
Abstract
BACKGROUND AND PURPOSE: The infarctions arising in the long insular arteries of the M2 segment have been poorly described in the past. The purpose of this study was to investigate the incidence, clinical characteristics, and pathogenesis of long insular artery infarcts.
MATERIALS AND METHODS: Patients with acute isolated infarcts in territories of the long insular arteries and lenticulostriate arteries were retrospectively reviewed. The long insular artery territory was defined as the area above the lenticulostriate artery territory at the level of centrum semiovale. On the coronal section, it lies between the tip of the anterior horn and the top of the superior limb of the insular cleft. Clinical features and prevalence of embolic sources were compared between the 2 groups.
RESULTS: Of 356 consecutive patients with acute ischemic stroke, 8 (2.2%) had a long insular artery infarct (long insular artery group) and 50 (14.0%) had a lenticulostriate artery infarct (lenticulostriate artery group). There were no differences in age, sex, prevalence of risk factors, neurologic deficit, or incidence of lacunar syndromes between these groups. Abrupt onset was more common in the long insular artery than in the lenticulostriate artery group (P = .004). The prevalence of embolic high-risk sources (eg, atrial fibrillation) was not significantly different between these groups, but the combined prevalence of all embolic sources, including moderate-risk sources, was significantly higher in the long insular artery group (P = .048).
CONCLUSIONS: Isolated infarction caused by long insular artery occlusion is not rare. Abrupt onset is more common for long insular artery infarction, and this finding could be attributed to the higher incidence of an embolic etiology as the pathogenesis of infarction.
ABBREVIATIONS:
- LIA
- long insular artery
- LSA
- lenticulostriate artery
- TEE
- transesophageal echocardiography
- WMMA
- white matter medullary artery
Periventricular white matter has 2 major vascular territories supplied by the deep and superficial penetrating arteries.1⇓⇓⇓⇓⇓⇓–8 Among the deep penetrating arteries, the lenticulostriate arteries (LSAs) arise from the M1 segment of the MCA and supply the lower part of the corona radiata.7⇓⇓–10 The superficial penetrating arteries, namely the white matter medullary arteries (WMMAs), arise from the cortical branches of the MCA and feed the periventricular deep white matter.1⇓⇓⇓⇓–6 Several reports suggest that WMMA infarction should be distinguished from LSA infarction and treated differently because of their different clinical and etiologic backgrounds.4⇓–6
The long insular artery (LIA) is a unique supplier of the periventricular white matter. It is one of the medullary arteries in close vicinity to the territory of deep perforators. The LIA infarction has been recognized mainly by neurosurgeons because interruption of this artery during the resection of opercular glioma often results in postoperative hemiparesis and characteristic corona radiata infarction.9⇓⇓–12 This entity has, however, attracted much less attention from physicians in other fields.
