
Abstract
BACKGROUND AND PURPOSE: The prevalence of tympanic plate fractures, which are associated with an increased risk of external auditory canal stenosis following temporal bone trauma, is unknown. A review of posttraumatic high-resolution CT temporal bone examinations was performed to determine the prevalence of tympanic plate fractures and to identify any associated temporal bone injuries.
MATERIALS AND METHODS: A retrospective review was performed to evaluate patients with head trauma who underwent emergent high-resolution CT examinations of the temporal bone from July 2006 to March 2012. Fractures were identified and assessed for orientation; involvement of the tympanic plate, scutum, bony labyrinth, facial nerve canal, and temporomandibular joint; and ossicular chain disruption.
RESULTS: Thirty-nine patients (41.3 ± 17.2 years of age) had a total of 46 temporal bone fractures (7 bilateral). Tympanic plate fractures were identified in 27 (58.7%) of these 46 fractures. Ossicular disruption occurred in 17 (37.0%). Fractures involving the scutum occurred in 25 (54.4%). None of the 46 fractured temporal bones had a mandibular condyle dislocation or fracture. Of the 27 cases of tympanic plate fractures, 14 (51.8%) had ossicular disruption (P = .016) and 18 (66.6%) had a fracture of the scutum (P = .044). Temporomandibular joint gas was seen in 15 (33%) but was not statistically associated with tympanic plate fracture (P = .21).
CONCLUSIONS: Tympanic plate fractures are commonly seen on high-resolution CT performed for evaluation of temporal bone trauma. It is important to recognize these fractures to avoid the preventable complication of external auditory canal stenosis and the potential for conductive hearing loss due to a fracture involving the scutum or ossicular chain.
ABBREVIATIONS:
- HRCT
- high-resolution CT
- TMJ
- temporomandibular joint
- TPF
- tympanic plate fracture
There are many reports in the literature describing CT of temporal bone trauma,1⇓⇓–4 detailing fracture plane orientations,4⇓–6 ossicular disruptions, otic capsule involvement,4,5 associations with air in the temporomandibular joint (TMJ),7 facial nerve injury,4⇓–6 and fracture mimics, to name a few broad categories.8 Temporal bone fractures involving the tympanic plate (Figs 1 and 2), however, are under-recognized and have received little attention beyond isolated case reports involving mandibular trauma.8⇓⇓⇓⇓⇓⇓–15 The tympanic plate of the temporal bone is a U-shaped structure forming the anterior wall, floor, and part of the posterior wall of the external auditory canal. The limited literature concerning tympanic plate fracture (TPF) suggests that these types of fractures are uncommon.4,10,11,16 Most literature on direct and indirect CT findings of temporal bone trauma was published in the pre-/early multidetector CT era1,3,7,17,18 or was based solely on non-high-resolution CT (HRCT) imaging,19; however, it is possible that posttraumatic TPFs are under-recognized or overlooked by the inexperienced observer. TPFs are important to identify, given the potential for the clinically significant long-term complications of external auditory canal stenosis and trismus.20 The purpose of this study was to retrospectively review acute posttraumatic HRCT temporal bone studies to determine the true incidence of TPF and to identify other associated temporal bone injuries.

External sagittal view of the left temporal bone depicting the tympanic plate as it forms part of the anterior wall of the external auditory canal.

