
Abstract
BACKGROUND AND PURPOSE: CTP may help triage acute stroke patients for IAT, but requires additional contrast agent, radiation, and imaging time. Our aim was to determine whether clinical examination (NIHSS) with NCCT and CTA can substitute for CTP without significantly affecting IAT triage of patients with acute MCA stroke.
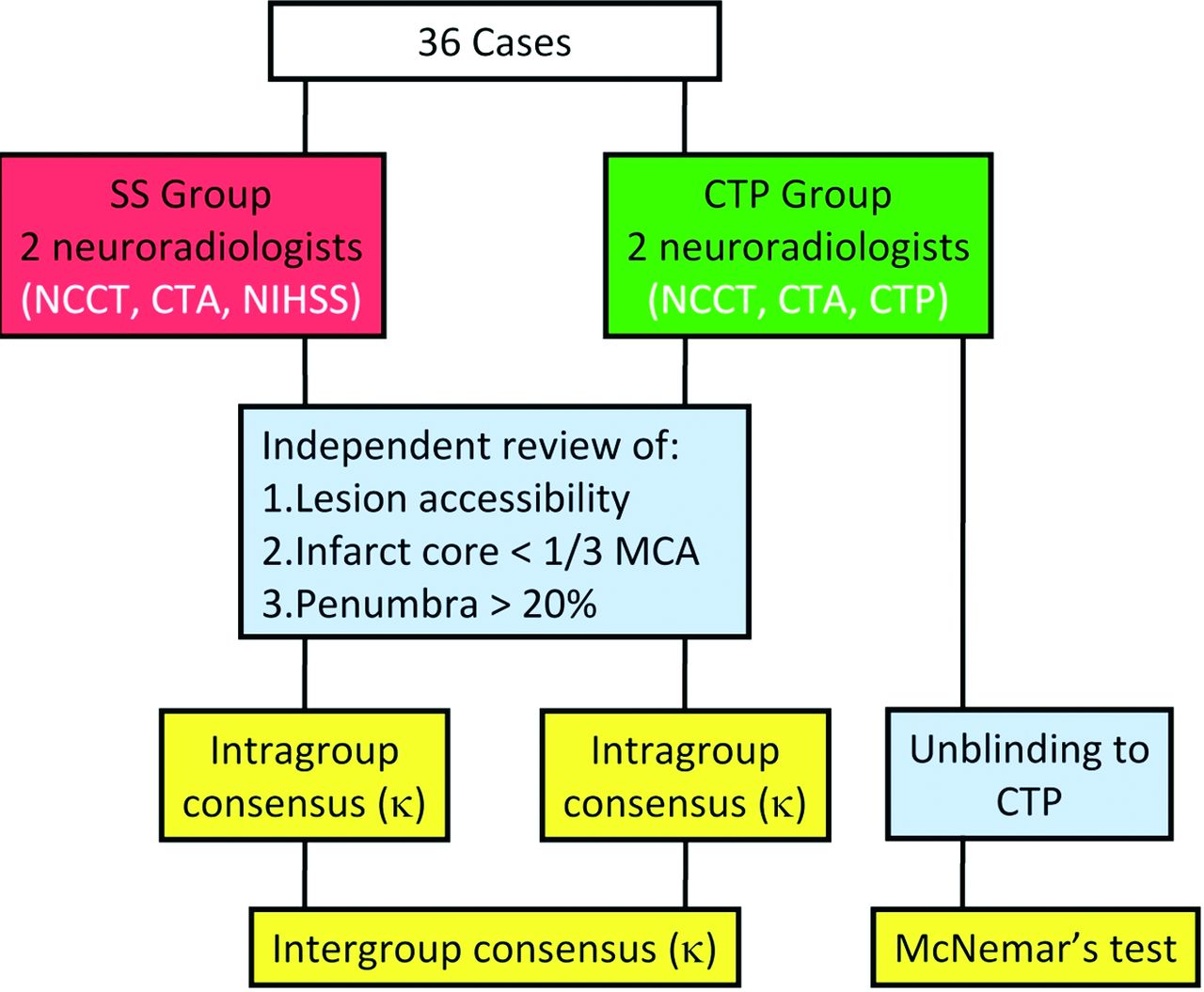
MATERIALS AND METHODS: We reviewed NCCT, CTA, and CTP imaging performed within 8 hours of symptom onset in 36 patients presenting with MCA territory stroke (September 2007–October 2009). Two neuroradiologists reviewed, independently and by consensus, NCCT, CTA, and CTP (CTP group), and 2 different neuroradiologists blinded to CTP reviewed NCCT, CTA, and NIHSS (stroke scale group) to determine IAT eligibility: M1 or proximal M2 occlusion; infarct core <1/3 MCA territory; and ischemic penumbra >20% infarct core. The stroke scale group estimated infarct core from NCCT and CTA source images and ischemic penumbra from core size relative to NIHSS score and re-evaluated patients after unblinding to CTP. We computed intragroup and intergroup κ scores for IAT treatment recommendation and used the McNemar test to determine whether CTP significantly affected the stroke scale group's decisions.
RESULTS: IAT was recommended in 16/36 (44%) and 17/36 (47%) patients by the CTP and stroke scale groups, respectively, with intragroup κ scores of 0.78 ± 0.11 versus 0.83 ± 0.09. The intergroup κ score was 0.83 ± 0.09. When unblinded to CTP, the stroke scale group revised 2/36 (5.6%) decisions, which was insignificant (P = .48, McNemar test).
CONCLUSIONS: NIHSS interpreted with NCCT and CTA may be an effective substitute for CTP-derived measures in the IAT triage of patients with acute MCA stroke. Replacing CTP may potentially reduce radiation and contrast dose and time to treatment.
