
Abstract
BACKGROUND AND PURPOSE: Methylation of the MGMT gene promoter is associated with a favorable prognosis in adult patients with GBM treated with TMZ. We determined the incidence of pseudoprogression according to the MGMT methylation status and the potential value of DSC perfusion MR images for predicting pseudoprogression.
MATERIALS AND METHODS: New or enlarged enhancing lesions after CCRT in adult patients with newly diagnosed GBMs were prospectively assessed by measuring their rCBV by using DSC perfusion MR images. Tumor tissue was assayed to determine MGMT promoter methylation status. All patients were regularly followed up at an interval of 2 months by MR images, including DSC perfusion MR images.
RESULTS: Ninety eligible patients were enrolled in this study. After CCRT, new or enlarged enhanced lesions were found in 59 of 90 patients, which were subsequently classified as pseudoprogression (26 patients, 28.9%) and real progression (33 patients, 36.7%). Overall, there was a significant difference in the mean rCBV between pseudoprogression and real tumor progression (P = .003). The ROC curve revealed that an rCBV ratio >1.47 had an 81.5% sensitivity and a 77.8% specificity. The unmethylated MGMT promoter group had a significant difference of mean rCBV between pseudoprogression and real progression (P = .009), though the methylated MGMT promoter group had no significant difference (P = .258).
CONCLUSIONS: The current study suggests that rCBV measured by DSC perfusion MR images has a differential impact on the predictability of pseudoprogression in patients with GBM.
Abbreviations
- CBV
- cerebral blood volume
- CCRT
- concomitant chemoradiotherapy
- CI
- confidence interval
- Cum
- cumulative
- DSC
- dynamic susceptibility-weighted contrastenhanced
- FA
- flip angle
- FLAIR
- fluid-attenuated inversion recovery
- GBM
- glioblastoma
- MGMT
- O6-methylguanine-DNA methyltransferase
- MSP
- methylation-specific polymerase chain reaction
- O6
- oxygen-6
- OS
- overall survival
- pseudo
- pseudoprogression
- pts
- patients
- rCBV
- relative cerebral blood volume
- ROC
- receiver operating characteristic analysis
- TMZ
- temozolomide
- WHO
- World Health Organization
The prognosis for patients with GBM remains dismal despite multidisciplinary treatment approaches. Establishment of therapeutic strategies is entirely dependent on the interpretation of MR imaging findings as well as clinical manifestations. Because of recent advances in the diagnostic techniques, new or progressive enhancing lesions on MR images demonstrating a transient increase in tumor enhancement without real progression, so-called pseudoprogression, after CCRT have been widely recognized.1–9 Pseudoprogression can spontaneously decrease in size or stabilize without additional treatments without developing neurologic symptoms. New or enlarging enhanced lesions after CCRT, suggesting either real tumor progression or pseudoprogression and affecting 20%–40% of all treated lesions, constitute a clinically relevant diagnostic dilemma in patients with newly diagnosed GBMs.
Currently, the validity of progression-free survival as the primary end point in many clinical trials and eligibility in salvage treatment trials have been limited because of erroneous interpretation of the pseudoprogression.10 Numerous phase II studies for recurrent gliomas included subjects who would be proved to have pseudoprogression, not real progression. In addition, differentiation between pseudoprogression and real progression is very critical for making decisions on future therapy or for predicting the prognosis in clinical practice. Therefore, for clinical trials, exclusion of pseudoprogression is essential to minimize the false-positive effect of a new drug. Several attempts have previously been made to determine whether an enlarged enhancing lesion is a true tumor progression/recurrence or pseudoprogression. In 1990, Macdonald et al11 defined the criteria for evaluating response to treatment and disease progression. They suggested that variations in the tumor-enhancing area, neurologic function, and steroid dosage should be considered in the assessment of tumor response. However, wide acceptance of this concept is difficult because of the appearance of pseudoprogression.
Recent studies have been performed on molecular properties of GBMs. Methylation of the DNA repair gene MGMT promoter region has been associated with favorable prognosis and prolonged survival in adult patients with GBM treated with TMZ.12–15 Pseudoprogression has been frequently observed in tumors with hypermethylation of the MGMT promoter gene more so than in tumors with an unmethylated MGMT promoter.14 Therefore, for the establishment of further treatment strategy, it is very essential to determine if new or progressive enhancing lesions are diagnosed as true progression or pseudoprogression according to the methylation status of the MGMT promoter gene.