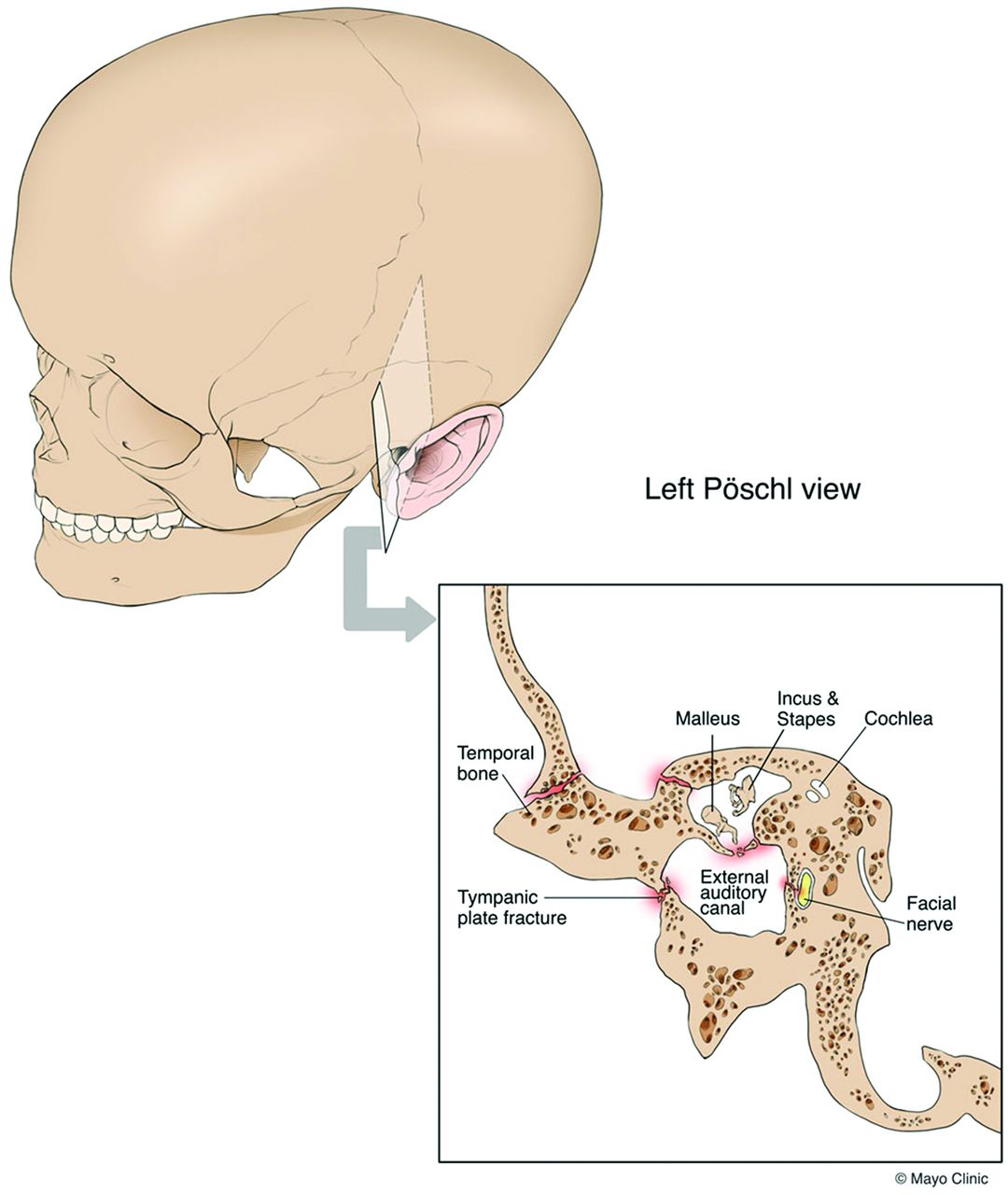
Oblique 3D view of the skull, including the external portion of the left temporal bone and the Pöschl plane for CT reformatting superimposed. This Pöschl plane view is depicted in the inset along with a TPF and some of the possible associated traumatic injuries.
Materials and Methods
Institutional review board approval with waived consent was obtained for this Health Insurance Portability and Accountability Act–compliant research study. A retrospective review was under taken of patients with acute trauma who underwent a HRCT examination of the temporal bone at a level 1 trauma center from July 2006 to March 2012. Two hundred sixty-three patients were identified on the basis of a search of a radiology report database during this time for CT reports containing the keywords “temporal bone” and “fracture,” followed by a visual review of each study to confirm the presence of a definable fracture through the temporal bone on HRCT, which yielded 58 patients. Studies were excluded if they were performed as a follow-up to a prior temporal bone HRCT, were not acquired using a HRCT temporal bone protocol, were of unacceptable image quality due to excessive motion/dental scatter, or were performed for ballistic injuries (19 patients). This process yielded 39 patients, 7 of whom had bilateral fractures that were analyzed as 2 separate cases, producing a total of 46 HRCT temporal bone fractures that met the inclusion criteria.