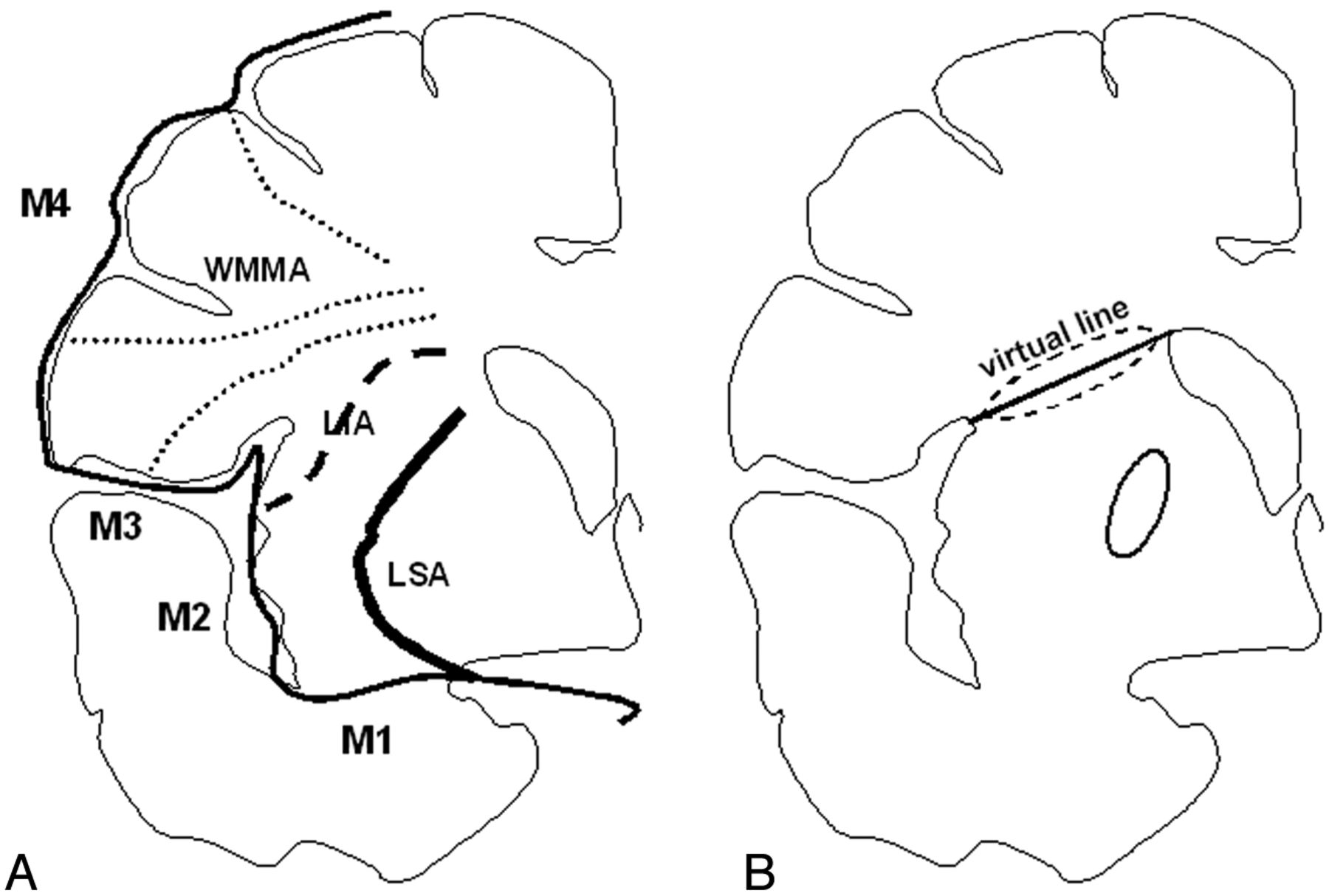
The LIA arises from the insular segment of MCA and has, therefore, been anatomically recognized as a subtype of the WMMA. The LIA has characteristics that are anatomically intermediate between the LSA and the WMMA, in that it supplies the insular cortex, extreme capsule, claustrum, and external capsule and quite often extends to the corona radiata (Fig. 1A).

Vascular territories of subcortical white matter and the basal ganglia on coronal images are schematically shown (figure based on a microangiogram of a postmortem brain section of Kumabe et al11). These areas are supplied with 3 individual arteries branching from the MCA, the LSA (bold line) from the M1 segment, the LIA (dashed line) from the M2 segment, and the WMMA (dotted lines) from the M3 or M4 segment (A). To standardize radiologic interpretation, interpreters drew the virtual line from the tip of the anterior horn to the top of the superior limb of the insular cleft (the A-I line), which almost corresponds to the vascular territory of the LIA. Then, subcortical infarctions involving the A-I line (dashed line circle) were categorized into the LIA group, and those situated under the A-I line (solid line circle) were classified as the LSA group (B).
Clinically, isolated LIA infarction is due to a single or a few occluded LIAs with no involvement of the main trunk of the insular artery. Hereafter, isolated LIA infarction is referred to as LIA infarction. The clinical features of LIA infarction have only rarely been reported11 because the sizes and shapes of LIA and LSA infarct lesions are similar and thus difficult to discriminate by using only transaxial MR imaging (Fig 2). These findings suggest that LIA infarcts are most likely frequently categorized as LSA infarcts. However, the LIA is a subtype of the WMMA; therefore, characteristics of LIA infarcts remain poorly investigated. To address these issues, we conducted a retrospective chart review to compare the occurrence, clinical features, and pathogenesis of LIA infarctions with the more commonly encountered LSA infarctions.

Axial and coronal reconstructed images from diffusion-weighted MR imaging in patients with an LIA infarct (A–C) and an LSA infarct (D–F) are shown. In each axial image, a small infarct of similar size can be observed. No apparent difference could be found between them. A, B and D, E: However, the coronal reconstructed images demonstrate that the former (C) is horizontally located from periventricular white matter to the top of the insular cortex or extreme capsule, while the latter (F) extends vertically (longitudinally) from the periventricular white matter to the putamen.
