
Abstract
BACKGROUND AND PURPOSE: Given the challenges posed by surgical clipping, endovascular techniques have been increasingly used to treat SHA aneurysms. The purpose of this study was to assess the safety and efficacy of endovascular techniques in the treatment of SHA aneurysms.
MATERIALS AND METHODS: Medical charts and initial and follow-up angiograms were reviewed retrospectively for all patients treated with endovascular procedures at our institution between January 2006 and February 2011.
RESULTS: We identified 87 patients with SHA aneurysms who were treated with endovascular techniques. Of these patients, 79 were women and only 8 were men (90.8% female predominance). Thirty-five patients were treated with coil embolization; 45, with stent-assisted coiling; 4, with balloon-assisted coil embolization; and 3, with a flow-diversion technique. Minor complications occurred in 2 patients (2.2%). None of the patients had a major complication. The mortality and permanent morbidity rates related to the procedure were 0%. Imaging follow-up was available for 89.4% of patients (DSA in 65, MRA in 11 patients) at a mean time point of 10.4 months (range, 6–60 months). Of the 76 patients with available follow-up, 3 patients had a recurrence (3.9%) and only 1 required further intervention (1.3%). Stent-assisted coiling was associated with lower recurrence rates than simple coil embolization.
CONCLUSIONS: SHA aneurysms have the lowest recurrence rate with endovascular treatment compared with aneurysms in other locations by using historical data. Because of its safety and efficacy, endovascular therapy should be considered the procedure of choice for the treatment of SHA aneurysms.
ABBREVIATION:
- SHA
- superior hypophyseal artery
SHA aneurysms are rare. They arise from the internal carotid artery between the origins of the ophthalmic and the posterior communicating arteries and project medially.1 Consequently, these aneurysms are intradural and may result in subarachnoid hemorrhage. SHA aneurysms have also been classified as paraclinoid aneurysms along with carotid cave, carotid ophthalmic, and posterior carotid wall aneurysms.2,3 Due to anatomic obstacles in this area, surgical clipping of SHA aneurysms is invariably challenging. Thus, endovascular therapy has been used frequently to treat these aneurysms in many centers, both here and abroad. It has been our observation that SHA aneurysms can be treated easily by endovascular means with remarkable short-term results. The rarity of these lesions has, however, precluded any quality studies assessing the effectiveness of endovascular therapy. We present the results of the largest series that assesses the safety and efficacy of endovascular therapy for SHA aneurysms.
Materials and Methods
We searched our data base for patients with SHA aneurysms who were treated with endovascular therapy at our institution between January 2006 and February 2011. Aneurysms arising from the internal carotid artery segment between the ophthalmic and posterior communicating arteries and projecting medially, as assessed by the senior author, were included in the study. Eighty-seven patients met our inclusion criteria. All patients had been offered endovascular therapy as a primary treatment option for their aneurysms. Thirty-five patients were treated with coil embolization; 45, with stent-assisted coiling; 4, with balloon-assisted coil embolization; and 3, with a flow-diversion technique (Figs 1 and 2). Aneurysms were embolized by using only bare metal coils (no bioactive coils were used). Stents were used for aneurysms with wide necks, for aneurysms with an unfavorable neck-to-dome ratio, and for rescue in case of coil prolapse into the parent vessel. Balloon assistance was typically indicated for parent vessel protection in ruptured wide-neck aneurysms, but this was based somewhat on operator preference.