The purpose of this study was to clarify the incidence of pseudoprogression during/after CCRT for newly diagnosed GBMs based on the methylation status of the MGMT promoter gene. We also assessed the predictive value of DSC perfusion MR imaging by using rCBV for differentiating pseudoprogression and real progression.
Materials and Methods
Patient Eligibility and Treatment Protocol
Adult patients with newly diagnosed GBMs were prospectively enrolled into this study if they were regularly followed up by MR imaging and were older than 20 years of age. All patients had histologically confirmed GBMs, and patients' ages ranged from 25 to 74 years. Treatment protocol included radiation therapy plus continuous daily TMZ (75 mg/m2/day) followed by 6 cycles of adjuvant TMZ (150 mg/m2 for 5 days every 28 days) after surgical resection or biopsy. A median OS was measured from the time of initial diagnosis to death or date of last follow-up. The first MR image, including DSC perfusion MR imaging, was routinely performed immediately after surgery (within the first 24–48 hours), a subsequent MR image was obtained 1 or 2 days before CCRT, and subsequent MR imaging was scheduled within 4 weeks after the end of CCRT. MR images were regularly obtained throughout the follow-up period at 2-month intervals. If the follow-up images revealed new or progressively enlarged enhancing lesions, the decision was made as to whether TMZ should be continued or an alternative chemotherapeutic regimen should be considered on the basis of various factors, such as patients' clinical manifestations, onset of development of enhancing lesions, pattern of contrast enhancement, general health status, and perfusion MR images reflecting CBV. To make an informed decision, we evaluated patients, taking into account radiologic findings and neurologic examination results, according to the criteria of Macdonald et al,11 judged by a multidisciplinary team consisting of 3 neurosurgeons, 2 neuro-oncologists, 2 radiation oncologists, and 2 neuroradiologists. In retrospectively reviewing the subsequent MR images, pseudoprogression was defined as the following: a new or progressively increasing lesion during CCRT or within 2 cycles of adjuvant treatment and either stable for at least 3–4 months or decreasing on subsequent MR images without further treatment, or histologically proved pure treatment-related necrosis at second-look surgery.
Therapeutic Strategy for the Pseudoprogression or Real Progression
Before the enrollment in this study, management for pseudoprogression or real tumor progression was based on the authors' established protocol. If pseudoprogression or real tumor progression was found within 1 or 2 cycles of TMZ maintenance therapy, pseudoprogression was considered first. For the patient without neurologic deterioration and simultaneously without an increase of cerebral blood perfusion in the lesion, no further treatment other than steroid medication was added and adjuvant TMZ therapy was continued until the MR imaging follow-up after 2 months. When the patient showed neurologic compromise consistent with radiologic abnormalities, second-look surgery or other chemotherapeutic regimens were recommended (Fig 1).

A–C, A 48-year-old woman with glioblastoma with a methylated MGMT promoter gene has a remote tumor mass on the contrast-enhanced T1-weighted image (A) immediately after the concomitant chemoradiotherapy. MR perfusion image (B) reflects a slight increase of CBV, indicating an rCBV of 1.41 compared with contralateral white matter. After 4 months' continuation of TMZ, enhancement of the lesion decreases without further treatment, which is compatible with pseudoprogression (C). D–F, A 65-year-old man with glioblastoma with unmethylated MGMT has a progressive enhancing lesion involving on the splenium (D). MR perfusion image (E) demonstrates a high increase of CBV indicating an rCBV of 4.38. After 2 months, the lesion shows stronger enhancement and more enlargements, demonstrating real tumor progression (F).
MGMT Status Assessment
Assessment of the methylation status of the MGMT promoter gene was available. MGMT methylation status was evaluated with the MSP after a nested polymerase chain reaction protocol, by using methods and assessment criteria described elsewhere.16,17 First, DNA from the primary tumor tissue specimen was subjected to bisulfite treatment, which converts unmethylated cytosine to uracil, according to the procedure of Herman et al.17 DNA samples were then purified, retreated with sodium hydroxide, precipitated with ethanol, and resuspended in water. DNA methylation patterns in the CpG islands of the MGMT gene were determined by chemical treatment with sodium bisulfite and subsequent MSP.
