?