
Abstract
BACKGROUND AND PURPOSE: In acute stroke, CTP is often used to visualize the endangered brain areas, including the ischemic core and the penumbra. Our goal was to assess the evolution of the infarct after mechanical thrombectomy and to analyze the interventional factors determining the fate of the penumbra.
MATERIALS AND METHODS: All patients receiving mechanical thrombectomy in the anterior circulation and receiving CTP beforehand were identified. The infarct volume was specified. The clinical parameters, outcome, and interventional results were correlated with the CTP and the final infarct size.
RESULTS: In total, 73 patients were included. After mechanical thrombectomy, 78.1% reached a TICI score of 3/2b. The final infarct volume was significantly smaller, with a TICI score of 3/2b compared with less sufficient recanalization (19.60 ± 3 cm3 versus 38.1 ± 9 cm3; P < .001). After TICI 3/2b recanalization, 81% ± 5.2% of the potential infarct size (calculated as the sum of infarct core and penumbra) could be rescued. In patients with TICI scores of 2a or worse, only 39 ± 28.3 were salvaged (P < .001). The Alberta Stroke Program Early CT Score after successful recanalization TICI score of 3/2b resulted in a decline of 1.9 ± 1.4 compared with the significantly higher degradation score of 3.7 ± 1.7 after recanalization, with a TICI score of 2a or worse. A recanalization TICI score of 3/2b resulted in an NIHSS improvement of 7.3 ± 0.8 NIHSS points, whereas a poorer recanalization improved on the NIHSS by only 2.5 ± 1.5 points (P < .01).
CONCLUSIONS: Mechanical thrombectomy is a potent method to rescue large areas of penumbra in acute stroke.
ABBREVIATIONS:
- CCT
- cranial CT
- MTE
- mechanical thrombectomy
Ischemic stroke caused by the acute occlusion of an intracranial blood vessel is a serious medical emergency. It can lead to severe disability and death in approximately one-fifth of all patients,1,2 and, because of the often prolonged dependency of patients who have a stroke, the disease brings high economic costs.3 Because of its ability to measure the infarct core by the diminished CBV and the penumbra and/or oligemia among others indicated by prolonged MTT, CTP has become a very useful and reliable tool in predicting final infarct sizes.4,5 As a result, this technique is widely used to detect potentially rescuable endangered brain tissue and therefore to guide decisions about the use of recanalization therapy.6
The intravenous administration of tPA up to 4.5 hours after symptom onset can result in an overall reduction in the mortality and severe disability rate of up to 30%.7 Despite this substantial improvement in ischemic stroke treatment by the introduction of tPA, the ability of this procedure to resolve large intracranial vessel occlusions has remained poor.8⇓–10 Whereas 63% of blood clots <4 mm were resolved by tPA, only 1% of clots >8 mm were successfully dissolved by tPA.11 Additionally <10% of all patients with stroke are eligible for intravenous tPA.12
In recent years, mechanical thrombectomy (MTE) as a new treatment option has been very successful in the treatment of large-vessel occlusions. Especially with the help of a catheter-guided, second-generation, retractable stent retriever, it is possible to harbor the clot from the intracranial vessel, which leads to fast and lasting reperfusion. Some recent studies showed both the efficacy and safety of this method, reporting both significantly higher rates of recanalization and improved clinical outcomes compared with intravenous tPA alone.13⇓⇓⇓⇓⇓⇓–20
The aim of the present study was to determine the volume of infarction and amount of rescued brain tissue after MTE and to determine whether a correlation with the clinical course exists.
MATERIALS AND METHODS
The present retrospective, single-center cohort analysis was performed following the guidelines of and was approved by the local ethics committee.
The inclusion criteria are listed as follows:
Patients had an acute stroke in the anterior circulation between January 1, 2008, and May 1, 2012.
Patients were investigated with an imaging protocol including CTP before MTE.
Patients were treated with the use of MTE.
A cranial CT (CCT) at least 12 hours after MTE was available.
Exclusion criteria were:
Evidence of intracranial hemorrhage or intracranial mass, suspicious of tumor.
No sign of major artery occlusion in CTA.
Clearly visible sign of infarction in more than one-third of the corresponding vascular territory.
All patients fulfilling the above-mentioned criteria were consecutively enrolled in the present study. The CTP examination was performed by a routine stroke CT protocol including CCT, CTA, and CTP, with the following parameters: All scans were performed on a 64-section multidetector CT scanner (Philips, Best, the Netherlands). The CTP was acquired with a total of 4 scan sections and a section thickness of 10 mm. Forty milliliters of contrast agent followed by 60 mL of saline was injected during the 60-second scan. The volume of the infarct core and the penumbra were calculated automatically (IntelliSpace Portal V5, Philips; thresholds: 1.5 times increased MTT, reduced CBV: 2 mL/100 g, high permeability: 5 mL/min/100 g21).
Subsequent stent-retriever–based MTE was performed as described elsewhere.22,23 Additionally, all patients were treated with a full dose of intravenous tPA (“bridging”). At 12 hours after MTE, the CCT and CTP images were fused with the use of commercial software (iPlan Cranial 3.0, BrainLAB AG, Germany) to match the angulation between pre-MTE CTP and post-MTE CCT and to limit the assessment of the post-MTE infarct size to the slides studied previously by CTP. Infarct size in CCT at 12 hours after MTE was measured 3 times on the corresponding slides by 2 experienced, board-certified neuroradiologists working independently, and the averages were calculated and used for further analysis. Additionally, the Alberta Stroke Program Early CT Score (ASPECTS)24 was obtained on the initial CT and in the follow-up CT by the same neuroradiologists in consensus.
Clinical assessment was performed by use of the NIHSS both at admission and on the day of discharge. The quality and success of MTE was measured by the TICI score, in which a TICI score of 3 or 2b was considered a good recanalization.
Statistical Analysis
Statistical analysis was performed with the use of SPSS 20 (IBM, Armonk, New York) and SigmaPlot 11 (Systat). If not otherwise mentioned, a Kruskal-Wallis 1-way ANOVA on ranks was followed by multiple comparison procedures (Dunn method) to test for significant differences between groups. Statistical significance was assumed at P < .05. All data are presented as mean ± standard estimate of the mean, if not otherwise indicated.
RESULTS
In total, 73 patients were included in the present study. Women made up 52.1% of patients, and the mean age was 68 ± 2 years (minimum: 18; maximum: 96). The NIHSS score at admission was 13.2 ± 0.75 (Table 1). The performed CTP showed an average ischemic core of 29 ± 5 cm3 and an average penumbra or tissue-at-risk of 85 ± 6 cm3 (Fig 1A).
Patient data