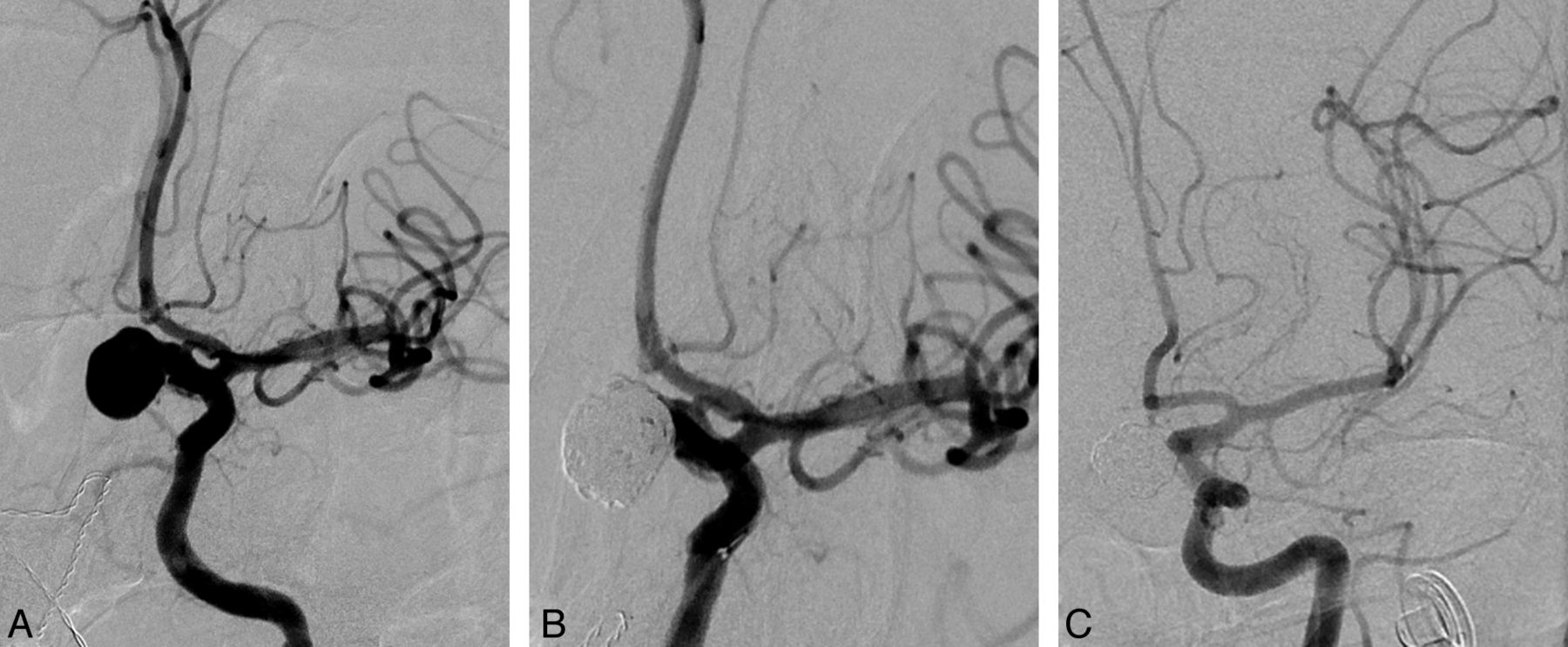
Frontal views of DSA of the left internal carotid artery, demonstrating a large SHA aneurysm in a 58-year-old woman (A). The aneurysm was treated with coil embolization (B) and showed complete occlusion at 6-month follow-up angiography (C).

Frontal views of DSA of the left internal carotid artery, showing a 5.5-mm SHA aneurysm pointing medially in a 36-year-old woman (A). The aneurysm was successfully embolized by using a stent-assisted technique (B) and progressed to complete occlusion on the 6-month follow-up angiogram (C).
Medical charts and initial and follow-up angiograms were retrospectively reviewed to determine the patient age, sex, size of the aneurysm, associated aneurysms, ruptured/unruptured aneurysm status, type of endovascular procedure, procedural complications, immediate and follow-up angiographic results, and rate of hemorrhage/rehemorrhage.
Excluding 1 patient in whom endovascular treatment failed and 1 patient who died as a result of a high-grade subarachnoid hemorrhage, follow-up imaging was available in 76 (89.4%) patients (DSA in 65, MRA in 11). Only 10.6% of patients (9/85) were lost to follow-up. Last available follow-up was at 6 months for 54 patients, at 1 year for 11 patients, at 2 years for 9 patients, and at 5 years for 2 patients. The mean angiographic follow-up was 10.4 months. Regardless of the need for further intervention, any recurrence, no matter how minimal, was categorized as a recurrence.
Results
Demographics and Aneurysm Characteristics
Of the 87 patients, 79 were women (90.8%) and 8 were men (9.2%). The mean age in the series was 51.1 years, with a range of 24–76 years and a median of 47 years. Mean aneurysm size was 6.0 mm, with a range of 2.5–15 mm and a median of 7 mm (Table 1). Of the 87 aneurysms, 12 were ruptured (13.8%) and 75 were unruptured (86.2%). Twenty-three patients had at least 1 aneurysm at another location (26.4%), 10 patients had ≥2 aneurysms at other locations (11.5%), and 14 patients had at least 1 associated paraclinoid aneurysm (16.1%). All associated aneurysms were located in the anterior circulation (100%), with paraclinoid aneurysms accounting for most of these (55.9%) (Table 2).
Size of SHA aneurysms
Anatomic location of aneurysms associated with SHA aneurysms
Endovascular Treatment
Of the 87 patients who underwent endovascular therapy, 35 were treated with coil embolization; 45, with stent-assisted coiling; 4, with balloon-assisted coil embolization; and 3 with flow diversion. One patient in the coil embolization group had an unsuccessful procedure due to coil prolapse into the parent vessel. She later underwent surgical clipping.