ABBREVIATIONS:
- ASPECTS
- Alberta Stroke Program Early CT Score
- IA
- intra-arterial
- IAT
- intra-arterial thrombolysis
- PROACT
- Prolyse in Acute Cerebral Thromboembolism
- SE
- standard error
Patients with acute ischemic stroke can be treated with IV-tPA up to 4.5 hours after symptom onset.1,2 For patients presenting later, for whom IV-tPA is contraindicated or for whom there is no clinical improvement following IV-tPA, IAT (intra-arterial thrombolytic infusion or mechanical thrombectomy) can be performed.3⇓–5 Traditionally, the only imaging performed before IV-tPA is NCCT to exclude acute hemorrhage or a large completed infarction. With the recent widespread availability of CTP, there has been enthusiasm for using CTP to assist in IAT triage. The fundamental premise is that patients have a central “core” of permanently infarcted tissue, surrounded by a “penumbra” of oligemic tissue at risk of infarction.6⇓–8 Timely reperfusion of penumbra could potentially limit infarction size. Conversely, reperfusion of a large infarct core could result in hemorrhage. In selecting patients for IAT, many centers seek a “mismatch,” where penumbra significantly exceeds infarct core.
At our institution, the acute stroke imaging protocol for patients with potential IAT has included NCCT, CTA, and CTP, with the primary criteria for considering IAT including the following: 1) absence of intracranial hemorrhage, 2) presence of a microcatheter-accessible proximal MCA occlusion, 3) absence of completed infarction exceeding one-third of the MCA territory, 4) identifiable penumbra exceeding core infarct by >20% (total core plus penumbra exceeding 120% of infarct core alone), and 5) treatment within approximately 8 hours of symptom onset. The purpose of our study was to determine whether a clinical measure of stroke penumbra based on the NIHSS, used conjunctively with NCCT and CTA, could effectively substitute for CTP performed by using common methodology. We hypothesized that NIHSS interpreted with NCCT and CTA may be a surrogate for CTP-derived measures in the IAT triage of patients presenting with acute MCA occlusion.
Materials and Methods
The Institutional Review Board granted a waiver of authorization for this retrospective Health Insurance Portability and Accountability Act–compliant study. We reviewed initial NCCT, CTA, and CTP examinations for all consecutive patients with acute MCA territory stroke presenting within 8 hours of symptom onset at our 2 teaching hospitals between September 2007 and October 2009. Patients with acute hemorrhage, ICA occlusion, or posterior circulation stroke were excluded. We obtained clinical history (time from symptom onset to imaging, age, sex, and NIHSS scores) from the electronic medical record. CT examinations were performed on a LightSpeed Qx/I 16 or VCT 64 (GE Healthcare, Milwaukee, Wisconsin) or Somatom 16 (Siemens, Erlangen, Germany) scanner with 16, 64, and 16 detector rows, respectively, and with corresponding craniocaudad brain coverage for CTP of 4.0, 8.0, or 2.4 cm. CTP used standard vendor acquisition and postprocessing algorithms (CT Perfusion 3, Version 2.6.10; CT Perfusion 4, Version 4.3.7; GE Healthcare and syngo CT 2006G, Version 1; Siemens, respectively).
Four Certificate of Added Qualification–certified neuroradiologists (with 6, 10, 20, and 20 years of postfellowship experience) independently reviewed all cases. One diagnostic neuroradiologist and 1 interventional neuroradiologist (CTP group) reviewed NCCT, CTA, and CTP data, blinded to NIHSS. The other 2 neuroradiologists, 1 diagnostic and 1 interventional (stroke scale group), reviewed NCCT, CTA and NIHSS data, blinded to CTP images (Fig 1.). Patients were deemed eligible for IAT if they met the following criteria:
1) CTA showed an M1 or proximal M2 occlusion (within 1 cm of the MCA bifurcation), which we defined to be “accessible” lesions;
2) Infarct core, estimated with NCCT and CTA source images9,10 (stroke scale group) or CBV (CTP group), was less than one-third of the MCA territory; and
3) Ischemic penumbra exceeded 20% of infarct core. The CTP group estimated penumbra by perceived mismatch between CBV and MTT or TTP. The stroke scale group estimated penumbra by comparing the NIHSS score with the site of arterial occlusion on CTA.11,12 In general, NIHSS scores between 8 and 12 have been considered most consistent with functional M2 branch occlusions or nondominant hemisphere distal M1 occlusion. An NIHSS score >12 has been considered most consistent with functional proximal M1 occlusion. We extrapolated these relationships in our study to conclude that for NIHSS score ≥8 and completed infarct core less than one-third of the MCA territory, there existed a significant physiologic ischemic penumbra.

Summary of the study design, highlighting independent and consensus analysis by neuroradiologists by using CTP (CTP group) and NIHSS with CTA (stroke scale group) to estimate infarct core and penumbra. Intragroup and intergroup consensus were determined (κ), as well as the significance of unblinding the stroke scale group to CTP (McNemar test).
For each case, reviewers in each group graded lesion accessibility and completed infarct less than one-third of the MCA as “yes” or “no” and significant penumbra as “yes,” “no,” or “unsure,” making a best guess if unsure and if the decision would ultimately influence IAT triage (ie, cases with an accessible lesion and infarct core less than one-third of the MCA). IAT was recommended if all criteria were satisfied. After initial independent review, stroke scale and CTP group reviewers re-examined cases with discrepancies in any of the 3 criteria and came to intragroup consensus for all 3 criteria and the overall IAT decision. After a 2-week delay, the stroke scale group re-evaluated all cases unblinded to CTP, both independently and by consensus, and rescored the overall IAT triage. κ values and SEs were calculated both within each group and between the consensus decisions of both groups for each of the 3 independent criteria as well as for the overall IAT triage decision. We used the McNemar test to determine whether adding CTP data significantly affected decisions made by the stroke scale group.