Materials and Methods
Definition of Vascular Territories
According to the figure of the coronal microangiogram of a postmortem brain obtained by Kumabe et al,11 the subcortical white matter and basal ganglia on coronal images was divided into the 3 individual vascular territories: the WMMA territory, the LIA territory, and the LSA territory, as shown in Fig 1A. The fact that stroke associated with sacrificed insular perforators during resection of an opercular glioma was located from the top of the insular cortex to the periventricular corona radiata is in accordance with this anatomic vascular distribution.11 In this study, to standardize radiologic interpretation, we drew a virtual line from the tip of the anterior horn to the top of the superior limb of the insular cleft in reference to the microangiogram of the LIA11 (referred to as the A-I line), because this corresponds closely to the previously reported vascular territory of the LIA (Fig 1B).9,10 Radiologic classifications were independently made by 1 neurologist with 10 years of experience under the supervision of a neuroradiologist with >20 years of experience, and by 1 neuroradiologist with 13 years of experience. When these investigators reached different decisions, the judgment from the neurologist supervised by the neuroradiologist was adopted. They were instructed to classify those infarctions involving the A-I line into the LIA group and to classify those situated under the A-I line and extending vertically (craniocaudal) as the LSA group. (Infarctions presenting over the A-I line were not included in this report.)
Patient Selection
With institutional ethics committee approval, clinical records of all patients with ischemic stroke who presented at our hospital between April 2003 and August 2010 and underwent MR imaging, including DWI and MRA, within 7 days of symptom onset were retrospectively reviewed. Patients with an isolated infarct in the LIA or LSA territories were included in this study. On the basis of the geographic distribution of a hyperintense area on coronal reconstructed images from DWI, patients were classified into the LIA group or LSA group, as described above (Figs 1 and 2). Patients with multiple infarcts or a large subcortical infarct (>15 mm) were excluded.
Clinical and Demographic Data
The following clinical data were obtained on each patient: 1) age; 2) sex; 3) vascular risk factors including hypertension, diabetes mellitus, hyperlipidemia, and smoking; 4) blood pressure value on admission; 5) NIHSS score on admission; 6) classic lacunar syndrome, which consisted of pure motor stroke, pure sensory stroke, sensorimotor stroke, ataxic hemiparesis, and dysarthria–clumsy hand syndrome; 7) mode of neurologic symptom onset, being either abrupt, gradual, or on awakening; 8) frequency of poor outcome, defined as a modified Rankin Scale ≥3 at 3 months after onset; and 9) embolic sources.
We also identified the following vascular risk factors: hypertension, defined as prior diagnosis or blood pressure >140/90 mm Hg persisting for >2 weeks after admission; diabetes mellitus, defined as prior diagnosis or fasting serum blood glucose >126 mg/dL or hemoglobin A1c >6.5%; hyperlipidemia, defined as prior diagnosis or fasting, serum low-attenuation lipoprotein cholesterol >140 mg/dL or fasting serum total cholesterol >220 mg/dL; and smoking, defined as regular daily cigarette use within the past 2 years.
Mode of neurologic symptom onset was defined in the following manner: abrupt, an abruptly started single episode reaching maximum severity within 30 minutes after onset; gradual, an episode reaching maximum severity >30 minutes after onset with gradually progressing or fluctuating symptoms; and on awakening, an episode with stroke symptoms noticed on awakening.
In this study, embolic sources included both cardiac and aortic sources. On the basis of a previously described definition, cardiac sources of embolism were further divided into groups associated with embolic high-risk sources and embolic moderate-risk sources.13 Atrial fibrillation, left ventricular aneurysm or thrombus, left atrial thrombus, recent transmural anterior myocardial infarction, rheumatic valvular disease, mechanical prosthetic valve, endocarditis, and primary intracardiac tumors were regarded as embolic high-risk sources. Embolic moderate-risk sources consisted of mitral annular calcification, mitral valve prolapse, cardiomyopathy, segmental wall-motion abnormality, patent foramen ovale, atrial flutter, sick sinus syndrome, valve strands, and left atrial spontaneous echo contrast. Aortic sources of embolism included ipsilateral occlusive arterial disease and aortic atheroma. Criteria for occlusive arterial disease were the presence of stenosis ≥50% by the NASCET criteria14 or occlusion in the ipsilateral extracranial carotid artery and stenosis ≥50% or occlusion in the ipsilateral intracranial carotid artery by measurement with MRA. Aortic atheroma was defined as an aortic plaque with thickness of ≥4 mm, mobile elements, or ulceration on transesophageal echocardiography (TEE). All patients underwent 12-lead electrocardiography, 24-hour electrocardiography monitoring, color-flow duplex carotid sonography, and transthoracic echocardiography to detect an embolic source. TEE was suggested to patients showing abrupt onset with no embolic source and was performed after informed consent was obtained.