HRCT of the temporal bone had been acquired without contrast on either a Definition, Definition AS+, or Definition Flash scanner (Siemens, Erlangen, Germany), using 12 × 0.3 mm or 16 × 0.3 mm collimation, 120 kV(peak), 0.8 pitch, and a 300-mm FOV. The source data were reconstructed into 0.5-mm sections at 0.3-mm increments in the axial, coronal, and Pöschl planes (Fig 3A) by using a bone kernel algorithm. These 46 HRCT cases were then reviewed on a PACS workstation by 3 neuroradiologists (C.P.W., C.H.H., and J. L.), each with a Certificate of Added Qualification, and a neuroradiology fellow (D.C.B.), respectively, for consensus diagnosis. At the review, readers were blinded to the original radiology report and clinical history. Consensus review was performed to ensure that the interpretation generated was representative of a typical group of neuroradiologists and to decrease any expectation bias. Each of the above 3 planar reformats was reviewed before a finding was determined, and subtle findings were confirmed by comparison with the opposite side in cases of unilateral fractures.

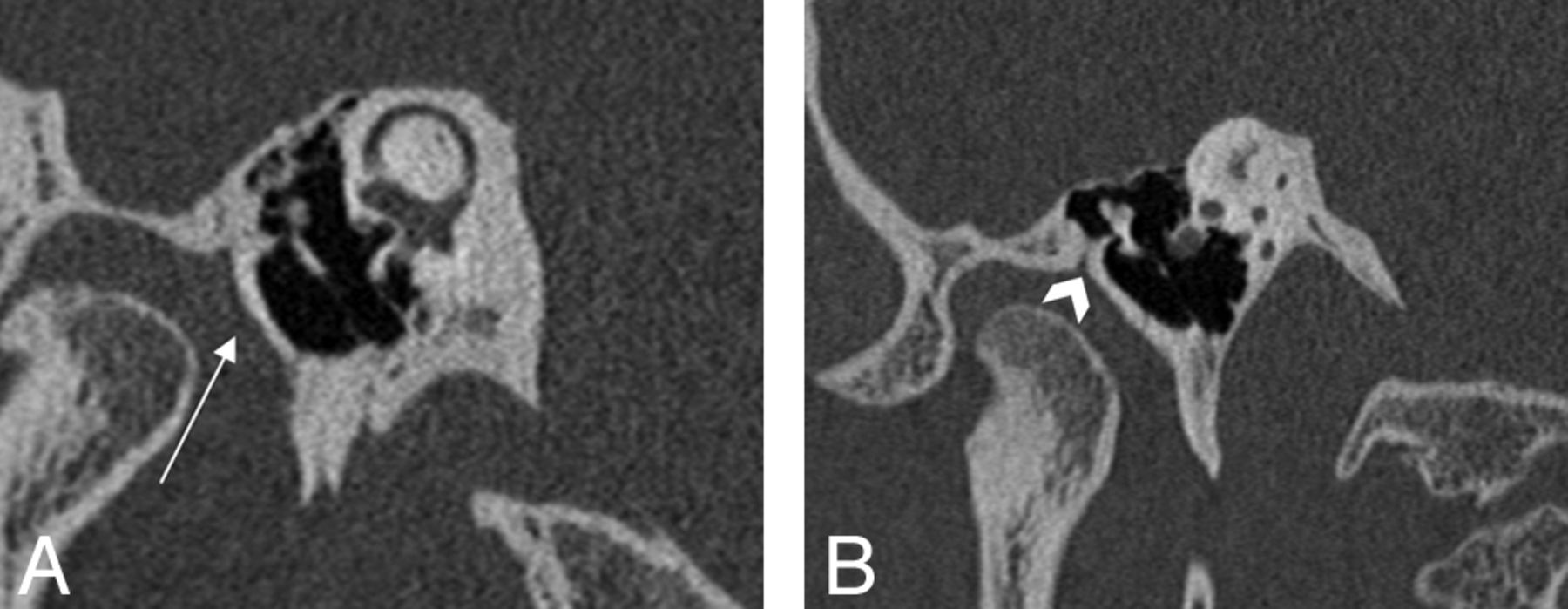
HRCT images with Pöschl views in the same patient demonstrating the tympanic plate (A, white arrow) and the petrotympanic fissure (B, arrowhead).
