
Abstract
SUMMARY: An enlarged facial nerve canal can be a seen in both pathologic and nonpathologic processes. The purposes of this report are the following: 1) to present a rare cause of bony facial nerve canal enlargement, due to an enlarged vein, with high-resolution MDCT and histopathologic correlation; and 2) to discuss the vascular anatomy that gives rise to this variant.
Abbreviations
- A
- artery
- AICA
- anterior inferior cerebellar artery
- GSPN
- greater superficial petrosal nerve
- MDCT
- multidetector row CT
The facial nerve runs a tortuous course in the fallopian canal through the temporal bone and is well evaluated on MDCT. The caliber of the fallopian canal on MDCT is relatively fixed, particularly proximally; the diameter of the intratemporal facial canal ranges from approximately 0.9 to 2 mm on histopathology.1,2 Deviations in its size may be related to anatomic variants or pathologic processes. Herein, we describe a case of fallopian canal enlargement due to a prominent vein running alongside the facial nerve.
Case Report
The temporal bone specimen came from a 79-year-old man who had bilateral gradually progressive hearing loss and tinnitus throughout his life. There was no history of trauma or surgery to the temporal bone. He joined the National Temporal Bone Bank Program, and after his death from unrelated causes, his temporal bone was evaluated in the Temporal Bone Laboratory at our institution.
Temporal bone histopathologic specimens were stained and examined by light microscopy. We performed CT scanning of the specimen in the axial plane on a 4-channel CT scanner (Somatom Plus 4 Volume Zoom; Siemens, Erlangen, Germany) with 0.5-mm collimation, 0.5-mm thickness, 320 mAs, and 120 kV(peak). The axial data were transferred to a separate workstation for postprocessing, with a commercially available 3D reformatting software (Voxar 3D; Barco, Edinburgh, Scotland).
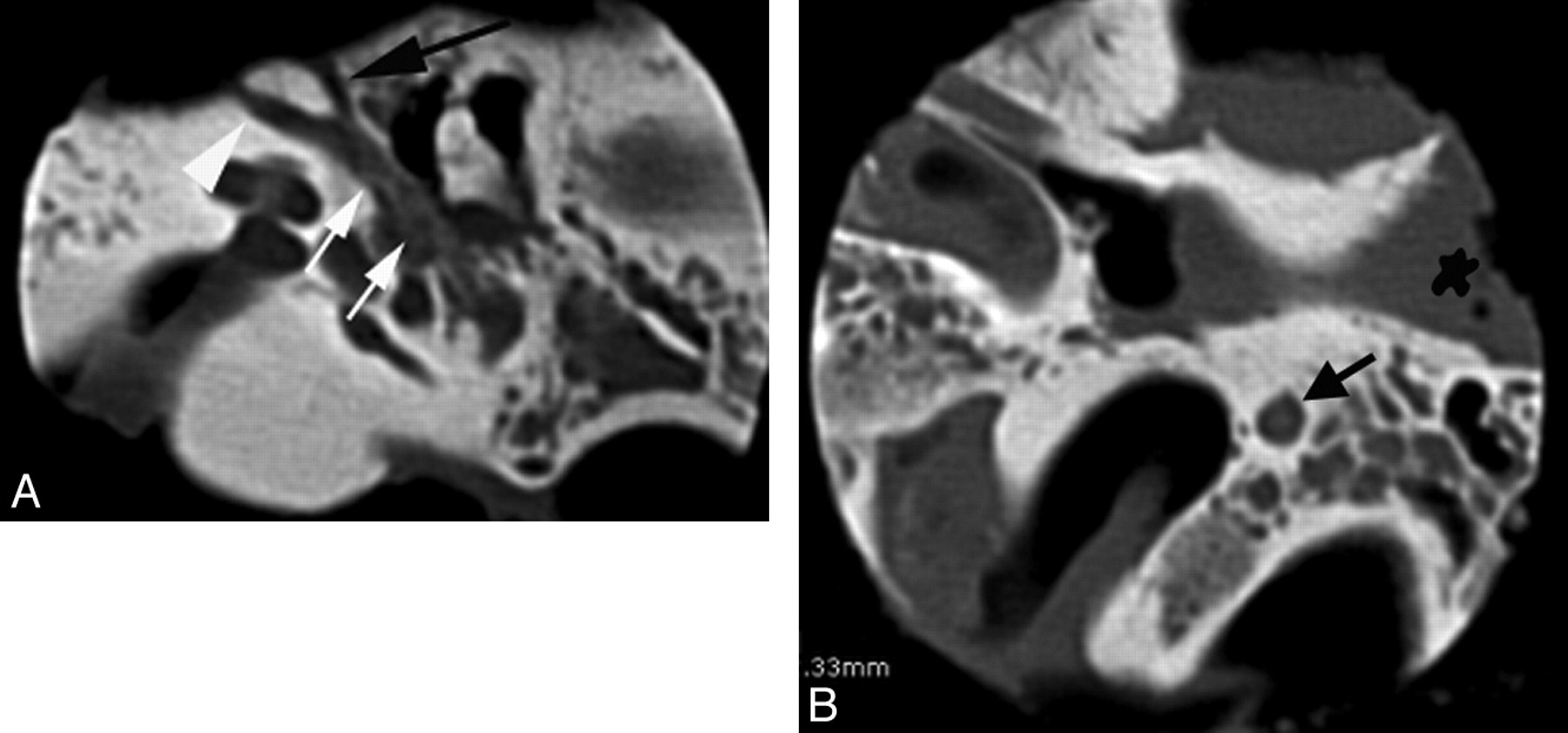
CT showed smooth enlargement of the bony facial nerve canal from the geniculate ganglion to the stylomastoid foramen without osseous erosion (Fig 1). There was a V-shaped branching pattern at the level of the first genu with 2 channels extending anteriorly. The foramen spinosum was present. The contralateral facial canal was normal in size.