For clarification, the actual decision to offer or not offer IAT for each patient at presentation incorporated all available information (NCCT, CTA, CTP, and NIHSS) but was also individualized to each patient. We compared the actual treatment decision for each patient with the retrospectively determined decisions from both groups. The IA therapies used in this study included IA-tPA infusion and mechanical thrombectomy (Merci retriever; Concentric Medical, Mountain View, California).
Results
Thirty-six patients, including 18 men and 18 women, met the inclusion criteria: mean patient age of 71.7 (range, 34–92 years), mean presenting NIHSS score of 17.4 (range, 8–27), and mean time from symptom onset (or when last known to be asymptomatic) to imaging of 4 hours 19 minutes (range, 1 hour 21 minutes to 8 hours 22 minutes). Ten, 10, and 16 patients were scanned on Qx/I 16, VCT 64, and Somatom 16 scanners, respectively. The intra- and intergroup agreements for each of the 3 IAT criteria are reviewed below and summarized in the Table
Summary of intragroup and intergroup scores for the 3 IAT criteriaa
There was complete intragroup and intergroup agreement regarding lesion accessibility. This was a completely objective measure based on CTA, and 28/36 (78%) of cases had accessible lesions.
Regarding infarct core less than one-third of the MCA, the interobserver κ score was 0.94 (SE, 0.06) and 0.66 (SE, 0.14) for the stroke scale and CTP groups, respectively, with 6 intragroup discrepancies among the 2 groups. Of the 5 discrepant cases within the CTP group, 3 were performed on the VCT 64 scanner, 1 on the Qx/I 16 scanner, and 1 on the Somatom 16 scanner. The intergroup consensus κ score for infarct core was 0.93 (SE, 0.07), with 1 discrepant case.
Regarding penumbra >20% of infarct core, the CTP group rendered opinions for every case with an interobserver κ score of 0.83 (SE, 0.09) and 3 discrepant cases (2 performed on the Somatom 16 scanner, 1 on the VCT 64 scanner). At least 1 stroke scale group reader was “unsure” of penumbra status in 14/36 cases that did not require penumbra estimation for IAT triage: Eight had inaccessible lesions, and 6 had completed infarct more than one-third of the MCA. Of the 22 cases in which both stroke scale readers rendered an opinion, there were 3 discrepancies, with an interobserver κ score of 0.64 (SE, 0.19). The intergroup consensus κ score for the 22 mutually graded cases was 0.49 (SE, 0.22).