Minor complications occurred in 2 patients (2.2%). One patient in the coil embolization group had a minor groin hematoma that resolved spontaneously. Another patient in the coil embolization group had angiographic evidence of extravasation into the cavernous sinus (with no extravasation in the subarachnoid space). This was easily controlled with coils, and the patient was asymptomatic and neurologically intact after the procedure. No major complications were observed in the series. There were no deaths or permanent morbidity related to the procedure.
Immediate Angiographic Results
Excluding the patient who had a failed procedure and the 3 patients who were treated with a flow-diversion technique, complete aneurysm occlusion (100%) was achieved in 50.6% of patients (42/83), near-complete occlusion (95%–100%) in 47.0% (39/83), and incomplete occlusion (<95%) in 2.4% (2/83). The initial angiographic results for the different endovascular modalities are summarized in Table 3.
Immediate angiographic results for aneurysms treated with different endovascular techniques
Follow-Up Angiographic Results and Rate of Hemorrhage/Rehemorrhage
Of the 65 patients with DSA follow-up (75.5%), 62 (95.4%) showed stable or complete occlusion of their aneurysms at the last available follow-up. Three patients (4.6%) had evidence of a recurrence, and only 1 patient (1.5%) required further intervention (Tables 3–5). The first patient showed a 20% recurrence on the 6-month follow-up angiogram after initial treatment with coil embolization. She was successfully treated with additional coil embolization and maintained 100% occlusion at the 6-month angiographic assessment. The second patient had a 10% recurrence at 6-month follow-up angiography after initial obliteration with coils. This did not require further intervention, but the patient was lost to follow-up. The third patient showed only a slight decrease in the size of his aneurysm at the 6-month follow-up after treatment with a flow-diversion stent technique. No recurrences were noted in patients who underwent stent-assisted coil embolization or balloon-assisted coil embolization. Among the 41 patients in whom <100% aneurysm occlusion was initially achieved, 29 had an available DSA follow-up and 17 (58.6%) showed progression to complete aneurysm occlusion (Table 6).
Angiographic outcome in 76 patients treated with endovascular techniques
Patients with recurrences after initial endovascular treatment
Initial and follow-up DSA results for patients treated with endovascular therapy
None of the 11 patients who underwent MRA follow-up had evidence of a recurrence. Overall, among the 76 patients in whom follow-up imaging was available (MRA or DSA), 3 patients (3.9%) had a recurrence and only 1 had to be retreated (1.3%). No early or late hemorrhage was observed after initial treatment in the series.
Discussion
SHA aneurysms are a rare type of intracranial aneurysm. Data pertaining to the characteristics and management of these lesions are extremely scant. Their treatment has therefore been based mainly on comparison with the wider heterogeneous group of paraclinoid aneurysms and varies with the preferences and experience of different centers. Treatment options include open surgery or endovascular techniques. We have offered endovascular therapy as the primary treatment option for all patients with SHA aneurysms who presented to our institution because we believe that these lesions are effectively managed with endovascular means while being particularly challenging for open surgery. We have assessed the safety and efficacy of endovascular therapy in the largest series of SHA aneurysms to date.
An interesting finding of our study is the extreme female sex predominance (90.8%) for SHA aneurysms. This has been previously reported in several paraclinoid aneurysm series, though it was not as pronounced as in our study.2,4⇓⇓–7 It seems that female sex predominance is a hallmark of paraclinoid aneurysms in general and SHA aneurysms in particular. We are unable to provide a plausible explanation for this finding. The tendency toward multiple aneurysms is another unique characteristic of SHA and paraclinoid aneurysms.6,8⇓⇓–11 In the present series, 26.4% of patients had multiple aneurysms with most of these arising from the paraclinoid segment or the posterior communicating artery (73.5%). Most interesting, none of the 34 associated aneurysms were located in the posterior circulation. This finding could indicate that specific local factors exerting their action mainly in the anterior circulation may be implicated in the pathogenesis of SHA aneurysms. Patients presenting with subarachnoid hemorrhage accounted for only 13.8% of all those in our series. Whether SHA aneurysms have a characteristically low risk of rupture requires more investigation because the design of this study is not suitable for assessing the natural history of these lesions. The size of SHA aneurysms was quite large in our series (6 mm on average), which is a common finding for paraclinoid aneurysms in general.11⇓–13
Surgical clipping of SHA aneurysms can be technically challenging. Obtaining proximal control, drilling of the anterior clinoid process to allow adequate exposure of the aneurysm, and opening the dural ring may add potential surgical morbidity. The procedure carries a risk of injury to the optic apparatus and other surrounding structures. It is also difficult during clip placement to preserve the patency of the small perforating branches supplying the optic chiasm and the pituitary gland, especially for large aneurysms. Despite recent advances in microsurgical techniques, the rate of complications related to surgical clipping of paraclinoid aneurysms—including SHA aneurysms—is still significant. Recent series have reported complication rates ranging from 15% to 35% with mortality rates as high as 3%–6%.4,14⇓–16 These rates are well above those observed with endovascular therapy in this series. We found a remarkable 0% and 2.2% risk of major and minor complications, respectively. In addition, there was no procedure-related permanent morbidity or mortality.