MR Imaging
MR imaging was performed on a 1.5T MR imaging unit (Intera Achieva Pulsar scanner; Philips Healthcare, Best, the Netherlands) with echo-planar capabilities. An acquisition time of approximately 4 minutes was used for DWI. Images were acquired by using a single-shot echo-planar imaging technique with the following parameters: 6000/88 ms (TR/TE), with a motion-probing gradient in 15 orientations; b-value = 1000 s/mm2; and averaging 2 times. A parallel imaging technique was used to record data with a 128 × 128 spatial resolution for a 230 × 230 mm FOV. A total of 41 sections were obtained, with a section thickness of 3 mm and no intersection gap. Coronal DWI was reconstructed from DWI data by using the multiplanar reconstruction of the PACS.
Analyses
Statistical analysis was undertaken by using a commercially available software package (Statistical Package for the Social Sciences for Windows, Version 11; IBM, Armonk, New York). The degree of interrater agreement was determined by calculation of the κ statistic. Baseline characteristics were compared with a χ2 test (for proportions), a t test (for means), or a Mann-Whitney test (for medians), between the 2 groups. Differences with a P value < .05 were considered statistically significant.
Results
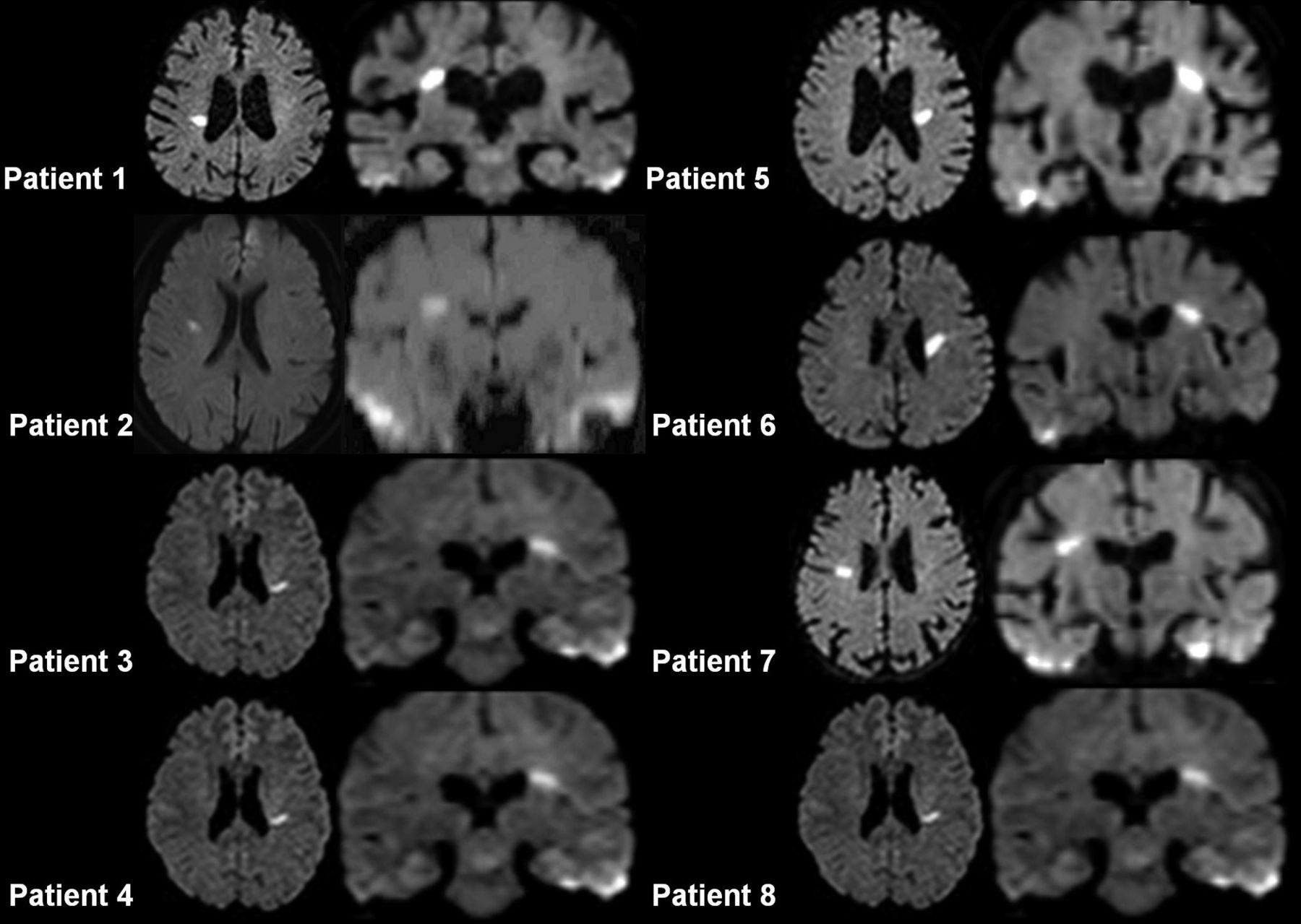
Among 356 consecutive patients with acute ischemic stroke, there were 8 (2.2%) patients with an LIA infarct (LIA group) and 50 (14.0%) with an LSA infarct (LSA group). The strength of inter-rater agreement for the classification was very good (κ = 0.923; 95% CI, 0.847–1.000). Axial and coronal reconstructed DWI from all cases of the LIA group are shown in Fig 3. Clinical and demographic features of the LIA and LSA groups are shown in the Table. Four patients in the LIA group and 4 patients in LSA group underwent TEE. No significant differences were seen between the 2 groups in sex, age, vascular risk factors, and blood pressure on admission.

Axial and coronal reconstructed images from DWI of each patient with a long insular artery infarct. Coronal reconstructed images show that infarcts are horizontally located from the anterior horn to the top of the insular cortex and involve the A-I line.
Demographic and clinical features of patients with long insular artery infarction (LIA group) and lenticulostriate artery infarction (LSA group)
All patients with an LIA infarct and most patients with an LSA infarct (86%, 43/50) had classic lacunar syndromes. Seven patients exhibiting nonlacunar symptoms in the LSA group included 3 patients with major hemispheric symptoms, 3 with pure dysarthria, and 1 with monoparesis.