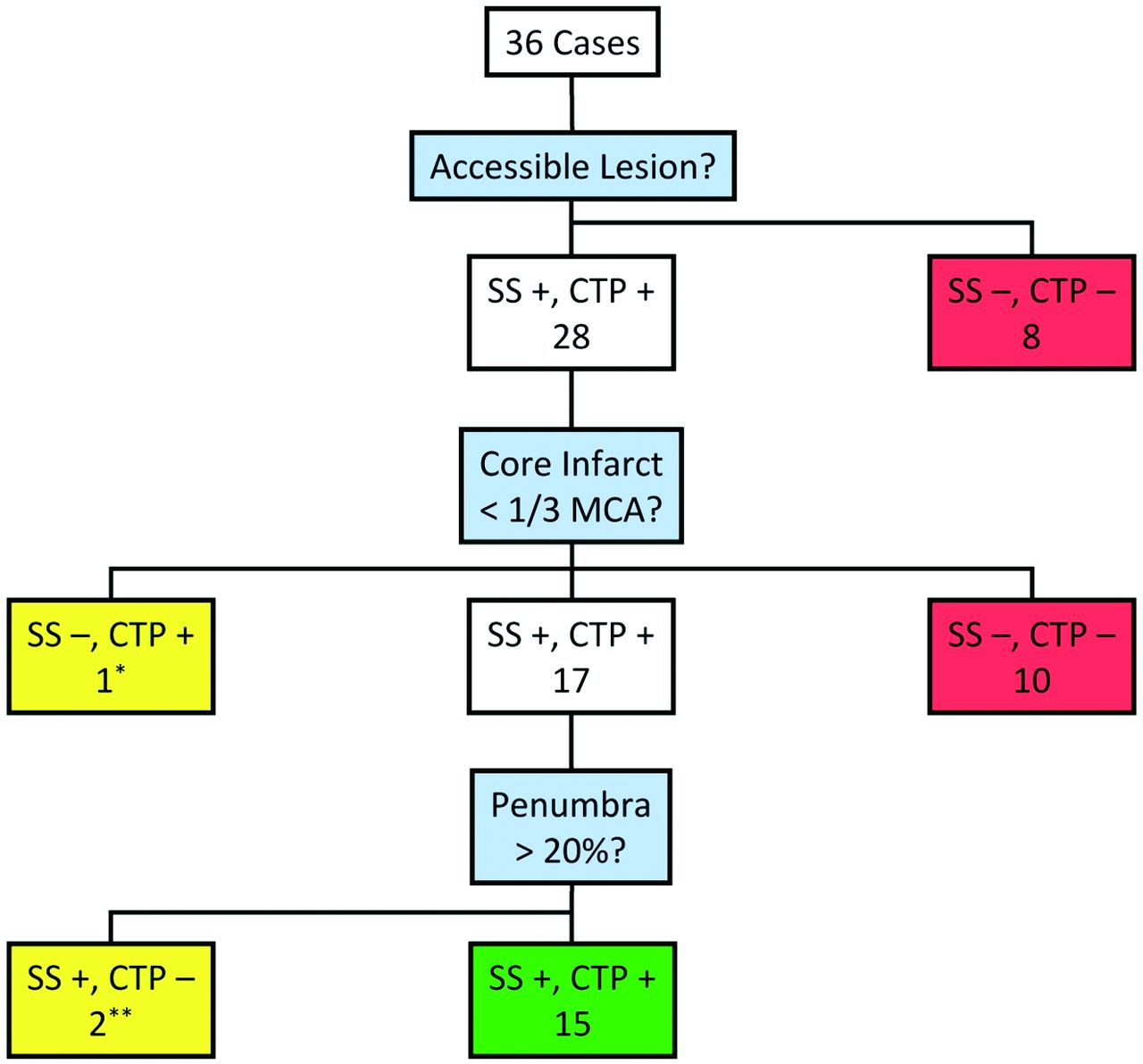
Of the 36 cases, 28 had an accessible lesion, of which 10 were concluded by both groups to have infarct core more than one-third of the MCA, and 17 were concluded to have a treatable infarct core. In 1 discrepant case, the CTP group deemed the infarct core treatable, whereas the stroke scale group did not (Fig 2). Of the 17 cases concluded by both groups to be treatable on the basis of access and infarct core, 15 were mutually agreed to have a treatable penumbra (eg, Fig 3). In the other 2 cases, the penumbra of the stroke scale group was deemed treatable, whereas that of the CTP group was not (Figs 4 and 5). Therefore, the overall CTP and stroke scale group consensus was to offer IAT in 16/36 (44%) and 17/36 (47%) patients, respectively, with IAT recommended for 15 of the same patients between the 2 groups, with only 3 discrepancies: 2 cases designated as “treat” by the stroke scale group and “no treat” by the CTP group on the basis of penumbra estimation, and 1 case designated “no treat” by the stroke scale group and “treat” by the CTP group on the basis of infarct core estimation. The intragroup κ scores for overall treatment were similar: 0.78 (SE, 0.11) and 0.83 (SE, 0.09) for the CTP and stroke scale groups, respectively. The κ score for intergroup consensus was 0.83 (SE, 0.09), with statistically significant correlation between treatment decisions for the 2 groups (P < .0001, 2-tailed Fisher exact test). The overall treatment decisions are summarized in Fig 6 .

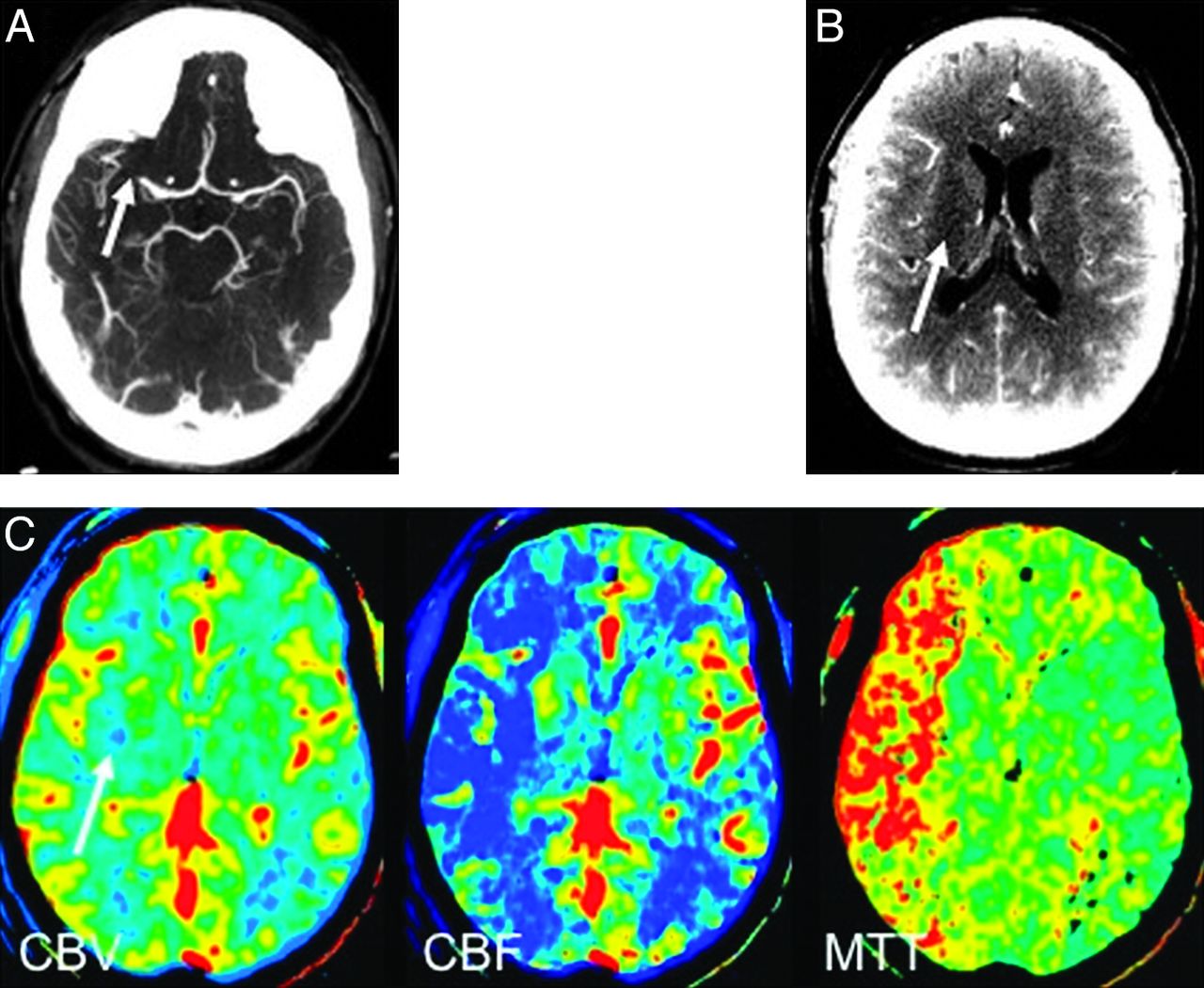
A 76-year-old woman 5 hours 22 minutes after symptom onset (NIHSS score = 25). A, CTA demonstrates left M1 cutoff (white arrow). B, CTA source images demonstrate hypoattenuation in the left corona radiata, basal ganglia, and temporal lobe consistent with MCA infarct. C, Predominantly matched CBV and CBF defects corresponding to a portion of infarct core predicted on CTA source images, with peripheral prolonged TTP suggesting penumbra (Somatom 16). IAT recommendations for stroke scale (infarct core more than one-third of the MCA territory) and CTP (treatable penumbra) groups were discordant.