MR Imaging Data Acquisition and rCBV Analysis
MR imaging studies were performed with a 3T system (Achieva; Philips Healthcare, Best, the Netherlands). Imaging sequences of the brain included spin-echo T1-weighted images, fast spin-echo T2-weighted images, FLAIR images, enhanced T1-weighted images with gadobutrol (Gadovist; Bayer Schering Pharma, Berlin, Germany), and perfusion- and diffusion-weighted images. The MR imaging parameters were as follows: 500/10 ms/90°/256 × 190 (TR/TE/FA/matrix) for spin-echo T1-weighted images; 3000/80 ms/90°/240 × 190/416 × 264 (TR/TE/FA/matrix) for fast spin-echo T2-weighted images; and 11,000/125 ms/90°/240 × 190/368 × 210 (TR/TE/FA/matrix) for FLAIR images. The other parameters were the following: section thickness, 5 mm with a 1.5 mm gap; FOV, 240 × 190 mm. DSC perfusion-weighted MR images were acquired during the intravenous injection of a bolus of gadobutrol at a dose of 0.1 mmol/kg of body weight and a rate of 4 mL/s by using a single-shot gradient-echo echo-planar imaging sequence (TR/TE, 1500/35 ms; FA, 40°; FOV, 24 cm; matrix, 256 × 256; section thickness, 5 mm; intersection gap, 2 mm).
Dynamic susceptibility-weighted images were processed at a radiology workstation (ViewForum, Philips Healthcare). Color-coded rCBV maps were generated. A neuroradiologist (S.T.K) with 12 years of experience placed a region of interest of 15–20 pixels within the tumor, on areas showing the highest intratumoral rCBV ratio on the color-coded maps. The maximum rCBV ratio in intratumoral regions of interest was selected for quantitative analysis. The rCBV ratio was expressed as ratios relative to those in a region of interest of the same pixels in the contralateral normal-appearing white matter.
Statistical Analysis
A median OS was calculated by using the Kaplan-Meier method; 95% CIs were calculated by using the associated estimated standard errors. The logrank test was used to compare the OS according to the MGMT promoter methylation status. The χ2 test with a 2-sided significance level of .05 was used to compare the incidence of pseudoprogression between methylated and unmethylated MGMT groups. The mean value of rCBV was assessed and analyzed according to each group by using an independent t test. ROC curves were plotted to calculate the most discriminative cutoff point with an optimal area under the curve and to define clinically the most relevant combination of sensitivity, specificity, and accuracy. A P value < .05 was considered to indicate a statistically significant difference. Statistical analysis was performed with the use of the Statistical Package for the Social Sciences software, Version 16 (SPSS, Chicago, Illinois) and STATA software, Version 11 (StataCorp, College Station, Texas).
Results
Between July 2006 and February 2008, 90 adult patients with newly diagnosed GBMs who were treated with CCRT followed by maintenance chemotherapy according to the above-described protocol were enrolled in the present study. The MGMT promoter methylation status was assessable in 73 of 90 patients. The median follow-up period included in the analysis was 16.5 months (range, 6.2–48 months) (Table 1).
Characteristics at baseline of 90 patients with newly diagnosed glioblastoma treated with concurrent chemoradiotherapy
OS and Toxicity
A median OS of 16.9 months was observed (95% CI, 13.6–20.3 months). Patients with methylated MGMT promoter had a median survival of 19.6 months (95% CI, 13.6–25.6 months), compared with a median survival of 13.4 months (95% CI, 10.6–16.1 months) in patients with an unmethylated MGMT promoter (P = .031, Fig 2). During the concomitant therapy phase, grade 3–4 thrombocytopenia occurred in 6 patients (6.7%) and grade 1–2 lymphocytopenia occurred in 12 patients (13.3%).

OS by the presence of the MGMT promoter methylation status (A) and by the presence of pseudoprogression or early tumor progression (B).