The LIA group included 3 pure motor stokes (37.5%) and 1 pure sensory stroke (12.5%). The remaining 4 patients (50%) exhibited ataxic hemiparesis or its variant, dysarthria–clumsy hand syndrome. The median NIHSS score in the LIA group on admission was 1.5, showing no significant difference from that in the LSA group. Modified Rankin Scale scores at 3 months after onset ranged from 0 to 2. No significant difference in the frequency of poor outcome (%) was observed between groups.
Regarding the onset of neurologic symptoms, abrupt onset was significantly more frequent in the LIA than in the LSA group (63% versus 12%, respectively; P = .004), while gradual onset was more frequent in the LSA than in the LIA group (25% versus 78%, respectively; P = .006).
The prevalence of embolic high-risk sources was not different between the 2 groups (1 patient with atrial fibrillation in the LIA group [13%] compared with 4 patients with atrial fibrillation in the LSA group [8%]). On the other hand, embolic moderate-risk sources were significantly higher in the LIA than in the LSA group (2 patients with patent foramen ovale in the LIA group [25%] compared with 0% in the LSA group; P = .01); thus, the combined prevalence of embolic high-risk sources and moderate-risk sources was significantly higher in the LIA than in the LSA group (37.5% versus 8.0%, respectively; P = .048). Neither ipsilateral occlusive arterial disease nor aortic atheroma was observed in either group.
Discussion
This study, which is the first to clarify the clinical characteristics of LIA infarction, resulted in 3 major findings.
First, it clarified the incidence of LIA infarction at an unexpectedly high rate of 2.2% of all strokes. One of the reasons that LIA infarction has been less recognized as a type of subcortical stroke in previous studies is probably due to the difficulty of its detection. Tûre et al10 reported that the diameters of the LIA and LSA were so similar that size-based discrimination between these vessels was difficult. However, they also reported that there was no communication observed between them. These observations suggest that these 2 entities can be distinguished on the basis of their geographic distribution (especially on coronal images, in which both the LIA and the LSA run parallel to the imaging section). In fact, the present discrimination criteria based on coronal DWI had quite a high level of interrater agreement, suggesting that coronal DWI can be the key to identifying LIA infarcts.