A 47-year-old man 3 hours 37 minutes after symptom onset (NIHSS score = 17). A, CTA demonstrates right M1 cutoff (white arrow). B, CTA source image demonstrates equivocal hypoattenuation in the right corona radiata (white arrow), suggesting a small infarct. C, Large mismatched CBF and MTT compared with CBV (white arrow), consistent with treatable penumbra (LightSpeed Qx/I). On the basis of NIHSS score, locus of M1 cutoff and size of infarct core, the stroke scale group also recommended IAT.

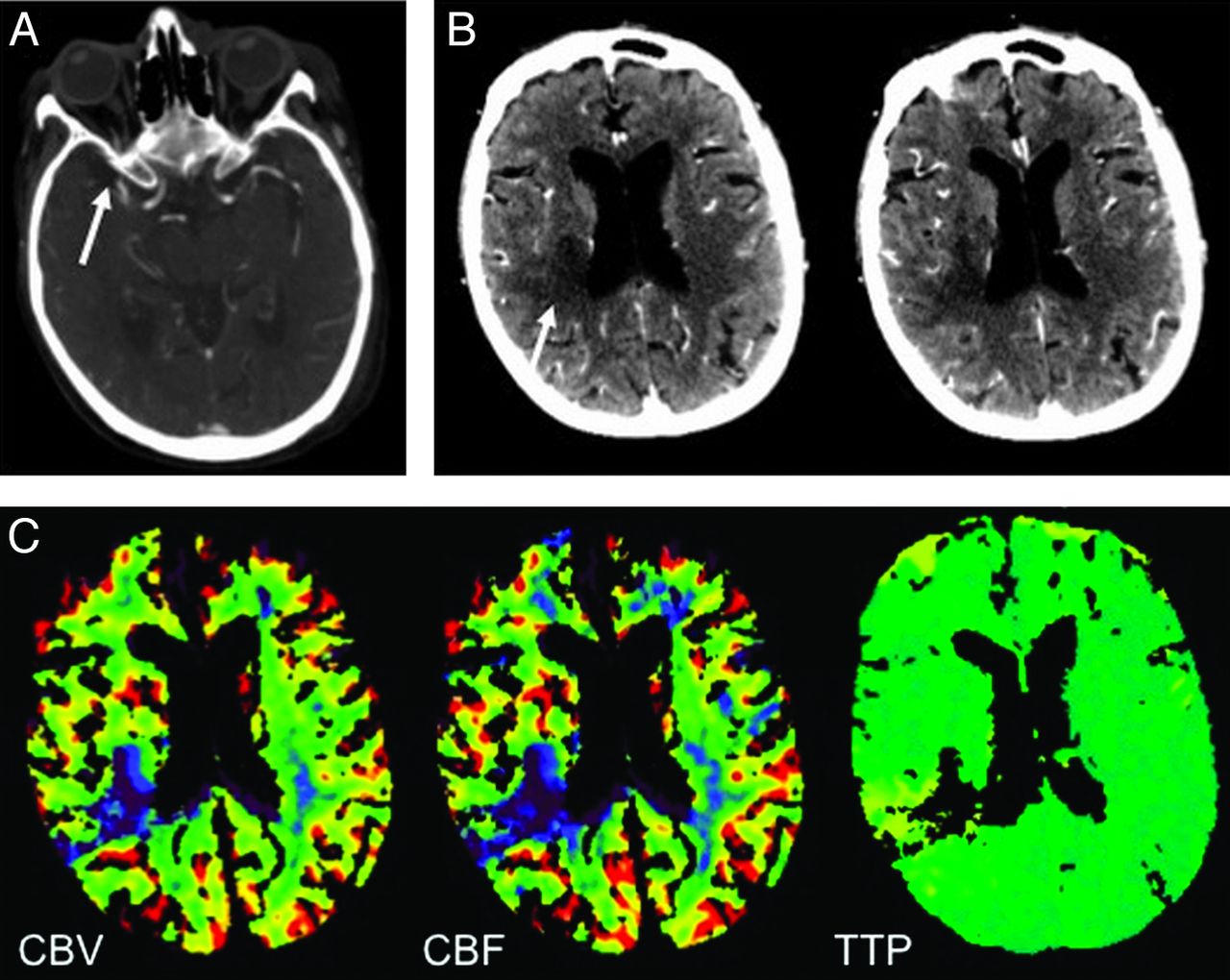
An 88-year-old woman 3 hours 1 minute after symptom onset (NIHSS score = 17). A, CTA demonstrates right M1 cutoff (white arrow). B, CTA source images demonstrate hypoattenuation in the posterior right MCA territory (white arrow), consistent with a small infarct. C, Matched CBV and CBF defects corresponding to the infarct core on CTA source images, with matched TTP defect predicting the absence of treatable penumbra (Somatom 16). On the basis of the NIHSS score, locus of M1 cutoff, and size of infarct core, the stroke scale group predicted a treatable penumbra and recommended IAT. The stroke scale group revised its recommendation to “no treat” when unblinded to CTP.