Cases were assessed for multiple variables. The fracture plane orientation was classified as either transverse, longitudinal, or mixed. These planes were determined relative to the axis of the petrous ridge, with fracture orientations considered longitudinal if <30°, transverse if >70°, or mixed if a combination of both planes was present.4 TPF was confirmed if there was a visible fracture extending through the tympanic plate that was clearly distinct from the petrotympanic fissure (Fig 3B). Fracture extension through the otic capsule was assessed for involvement of the vestibule, semicircular canals, and/or cochlea. The entire course of the facial nerve through the temporal bone was followed for the presence of fracture involvement, including the tympanic and mastoid segments. Facial nerve canal fracture was designated if there was a clear intersection between the course of the fracture and the labyrinthine segment or anterior genu of the facial nerve, while perigeniculate involvement was determined if the fracture line passed within 2 mm of the anterior genu on any planar reformat.
The scutum and internal auditory canal were examined for any fracture involvement. Ossicular integrity was assessed for the presence of subluxation/dislocation of either the malleoincudal joint, incudostapedial joint, or both. Ossicular complex displacement was determined if the entire ossicular chain was notably displaced from its expected location due to either ligamentous rupture or fracture of bony attachment sites. Images were reviewed by using lung windows for the presence of pneumocephalus, pneumolabyrinth, or air in the TMJ fossa. The CT boundaries of the TMJ fossa were defined by its bony margins: anteriorly by the articular tubercle, posteriorly by the tympanic plate, and medially and laterally by the condylar head width. Images were evaluated for mandibular condyle dislocation or fracture.
An otolaryngology chief resident (M.L.C.) performed a retrospective review of each patient's electronic medical record, assessing any potential clinical consequences of the temporal bone trauma. Statistical analysis was performed using a commercially available software package (JMP, Version 9.0; SAS Institute, Cary, North Carolina). The Pearson χ2 test was used to determine the association between TPF and ossicular disruption; fracture plane orientation; fractures involving the otic capsule, facial nerve canal, scutum, or mandibular condyle; mandibular condylar dislocation; pneumocephalus; pneumolabyrinth; and TMJ gas. A P value < .05 was considered statistically significant.
Results
Thirty-nine unique patients (41.3 ±17.2 years of age; 33 men, 6 women) were identified who had undergone temporal bone HRCT in the acute setting. Seven of these patients had bilateral temporal bone fractures, which yielded a total of 46 distinct temporal bone fractures that were evaluated. The CT features of temporal bone fractures and TPF are listed in Table 1. The distribution of fracture orientations was transverse in 2 (4.4%), longitudinal in 18 (39.1%), and mixed in 26 (56.5%). The otic capsule was involved in only 4 cases (9%). Pneumocephalus was present in 16 cases (35%). TMJ gas was seen in 15 (33%) cases. TPFs were identified in 27 (58.7%) cases and were most conspicuous on the Pöschl view (Figs 4 and 5). Ossicular disruption was seen in 17 (37.0%) cases. Fractures involving the scutum were seen in 25 (54.4%) cases. None of the 46 temporal bone fractures, including the TPF cases, had an associated mandibular condyle dislocation or fracture. A fracture extending to involve the internal auditory canal occurred in only 1 (2%) case. Pneumolabyrinth was identified in only 1 (2%) case.