A, Axial MDCT scan through the right temporal bone at the level of the cochlea demonstrates smooth enlargement of the tympanic segment of the facial canal (white arrows) with a V-shaped continuation anteriorly at the level of the first genu (black arrow and white arrowhead). B, Axial image at a more inferior level demonstrates an enlarged mastoid segment of the facial nerve (black arrow).
Histopathologically, the facial canal contained a normal-sized facial nerve with a similar-sized vein running parallel to it (Fig 2B). At the first genu, there was a V-shaped branching pattern of the venous structures replicating the CT appearance (Fig 2A).

Photomicrographs of axial histopathologic specimens through the right temporal bone. A, Prominent veins (white arrow, black arrowhead) enter the facial canal anteriorly. The asterisk indicates the genu of the facial nerve. B, An enlarged vein (small black arrow) accompanies the mastoid segment of the facial nerve (long black arrow). The asterisk indicates the cochlea; the small black arrowheads, the tympanic membrane (hematoxylin-eosin stain, 1.5× magnification).
Discussion
Arterial supply to the facial nerve is segmental. The intracanalicular facial nerve is supplied by the AICA.3 The internal auditory artery, a branch of AICA, supplies the labyrinthine segment of the facial nerve.3
The petrosal artery (also referred to as the superficial petrosal artery) branches off from the middle meningeal artery immediately after it enters the skull through the foramen spinosum.4 It enters the hiatus of the GSPN accompanying that nerve and provides arterial arborization to the geniculate ganglion and the tympanic segment (Fig 3). There is occasionally a second branch of the middle meningeal artery; the superior tympanic artery, which either anastomoses with the petrosal artery or itself extends into the facial canal (sometimes accompanying the lesser petrosal nerve) (Fig 3).4,5

Schematic illustrates the tortuous course of the intratemporal facial canal, from proximal to distal ends: 1) labyrinthine segment 2) geniculate ganglion 3) tympanic segment, and 4) mastoid segment. The petrosal artery arises from the middle meningeal artery and enters the fallopian canal via the hiatus for the GSPN (5). The superior tympanic artery arises from the middle meningeal artery and supplies the facial nerve through a separate bony canal.
The stylomastoid artery from the posterior auricular artery ascends via the stylomastoid foramen to supply the mastoid segment.5 It anastomoses with the petrosal artery in the tympanic segment of the facial nerve.4
Venous drainage of the facial nerve generally accompanies the named arteries within the nerve sheath.4 Ultimately the venous drainage from the geniculate ganglion and tympanic segment is into the middle meningeal vein.4 In our case, the V-shaped configuration of the venous channels suggests that these represent prominent petrosal and superior tympanic veins.
Causes of facial canal enlargement are numerous. Congenital/developmental variants include a persistent stapedial artery (associated with absent foramen spinosum),6 congenital cholesteatoma,7 and meningocele with or without a CSF fistula involving the facial canal.8,9 Primary facial nerve neoplasms include schwannomas, neurofibromas, hemangiomas, meningiomas, epidermoids, and paragangliomas.10–12 Also, perineural spread of parotid (and other) malignancies via this route,13 leukemic infiltration,14 and metastatic disease affecting the facial nerve15 have been described.
Although the presence of veins and arteries in the facial canal is well known,16,17 venous causes of facial canal enlargement have not been previously described. Being aware of a venous etiology of facial canal enlargement can help prevent unnecessary work-up and intervention in asymptomatic patients. The otologist can be alerted to the presence of this vascular variant if middle cranial fossa surgical procedures entailing elevation of the dura are planned to decrease intraoperative bleeding risk.
References
- Received December 28, 2009.
- Accepted after revision February 5, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.