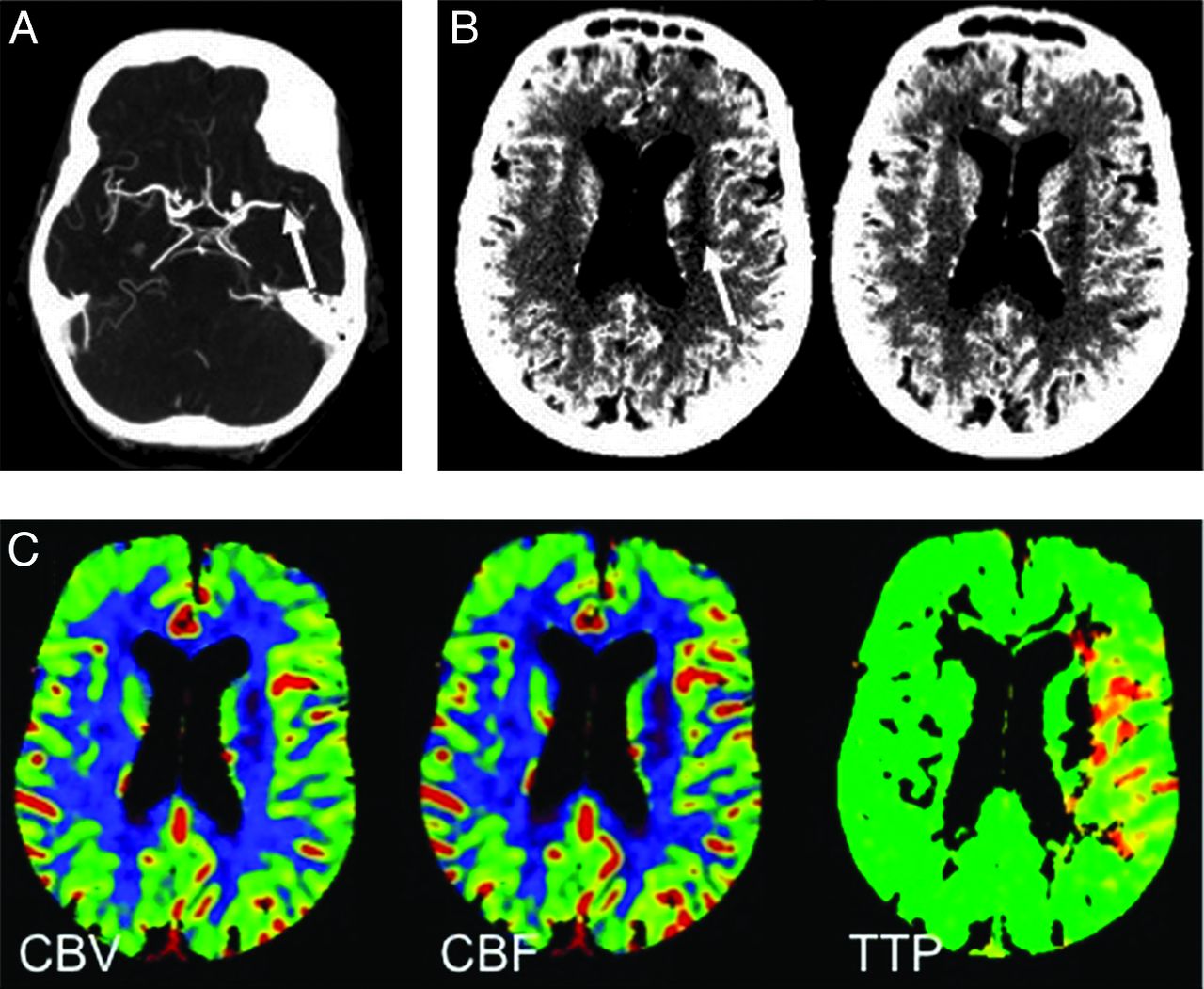
A 92-year-old woman 4 hours 11 minutes after symptom onset (NIHSS score = 9). A, CTA demonstrates a focal defect in the distal left M1 (white arrow). B, CTA source images demonstrate hypoattenuation in the left corona radiata (white arrow), consistent with a small infarct. C, Essentially matched CBV and CBF defects corresponding to the infarct core on CTA source images, with a matched TTP defect including a small peripheral region of prolonged TTP predicting the absence of substantial penumbra (Somatom 16). On the basis of the NIHSS score, the locus of M1 cutoff, and size of infarct core, the stroke scale group predicted a treatable penumbra and recommended IAT. The stroke scale group revised its recommendation to “no treat” when unblinded to CTP.

Summary of treatment decisions for the stroke scale and CTP groups. Of the 28 patients with accessible lesions, 17 were concluded by both groups to have treatable infarct core (less than one-third of the MCA territory), 15 of whom had treatable penumbra (>20% infarct core). There was 1 discrepancy regarding infarct core (asterisk), treated by the CTP but not the stroke scale group, and 2 discrepancies regarding penumbra (double asterisks), both treated by the stroke scale but not the CTP group but reversed by the stroke scale group on unblinding.
After unblinding to CTP, the stroke scale group revised 2/36 (5.6%) overall IAT decisions by consensus from “treat” to “no treat,” increasing the intergroup κ score to 0.94 (SE, 0.06). Both revisions were based on penumbra estimation, and the changes in overall IAT triage were deemed insignificant by using the McNemar test (P = .48).