Evaluation of Pseudoprogression/Real Tumor Progression
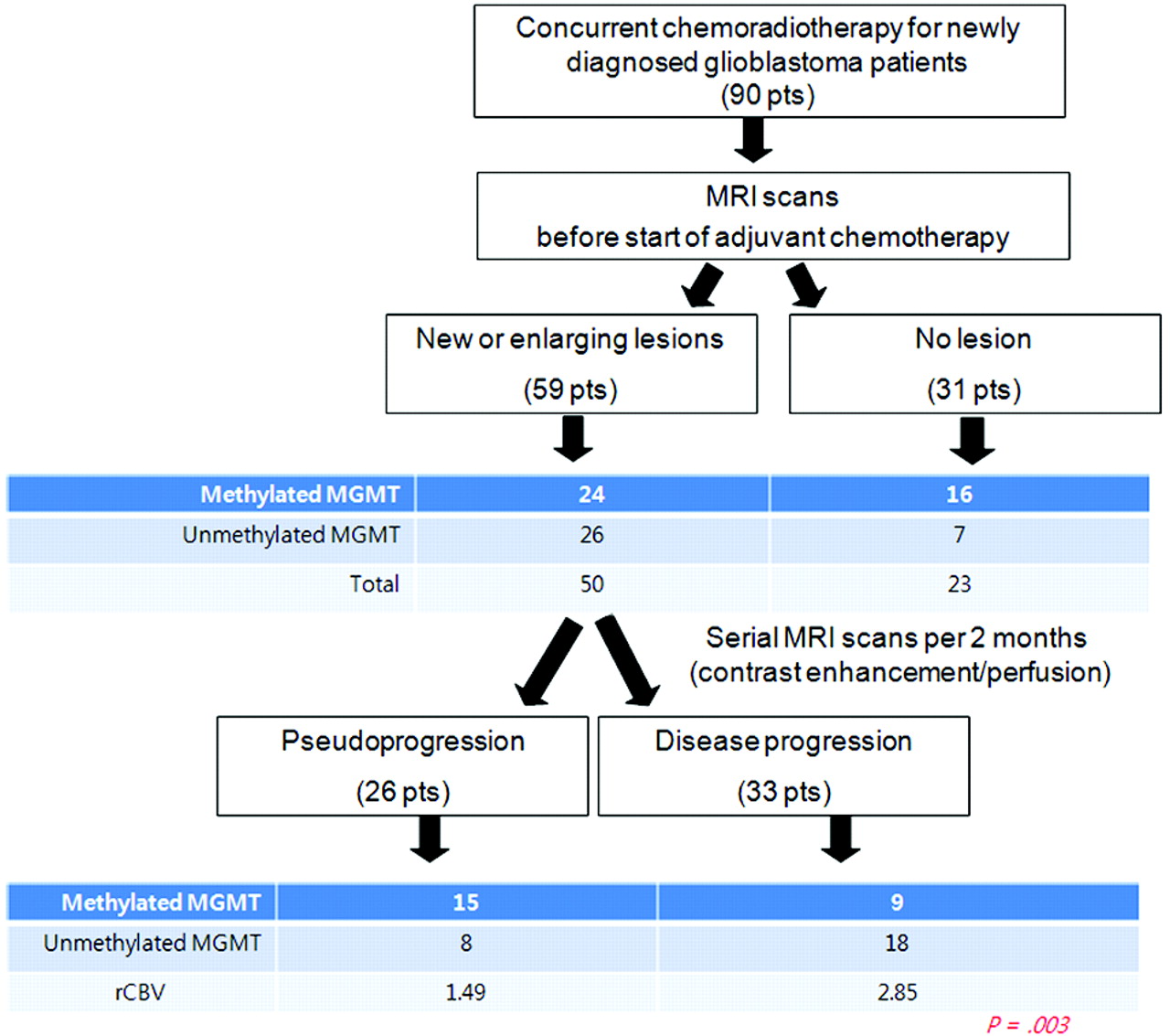
By the definition described in this protocol, new or enlarging enhanced lesions during CCRT or within 1 or 2 cycles of adjuvant treatment were analyzed by clinical examination and follow-up MR images to determine whether the lesions were pseudoprogression or real tumor progression. During this period, 59 of 90 patients (65.9%) had a new or enlarging lesion, whereas 31 patients (34.1%) had stable disease. On the basis of the serial follow-up MR imaging, new or enlarging enhancing lesions in 26 patients (28.9%) spontaneously disappeared or were stable without neurologic deterioration, which proved to be pseudoprogression, and 33 patients (36.7%) showed aggravation of the enhancing lesions with neurologic compromise, demonstrating real tumor progression. Despite radiologic change, 4 patients with neurologic compromise underwent second-look surgery, leading to a diagnosis of treatment-related necrosis. The median OS was 21.7 months (95% CI, 15.3–28.0 months) in patients with pseudoprogression, whereas it was 29.3 months (95% CI, 24.3–34.3 months) in those with stable lesions. By contrast, in those with real progression, median OS was only 13.5 months (95% CI, 9.5–17.6 months).