Second, this study showed that all patients with an LIA infarct demonstrated classic lacunar syndromes, similar to those with LSA infarcts. In a previous study investigating the clinical differences between WMMA and LSA infarction, the incidence of nonlacunar syndromes was significantly higher in WMMA infarcts (observed in approximately half) than in LSA infarcts.6 Most interesting, clinical symptoms of LIA infarction resemble those of the LSA infarction rather than WMMA infarction, though the LIAs are anatomically recognized as a subtype of the WMMA. This feature also suggests that LIA infarcts cannot be distinguished from LSA infarcts by clinical symptoms alone. The clinical difference between WMMA and LIA/LSA infarcts was probably caused by different attenuations of the subcortical pyramidal tract fibers, which are denser in the middle and lower part supplied by the LIA or LSA rather than in the upper part supplied by the WMMA.
Finally, the present study showed that 5 of 8 patients with LIA infarcts (63%) experienced an abrupt onset of symptoms, which was less commonly observed in the LSA group. This finding implies that an embolic etiology is more common in the pathogenesis of LIA infarcts than in LSA infarcts. Although the prevalence of high-risk embolic sources was not significantly different between the 2 groups, the fact that the combined prevalence of embolic high-risk sources and moderate-risk sources was higher in the LIA (38%) than in the LSA group (8%) might provide supportive evidence for this speculation. Most important, an embolic mechanism has also been suggested for WMMA infarction.3⇓⇓–6 Because LIAs are a subtype of WMMA, the pathogenesis of the LIA infarction could be similar to that of the WMMA infarction. The size or shape of LIA and LSA infarcts corresponds with so-called lacunar infarction, for which stroke physicians often place a low priority for the evaluation of embolic sources and frequently recommend antiplatelet agents, because this pathology has been regarded as a small-vessel disease. Our results imply that LIA infarction represents a subgroup requiring attention in terms of embolism and might warrant proper secondary preventive measures, including administration of anticoagulants like warfarin.
This study was limited in the identification of embolic sources because TEE was not performed in all patients. Because it is not common to recommend that patients with lacunar syndrome undergo TEE, selection bias might be present. More than half of the LIA group and <10% of the LSA group underwent TEE. This discrepancy is partially due to the lower frequency of abrupt onset in LSA infarctions and implies that the incidence of embolic sources in LSA infarction might be underestimated. On the other hand, no embolic sources were detected in 4 TEE results from the LSA group, even though all showed abrupt onset. Such an ambiguity should be clarified in a further prospective study with a detailed protocol of echocardiographic evaluation.
Conclusions
LIA infarction was found to be more common than previously thought and possess clinical characteristics similar to those of LSA infarction. Furthermore, embolic phenomena might be a more common etiologic factor in LIA than in LSA infarctions. Data collection with a section thickness of 3 mm and no intersection gap15 enabling coronal reconstruction can be the key to identifying LIA infarcts, to draw the attention of clinicians to the possibility of embolism. Prospective large-scale studies are needed to make clear the etiologic characteristics of LIA infarcts.
Footnotes
Disclosures: Takashi Kasai—RELATED: Grant: The Japan Heart Foundation/Bayer Yakuhin Research Grant Abroad. Kei Yamada—UNRELATED: Consultancy: Lundbeck Japan, Grants/Grants Pending: JSPS Kakenhi,* Payment for Lectures (including service on Speakers Bureaus): Daiichi-Sankyo, Bayer, Eisai, Kyorin, Mitsubishi-Tanabe Pharma, Nippon Medi-physics, Philips Healthcare, Siemens, Sanofi, Aventis, Termo, Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Daiichi-Sankyo, Bayer, Eisai, Kyorin, Mitsubishi Tanabe Pharma, Nippon Medi-physics, Philips Healthcare, Siemens, Sanofi-Aventis, Termo. *Money paid to the institution.
This work was supported by a grant from The Japan Heart Foundation/Bayer Yakuhin Research Grant Abroad (T.K.).
REFERENCES
- Received January 23, 2013.
- Accepted after revision June 10, 2013.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.