Of the 25 patients with accessible lesions and intergroup retrospective treatment consensus, there was discordance with actual IAT triage in 5 cases (20%). In 3 cases, retrospective recommendation was to treat and the patient did not actually receive IAT, most commonly due to old age and perceived inability to tolerate the procedure. In 2 cases, retrospective recommendation was to not treat and the patient did actually receive IAT, primarily due to young age and anticipated poor quality of life without intervention; in 1 such case, there was subsequent parenchymal hematoma type 2. Of the 20 patients with concordant IAT triage, 12 received IAT, 2 with subsequent hemorrhagic infarct type 1 and 1 with hemorrhagic infarct type 2.
Discussion
The goal of revascularization therapy in acute MCA occlusion is timely flow restoration to salvageable brain. Historically, time from symptom onset has been a surrogate marker of tissue viability. Pre-IAT imaging is aimed at identifying patients with substantial tissue at risk and smaller areas of irreversible core infarct. Major IV-tPA2,13 and IAT3,4 trials have used only NCCT before intervention. To justify routine use of CTP (with associated increased iodinated contrast and radiation dose as well as increased imaging time and cost) for IAT triage, differences in decision making or improvements in outcome must be demonstrated. Two central premises underlie our study. The first is that NIHSS, combined with the site of arterial occlusion on CTA, provides adequate estimation of infarct core plus penumbra, while providing an anatomic guide for lesion accessibility. The second is that patients in whom revascularization is unlikely to help and could potentially be detrimental (ie, from hemorrhage) can be identified by using NCCT.
Among the standard CTP parameters, MTT is elevated in both penumbra and infarct core, whereas CBV is typically diminished only in the infarct core.6 Thus, MTT-CBV mismatch is commonly thought to reflect the ischemic penumbra. Because penumbra represents nonfunctioning ischemic brain, an alternative estimate for infarct core plus penumbra would involve a combination of clinical examination (NIHSS) and a proximal arterial occlusion on CTA. There is significant correlation between admission NIHSS score and the site of arterial occlusion,11,12,14 with patients with NIHSS scores ≥12 likely having a proximal MCA occlusion and corresponding ischemia. There is also a strong correlation between NIHSS score and MR PWI lesion volume.15,16 We, therefore, believe that a large clinical deficit (NIHSS score ≥8) in conjunction with a proximal arterial occlusion on CTA allows estimation of total infarct core plus penumbra, obtainable without CTP. The use of clinical examination alone has been previously evaluated as the “clinical diffusion mismatch,” which initially showed promise but has more recently not been shown to correlate as well as PWI.15⇓–17 Most interesting, when MRA-DWI mismatch has been evaluated, it does appear to be predictive of patients improving with recanalization.18 We, therefore, believe that the combination of NIHSS and vascular status provides a robust justifiable estimation for the presence of large territories of tissue at risk.
Other reasons to use CTP might be to potentially reduce the risk of intracerebral hemorrhage, especially parenchymal hematoma type 2,19 and to prognosticate clinical outcome; however, studies suggest that NCCT may be sufficient. Trials of IV-tPA20 and IAT21 demonstrated increased risk of hemorrhage when more than one-third of the MCA territory had hypoattenuation on NCCT. Similar thresholds by using ASPECTS have been demonstrated for both IV-tPA and IAT, with ASPECTS ≤7 having worse outcomes22 and patients with ASPECTS >7 receiving IAT in the PROACT trial 3 times more likely to have independent functional outcome.23 Good correlation between CBV and NCCT has been demonstrated, with NCCT ASPECTS ≤7 and CBV ASPECTS ≤8 predicting poor outcome.24 Patients with ASPECTS >7 are also most likely to benefit from combined IV-tPA and IAT,25 and ASPECTS <7 has been shown to provide a conclusive estimate of more than one-third of the MCA territory infarction.26 Further estimation of infarct core was available in our study by using CTA source images, which have been shown to approximate CBV and final infarct volume under certain conditions.9,10
Our results show very high correlation (κ = 0.83) for IAT recommendation by using our IAT inclusion criteria between a reader group using CTP and another relying on NCCT, CTA source images, and NIHSS for infarct core and penumbra determination. Unblinding the latter group to CTP did not significantly alter intergroup κ; this finding suggests that CTP may not contribute to the IAT triage algorithm in a substantive manner. One caveat is that while CTA source images have approximated CBV and final infarct volume in the past,9,10 the advent of faster 64-, 256-, and 320-detector scanners has rendered these images more CBF-weighted and less CBV-weighted,27,28 which could potentially limit their use as a surrogate for infarct core on CBV maps. We think, however, that use of NCCT ASPECTS (with a threshold value of 7) may alleviate this potential problem in identifying patients not likely to benefit from IAT.26
Scanners providing varying degrees of MCA territory coverage on CTP were used in this study, raising the question of whether scanner differences affected intra- and intergroup agreement and IAT recommendations. Somatom 16 examinations were performed with two 12-mm slabs covering 2.4 cm, without coverage of the entire MCA territory, theoretically rendering it more difficult to estimate the one-third MCA rule, compared with the LightSpeed scans using eight 5-mm sections covering 4.0 cm (Qx/I 16) and sixteen 5-mm sections covering 8.0 cm (VCT 64). Of the 8 intragroup discrepancies in the CTP group (5 for infarct core, 3 for penumbra), 5 were obtained on a GE Healthcare scanner with the greater degree of volume coverage, implying that limited volume coverage does not impact the variability of core or penumbra estimation.29,30 Potential secondary benefits of our hybrid CT resources were that by blending patient studies, we reduced bias resulting from manufacturer-specific CTP calculation algorithms and simulated the cross-section of CTP methodologies in the community.