Association of Pseudoprogression with MGMT Status
In 17 of 90 patients, MGMT methylation status was not identified because of the poor quality of tumor tissue. In 73 patients available for the assessment of the MGMT promoter gene methylation, the promoter was methylated in 40 patients (54.8%) and unmethylated in 33 patients (45.2%). Pseudoprogression was found in 15 of 40 patients (37.5%) with a methylated MGMT promoter and in 8 of 33 patients (24.2%) with an unmethylated MGMT promoter (Fig 3). Patients with a methylated MGMT promoter had a significantly higher incidence of pseudoprogression than those with an unmethylated MGMT promoter (P = .019).

Diagram of the study design.
Predictive Value of DSC Perfusion MR Image for Pseudoprogression
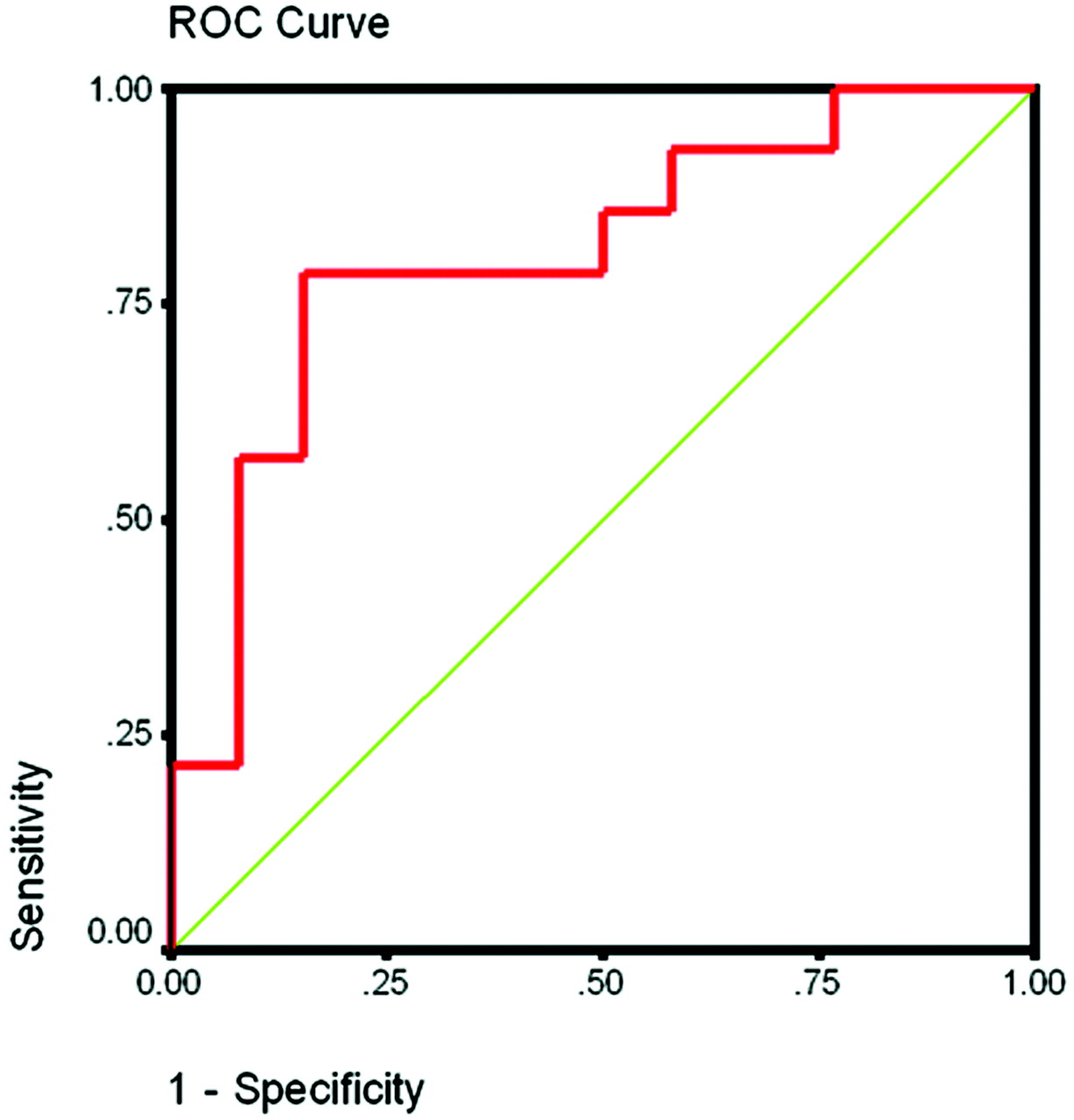
DSC perfusion MR images were prospectively assessed in 59 patients with new enhancing lesions. The mean rCBV ratios for patients with each clinical response were as follows: 1.29 (95% CI, 0.73–1.84) for stable disease (n = 31), 2.85 (95% CI, 1.99–3.70) for real tumor progression (n = 33), and 1.49 (95% CI, 1.04–1.93) for pseudoprogression (n = 26). Overall, there was a significant difference of the mean rCBV between pseudoprogression and real tumor progression (P = .003; Fig 3). On the ROC curves in perfusion images, the rCBV ratio of >1.49 had 81.5% sensitivity and 77.8% specificity (Fig 4). In 48 patients in whom rCBV and MGMT methylation studies were available, the relationship between MGMT methylation status and rCBV ratio was investigated. In the patients with GBM with an unmethylated MGMT promoter, there was a significant difference of mean rCBV between pseudoprogression and real progression (0.87 versus 3.25, P = .009), while in the methylated MGMT promoter group, no definite difference was observed between the 2 groups (1.56 versus 2.34, P = .258; Table 2).

ROC curve of rCBV predicting pseudoprogression. The rCBV ratio of >1.49 has an 81.5% sensitivity and 77.8% specificity.
Mean rCBV ratio between pseudoprogression and real progression
Discussion
Pseudoprogression is characteristically found within 2 or 3 months after treatment,2,4 whereas delayed radionecrosis generally occurs 3–12 months after radiation therapy alone.15,18 In pseudoprogression, patients can present with progressive neurologic deficits and signs of increased intracranial pressure, sometimes requiring surgery and, on occasion, even being fatal, though spontaneous radiologic and clinical recovery can also occur. The histopathologic examination of pseudoprogression demonstrates findings similar to those in radiation necrosis, such as necrosis, edema, and gliosis in