Clinical and CT features of temporal bone fractures

A 66-year-old intoxicated man, status post 2 falls within an hour, each of which led to his head striking a cement floor. Right tympanic plate fractures demonstrated on HRCT. Axial (A), Pöschl (B), and coronal (C) plane views. Tympanic plate fracture is demonstrated by white arrows.

A 21-year-old woman, status post motor vehicle collision, with bilateral tympanic plate fractures (only the right one is shown). The complex nature of the right tympanic plate fracture is demonstrated by the white arrows on the axial (A), Pöschl (B), and coronal (C) plane images.
Statistical analysis revealed the following positive associations with TPF (Table 2): Of the 27 cases of TPF, 14 (51.8%) had associated ossicular disruption (P = .016) and 18 (66.6%) had an associated fracture of the scutum (P = .044). There was no correlation between fracture plane orientation and TPF. In addition, fracture plane orientation was not predictive of ossicular disruption or scutum fracture. There was no statistical difference between unilateral-versus-bilateral temporal bone fractures and the frequency of TPF (P = .52). Twenty-two fractures were found that involved the course of the facial nerve in the temporal bone. Twenty-one of these involved the geniculate/perigeniculate region, and 1 involved the tympanic segment. There was no correlation between TPF and fractures involving the segments of the facial nerve (P = .56). The presence of gas within the TMJ fossa was not predictive of a TPF (P = .21). The review of the patient posttraumatic clinical courses was unrevealing, especially because clinical parameters were often incompletely documented.
Tympanic plate fractures and associations
Discussion
Fractures of the temporal bone are common in cases of major head trauma, with a reported incidence of 3%–22% in patients with skull fractures.5,21 Temporal bone fractures frequently have associated complications such as hearing loss, cranial neuropathy or dysfunction, CSF leak, and vestibulopathy occurring in 5%–10% of cases.22,23 Previously Schubiger et al6 noted that 48% of patients with temporal bone fractures had ossicular chain disruption, facial nerve damage, or a CSF leak.6 Subsequently, Dahiya et al5 reported a higher incidence of facial paralysis, CSF leaks, profound hearing loss, and more frequent intracranial complications when temporal bone fractures involved the otic capsule compared with those that spared the bony labyrinth. Patients with temporal bone fractures often have coexistent major intracranial injuries because a significant force is required to fracture the temporal bone.24
The tympanic part of the temporal bone is a U-shaped structure forming the anterior wall (or posterior margin of the glenoid fossa), floor, and part of the posterior wall of the external auditory canal. The tympanic plate is this anterior wall segment of the tympanic portion of the temporal bone, interposed between the external auditory canal and the glenoid fossa (Fig 1). The plate is subjacent to the squamous part of the temporal bone, from which it is separated by a contiguous set of fissures running along the anterosuperior external auditory canal: the squamotympanic fissure laterally and the petrotympanic fissure medially. The petrotympanic fissure permits passage of the chorda tympani nerve (via the canal of Huguier), fibers from the anterior ligament of the malleus, and the anterior tympanic branch of the internal maxillary artery.25 Identification of this contiguous fissure (best visualized in the Pöschl plane) is important to avoid mistaking it for a temporal bone fracture and in localizing the tympanic plate.