We also found an exceptionally low recurrence rate of 3.9% at follow-up. Furthermore, the rate of recurrence requiring further intervention was as low as 1.3%. This is, to our knowledge, the lowest recurrence rate reported for any type of aneurysm with endovascular therapy. To put this into perspective, the recurrence rate is 24%–35% for posterior circulation aneurysms,17,18 18%–32% for middle cerebral artery aneurysms,19 37% for posterior communicating artery aneurysms,20 25% for anterior communicating artery aneurysms,20 26% for carotid ophthalmic artery aneurysms,20 40% for cavernous aneurysms,21 and 12%–29% for all paraclinoid aneurysms.4,5,11,22 One plausible explanation for the observed low recurrence rate after endovascular therapy is the fact that SHA aneurysms are sidewall aneurysms projecting medially, which prevents the direct jet flow of blood from entering the aneurysm sac, hence, favoring stasis and thrombosis. This would also explain why bifurcation or end-vessel aneurysms tend to recur after endovascular treatment. In our series, no hemorrhages were observed after initial endovascular treatment, which shows that SHA aneurysms can be reliably secured with endovascular therapy.
We are aware of only 1 study that assessed the safety and efficacy of endovascular therapy for SHA aneurysms specifically. In this study, Gurian et al6 performed coil embolization in 11 patients with SHA aneurysms that were considered to be at high risk for surgery. They had no procedure-related complications and reported aneurysm recanalization in 1 of 7 patients at follow-up angiography. The authors concluded that coil embolization was an excellent alternative for treating SHA aneurysms. Although the results of this study are in line with our findings, the sample size was too small to draw any firm conclusions. Moreover, no patients were treated with stent or balloon-assisted coiling techniques. In other series, small samples of SHA aneurysms were included along with other paraclinoid aneurysms. The rate of recurrence at follow-up ranged from 12% to 29%, and complications were seen in 3%–7% of patients.4,5,11,22 However, no separate analysis was done for SHA aneurysms specifically to identify this seemingly unique category in the large heterogeneous group of paraclinoid aneurysms. Furthermore, because of the nonavailability of stents at the time these studies were conducted, none of the patients were treated with stent-assisted coil embolization.
In fact, many SHA aneurysms are complex with wide necks and, thereby, require stent-assisted techniques. Besides preventing coil herniation into the parent vessel, stent deployment diverts blood flow away from the lumen and enhances thrombosis in the aneurysm.23 In the present series, while 2 recurrences and 2 complications occurred in patients treated with coil embolization, none were noted in the stent group. Although the number of events is too small to allow any statistical analysis, stent techniques seem to have the highest occlusion rates and the lowest complication rates for SHA aneurysms. Overall, regardless of the technique, endovascular therapy has an unparalleled safety-efficacy profile and should be considered the procedure of choice for the treatment of SHA aneurysms. Surgery should be reserved for patients in whom endovascular therapy is unsuccessful.
One limitation of our study is the lack of comparison with a control group that was treated with surgery. Because most centers, including ours, prefer to manage SHA aneurysms with endovascular therapy, we believe that it is very difficult to design a study with a control surgical group. Other limitations of this study stem from its retrospective design and the lack of angiographic follow-up in 10.6% of patients. Given the relatively short-term nature of the angiographic follow-up in this series, longer follow-up periods are required to ascertain that endovascular therapy provides durable aneurysm closure.
Conclusions
In this study, we present the results of the largest series of SHA aneurysms to date. We found an extreme female sex predominance for these lesions and a high incidence of associated aneurysms in the anterior circulation (exclusively). We were also able to demonstrate that endovascular therapy has a remarkably low rate of complications for SHA aneurysms. The rate of recurrence after endovascular treatment is the lowest for SHA aneurysms compared with aneurysms in other locations by using historical data. Endovascular therapy should therefore be considered the procedure of choice for the treatment of SHA aneurysms. Stent-assisted coiling seems to be the preferred endovascular technique. Surgery should be considered as an alternative whenever endovascular treatment fails.
Footnotes
Disclosures: Stavropoula Tjoumakaris—UNRELATED: Consultancy: Stryker Neurovascular, Comments: Speakers Bureau. Aaron Dumont—UNRELATED: Consultancy: MicroVention, ev3, Comments: consultant for technology development.
References
- Received October 18, 2011.
- Accepted after revision December 7, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.