addition to endothelial thickening, hyalinization, thrombosis, and occlusion of vessels.1–6 These results could be explained by chemoradiotherapy possibly causing a high degree of tumor cell and endothelial cell killing, resulting in the acceleration of the radiation necrosis.15,19 However, even in second-look surgery, differentiation between pseudoprogression and real tumor progression is very difficult because pseudoprogression can still involve residual infiltrated tumor cells, often leading to erroneous interpretation by the pathologist. Therefore, the diagnosis of pseudoprogression can be made on the basis of the combination of the clinical manifestations, radiologic findings, and pathologic findings by the multidisciplinary team approaches. Recent studies have suggested that MGMT promoter methylation status could predict the incidence and outcome of pseudoprogression in patients with newly diagnosed GBM.2,6,14
Measurement of CBV between Pseudoprogression and Real Progression
The blood volume in tumor progression increased as a consequence of a combination of neocapillary formation and dilation of existing vasculature.7,20,21 Because the contrast enhancement induced by radiation effect is also a consequence of vascular permeability, effort has been made to differentiate tumor progression and treatment-related necrosis by assessing CBV.22–27 To date, measurement of the rCBV ratio is believed to be essential for predicting real tumor progression in a variety of fields. Despite the feasibility of applying the rCBV ratio in clinical practice, reliance on this measure remains a matter of concern. First, rCBV in the cortical area is higher than that in the white matter and, subsequently, leads to confusion in interpretation. Second, rCBV provides a lower quality of resolution than in conventional MR imaging.7 Third, because many tumor progressions are intermingled with the necrotic tissue, rCBV results in the overestimation of the lesion. Nevertheless, the authors hypothesized that DSC perfusion MR imaging could provide methods for differentiating pseudoprogression from real tumor progression because vascular proliferation was characteristic of tumor progression. The results in this study provide an algorithm of how to interpret the new or progressive enhancing lesions on contrast MR images. According to our results, rCBV had more predictability in unmethylated MGMT than hypermethylated MGMT. The possible reason could be the high probability of real progression in the tumor with unmethylated MGMT status. In pseudoprogression, intermingling of necrotic tissue with real tumor portion could lead to confusion of the rCBV value.