It is worth considering whether the high intergroup κ is due to a predominance of inaccessible lesions or large infarct cores, which would render CTP-based penumbra estimation moot. In our patient series, there were 8 inaccessible lesions; for the 28 patients with accessible lesions, the intergroup κ for IAT triage is still 0.78 (SE, 0.12) and the McNemar test is unchanged. There were 10 cases with accessible lesions and intergroup consensus of infarct core of more than one-third of the MCA territory; infarct core was disputed in 1 case, leaving 17 cases in which both groups agreed that penumbra estimation would affect IAT triage. There were 2 discrepant penumbra estimations in these 17 cases. Assuming that CTP yields the “correct” estimation of penumbra, one would predict a 2/17 (12%) chance of selecting the “wrong” treatment plan on the basis of CTA and NIHSS in patients with accessible lesions and small infarct cores. In actuality, these 2 patients did not receive IAT. In 1 case rated “treat” by the stroke scale group and “no treat” by the CTP group (Fig 5), the follow-up infarct on CT 17 days after CTP matched the CBV core with no appreciable infarct extension. In the other case rated “treat” by the stroke scale group and “no treat” by the CTP group (Fig 4), the follow-up infarct on CT approximately 1 year after CTP demonstrated extension to the midanterior right temporal lobe, and it is unclear whether this represented infarct progression or a new interval infarct. In the case in which infarct core size was disputed (Fig 2), the patient did not receive IAT in actuality, and no follow-up imaging was available. How the risk of selecting the “wrong” treatment plan by omitting CTP compares with the benefit of cost-savings (radiation dose, administered contrast material) is a matter of debate. A compromise protocol might be to only perform CTP in those cases with an accessible lesion and small infarct core, which occurred in 17/36 (47%) of our cases.
There is no consensus within the stroke imaging community on the ideal IAT selection criteria, and this remains an area of active investigation; we chose common published criteria used for clinical trials summarized in Mishra et al.31 The optimal CTP postprocessing algorithms for defining infarct core and ischemic penumbra have yet to be determined.32 In fact, the paradigm of CBV-CBF mismatch as the optimal measure of penumbra has been challenged, and collateral vessels rather than core/penumbra mismatch may be a superior overall predictor of clinical outcome.33 Our study could be extended to compare NIHSS with other CTP parameters and thresholds. CTP acquisition, reconstruction, and postprocessing are highly variable and vendor-dependent.34,35 We used different scanners from different vendors in this study, which introduces variability; it is possible that a particular stroke may satisfy penumbra criteria on 1 scanner but not another. We used subjective rather than quantitative analysis of core size and penumbra extent. Although this potentially introduces error for any given IAT criteria threshold, it may better match the general “real-time” approach used in the community without time-consuming postprocessing.
Our study was not designed to address the controversial question of whether CTP-generated CBV accurately reflects infarct core analogous to DWI or whether CTP mismatch correctly depicts penumbra. For instance, there is evidence that DWI infarct core may have high, low, or normal CBV depending on infarct age.36 We acknowledge that CTP is not necessarily a criterion standard facilitating “correct” IAT triage with which the stroke scale group's decision should be compared. Our objective was to determine whether triage decisions with and without the use of CTP are analogous, with our hypothesis being that CTP does not significantly alter the triage decision that would have been made by using NIHSS without CTP. We conclude that this is true in most cases, regardless of whether it is the “right” decision or not.
The main limitations of our study are its retrospective nature, small sample size, and possible lack of applicability to other acute stroke-management programs. Neuroradiologists reviewed all of our studies, whereas general radiologists or neurologists might review most acute stroke imaging nationwide. An additional limitation is the lack of a criterion standard for outcomes because it is not possible to compare infarct progression, hemorrhage, and clinical status for both “treat” and “no treat” states in each patient. Furthermore, DWI is generally thought to be the best imaging measure of infarct core and may therefore provide additional benefit in triaging IAT candidates; the applicability of our results to MR PWI is unknown, but DWI, MRA, and NIHSS, without PWI, may be analogously sufficient for IAT decision making using MR imaging.18 Although this presents less of a contrast agent and radiation issue, it would still offer a reduction in imaging time. We think that our focus on CT is important because CT is prevalent in community emergency departments, and there is increasing concern about radiation exposure. Nonetheless, an MR imaging analog of our study could be performed by comparing DWI/MRA with MR PWI and DWI/MRA with NIHSS.
Conclusions
For patients presenting with acute MCA stroke within approximately 8 hours of symptom onset, the IAT triage decision was not significantly different with or without CTP, when clinical examination (NIHSS), site of occlusion on CTA, and infarct core estimation on NCCT or CTA source images were provided for analysis. Further research into whether CTP improves outcomes appears to be justified before it is routinely applied to patients who are potential candidates for IAT. Replacing CTP may potentially reduce radiation and contrast dose, time to treatment, and cost.
Footnotes
-
Paper previously presented in part at: 96th Scientific Assembly and Annual Meeting of the Radiological Society of North America, November 28–December 3, 2010; Chicago, Illinois.
Disclosures: Mahesh Jayaraman—UNRELATED: Consultancy: Depuy Institute, Comments: One-time consulting fee.
References
- Received December 1, 2011.
- Accepted after revision February 3, 2012.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effect of Radiographic Contrast Media Shortage on Stroke Evaluation in the United States
- Endovascular treatment for acute ischaemic stroke due to medium vessel occlusion: data from ANGEL-ACT registry
- NCCT and CTA-based imaging protocol for endovascular treatment selection in late presenting or wake-up strokes
- Initial hospital management of patients with emergent large vessel occlusion (ELVO): report of the standards and guidelines committee of the Society of NeuroInterventional Surgery
- Future acute ischemic stroke trials should randomize on the angio table