In our study, TPFs (Fig 2) were commonly seen on HRCT of the temporal bone in acute trauma. This finding is in contradistinction to the purportedly “rare” and “uncommon” occurrence of TPF reported in the literature.10,11,16 One explanation for this under-reporting could be that TPFs in our study were most conspicuous on the Pöschl plane, which is generally not included on routine CT examinations. Most interesting, a study in 1988 mentioned the benefits of direct sagittal CT in temporal bone evaluation including the external auditory canal and for TMJ trauma, but it did not mention TPF.26
Most, if not all, of the articles referencing a low incidence of tympanic plate injuries were written in the context of mandibular trauma, detailing a blow to the chin driving the mandibular condyles posteriorly and then impacting the tympanic plate. While this mechanism makes intuitive sense, none of our cases had evidence of a mandibular fracture or dislocation. In addition, in the present study the tympanic plate was typically never fractured in isolation, suggesting an alternative fracture mechanism. Both Valvassori27 and Ghorayeb and Yeakley28 briefly noted fracture extension into the glenoid fossa in most of their temporal bone fracture cases, often in association with a longitudinal or mixed fracture, respectively. Although specific mechanisms of injury were not provided, their studies appeared to be based on patient populations experiencing blunt nonpenetrating trauma, similar to our patient group.
In our study, there was a statistically significant association between ossicular injury and TPF. This could merely represent extension of an adjacent fracture plane, given the close anatomic relationship of the tympanic plate and the ossicles. Alternative mechanisms of ossicular injury due to TPF should also be considered, such as damage to the anterior ligament of the malleus. This ligament anchors the malleolar head to the anterior wall of the tympanic cavity and spina angularis of the sphenoid.25,29 However, to reach its sphenoid insertion, the fibers of the anterior ligament of the malleus must course through the petrotympanic fissure. Because the tympanic plate borders the petrotympanic fissure, a TPF could disrupt these passing fibers and lead to ossicular injury. A second explanation could be related to the lateral ligament of the malleus, which connects the malleolar neck to the osseous margins of the tympanic notch and runs inferior to the scutum.25 Given the correlation between fractures of the tympanic plate and scutum in our study, the association between TPF and ossicular injury could be due to lateral ligament damage from a scutum fracture. Regardless of which ligament is disrupted, either could destabilize the ossicles and transfer additional strain on the remaining ligaments and joints, ultimately contributing to ossicular injury.
Potential long-term complications of TPF are well-documented in the literature, including external auditory canal stenosis, TMJ dysfunction, prolapse of the mandibular condyle into the external auditory canal, and facial nerve paresis.9,10 External auditory canal stenosis can vary from mild to complete occlusion with variable degrees of conductive hearing loss. Stenosis presumably occurs from marked comminution and displacement of the tympanic plate, resultant loss of anterior wall structural integrity, callus formation, and fibrous inflammation.20 The management and treatment of external auditory canal stenosis are beyond the scope of this article, but the mainstay of preventive treatment is packing of the canal in cases at high risk for the development of stenosis. Early identification of this injury and medical management can reduce the need for surgery in cases of fixed stenosis. Surgery often involves canaloplasty to remove fixed narrowing and bony irregularities, excision of any soft-tissue stenosis, and/or skin grafting, often with restenosis rates as high as 27%.20 TMJ dysfunction is another possible long-term complication, though acutely there is usually trismus and pain due to regional soft-tissue and retrodiscal inflammation.10 For these reasons, it is important for the radiologist to document the presence of a TPF.
The present study has several limitations. This is a retrospective review and is limited as such. Cases were identified from a cohort of patients in whom some type of temporal bone fracture in an acute setting had been reported by a neuroradiologist. Hence, there exists the potential for having missed cases not appreciated by the initial neuroradiologist, thereby excluding more subtle cases of temporal bone trauma. There may be a referral bias because we are a tertiary care center. In addition, because our institution is a large referral center, many patients had limited or no long-term follow-up after their initial injury and acute care. Future work could include more detailed prospective clinical follow-up and outcomes for these types of patients.
Conclusions
TPFs are commonly seen on dedicated HRCT performed for the evaluation of acute temporal bone trauma, which is in contradistinction to previous literature concerning CT imaging of temporal bone trauma. TPFs were most conspicuous on the Pöschl view. It is important to recognize these fractures to avoid the preventable complication of external auditory canal stenosis and its potential impact on conductive hearing loss with a fracture involving the scutum or ossicular chain.
REFERENCES
- Received January 17, 2013.
- Accepted after revision March 29, 2013.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.