Therapeutic Strategies for Possible Pseudoprogression of Lesions
In attempting to determine whether TMZ would be maintained or changed when encountered with new or enlarging enhancing lesions, the authors suggest first identifying the methylation status of the MGMT promoter gene. If the MGMT promoter in the tumor tissue is methylated, pseudoprogression should be considered first on the basis of the high incidence of pseudoprogression in the study of Brandes et al14 and the present data. Then, continued TMZ is recommended until the next follow-up MR imaging, even if the lesion subsequently proves to be true progression. By contrast, if the MGMT promoter is unmethylated, the rCBV measurement will be more useful in confirming or refuting real tumor progression. If the rCBV is >1.47, then the second-line treatment technique should be considered. This demonstrates that the assessment validity of rCBV should be correlatively matched with the MGMT promoter gene status.
Conclusions
rCBV value measured by DSC perfusion MR images has a differential impact on the predictability of pseudoprogression in patients with GBM. In particular, rCBV values were more powerful predictors in tumors with an unmethylated MGMT promoter status, compared with tumors with a hypermethylated MGMT status. In the near future, a more reliable distinction between pseudoprogression and real progression needs to be further clarified in well-designed prospective series of sufficient sizes.
Footnotes
Doo-Sik Kong and Sung Tae Kim contributed equally to this work.
This work was supported by the Samsung Biomedical Research Institute grant SBRI C-B0-303-1.
References
- Received April 27, 2010.
- Accepted after revision July 19, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Advanced Distance-Resolved Evaluation of the Perienhancing Tumor Areas with FLAIR Hyperintensity Indicates Different ADC Profiles by MGMT Promoter Methylation Status in Glioblastoma
- Application of 7T MRS to High-Grade Gliomas
- Diagnosis of Pseudoprogression Following Lomustine-Temozolomide Chemoradiation in Newly Diagnosed Glioblastoma Patients Using FET-PET
- MGMT Promoter Methylation Status in Initial and Recurrent Glioblastoma: Correlation Study with DWI and DSC PWI Features
- Vessel Type Determined by Vessel Architectural Imaging Improves Differentiation between Early Tumor Progression and Pseudoprogression in Glioblastoma
- Radiogenomics-based Risk Prediction of Glioblastoma Multiforme with Clinical Relevance
- Moving Toward a Consensus DSC-MRI Protocol: Validation of a Low-Flip Angle Single-Dose Option as a Reference Standard for Brain Tumors
- Multisite Concordance of DSC-MRI Analysis for Brain Tumors: Results of a National Cancer Institute Quantitative Imaging Network Collaborative Project
- Differentiating Tumor Progression from Pseudoprogression in Patients with Glioblastomas Using Diffusion Tensor Imaging and Dynamic Susceptibility Contrast MRI
- MR Imaging-Based Analysis of Glioblastoma Multiforme: Estimation of IDH1 Mutation Status
- ASFNR Recommendations for Clinical Performance of MR Dynamic Susceptibility Contrast Perfusion Imaging of the Brain
- Diffusion and Perfusion MRI to Differentiate Treatment-Related Changes Including Pseudoprogression from Recurrent Tumors in High-Grade Gliomas with Histopathologic Evidence
- Differentiation of Tumor Progression from Pseudoprogression in Patients with Posttreatment Glioblastoma Using Multiparametric Histogram Analysis
- Does MR Perfusion Imaging Impact Management Decisions for Patients with Brain Tumors? A Prospective Study