A, Chart shows initial sizes of the infarct core and the penumbra in CTP. The average final infarct size after MTE (striped pattern) is smaller than the predicted infarct core. B, Good recanalization of TICI score 3/2b results in a significantly smaller infarction compared with a less sufficient recanalization.
MTE was performed subsequently, and 78.1% of all patients could be sufficiently recanalized, with a TICI score of 3 or 2b (Table 1). There was no significant difference in baseline values concerning patients with a sufficient versus insufficient recanalization concerning either the epidemiologic data or the treatment modalities such as time to treatment or time to reperfusion. Also, there was no significant difference in the ASPECTS before MTE, with a score of 8.1 ± 0.9 in patients with a recanalization result of TICI 2a or worse and 8.2 ± 1.1 in patients with TICI 3/2b. The measured infarct size after MTE in our patient group was 19.60 ± 3 cm3. The patients with a sufficient recanalization of TICI 3/2b had a significantly smaller infarct size of 14.5 ± 2.1 cm3 compared with the infarct size of 38.1 ± 9 cm3 (P < .001) after a poorer MTE result of TICI 2a or worse (Fig 1B). As an internal quality reference, the ASPECTS was assessed before and after MTE, and the difference was calculated. In analogy to our acquired infarct volumes, the difference in ASPECTS after successful recanalization TICI score of 3/2b resulted in a decline of 1.9 ± 1.4, compared with significantly higher degradation of 3.7 ± 1.7 after a less sufficient recanalization, with a resulting TICI score of 2a or worse (Fig 2A).

A, Successful recanalization resulted in a significantly lower deterioration of ASCPECTS after MTE compared with a less sufficient recanalization. B, There is a clear correlation between the amount of rescued tissue at risk identified by CTP and the final infarct growth measured by the difference in ASPECTS before and after MTE.
The sum of the infarct core and penumbra represents the potential size of the final infarction. Therefore, we were able to calculate the amount of rescued brain volume. A TICI score of 3/2b resulted in the rescue of 81% ± 5.2% of endangered brain tissue, whereas only 39% ± 28.3% could be salvaged after MTE TICI score of 2a or worse (P < .001) (Fig 3). The difference was especially dramatic in light of the group with large-tissue rescues. Furthermore, in 54.4% of the patients with a good MTE result, >90% of their potential infarction was rescued in contrast to only 6.25% of all patients with poorer MTE results (Fig 4). Again, the ASPECTS was used as an internal reference. There was a significant correlation between the difference in ASPECTS before and after MTE on the one hand and the corresponding amount of rescued brain tissue on the other. Whereas the rescue of >90% of endangered brain tissue resulted in a deterioration of ASPECTS of 1.6 ± 0.2, the ASPECTS worsened by 3.7 ± 2.4 points when <50% of endangered brain tissue could be rescued (Fig 2B) (Table 2).

MTE of TICI score 3/2b was able to rescue >80% of the endangered brain tissue at risk (evaluated by pre-MTE CTP). Less than half of that tissue could be rescued by a poor MTE.

Stacked bar chart shows the grouped percentage of rescued brain tissue. After TICI score 3/2b recanalization in >50% of all cases, >90% of the tissue at risk could be rescued, whereas that rate dropped to <10% after MTE with a TICI score of 2a or less. Additionally, the number of cases in which <50% of tissue at risk could be rescued nearly quadrupled with a poor recanalization.
Patient data after MTE
Three examples of different MTE results that led to different amounts of final infarct and rescued brain tissue are shown in Fig 5.

A, CTP indicated a large penumbra in the right MCA territory (black arrow). MTE was unsuccessful with a TICI score of 0. In the post-MTE CCT, a large infarction (larger than the initial penumbra, possibly caused by swelling effects) developed (white arrow). In the following days, a progressive herniation occurred and the patient died. B, In CTP, an infarct core in the left frontal MCA territory is detected (black dashed arrow) with a large surrounding penumbra (black arrow). After MTE TICI score of 3, the infarct core became infarcted (white dashed arrow) where the penumbra could be rescued. C, In CTP, a large area of tissue at risk in the left MCA territory without any significant infarct core can be detected (black arrow). After MTE TICI score of 3, no sign of infarction could be detected in post-MTE CCT.
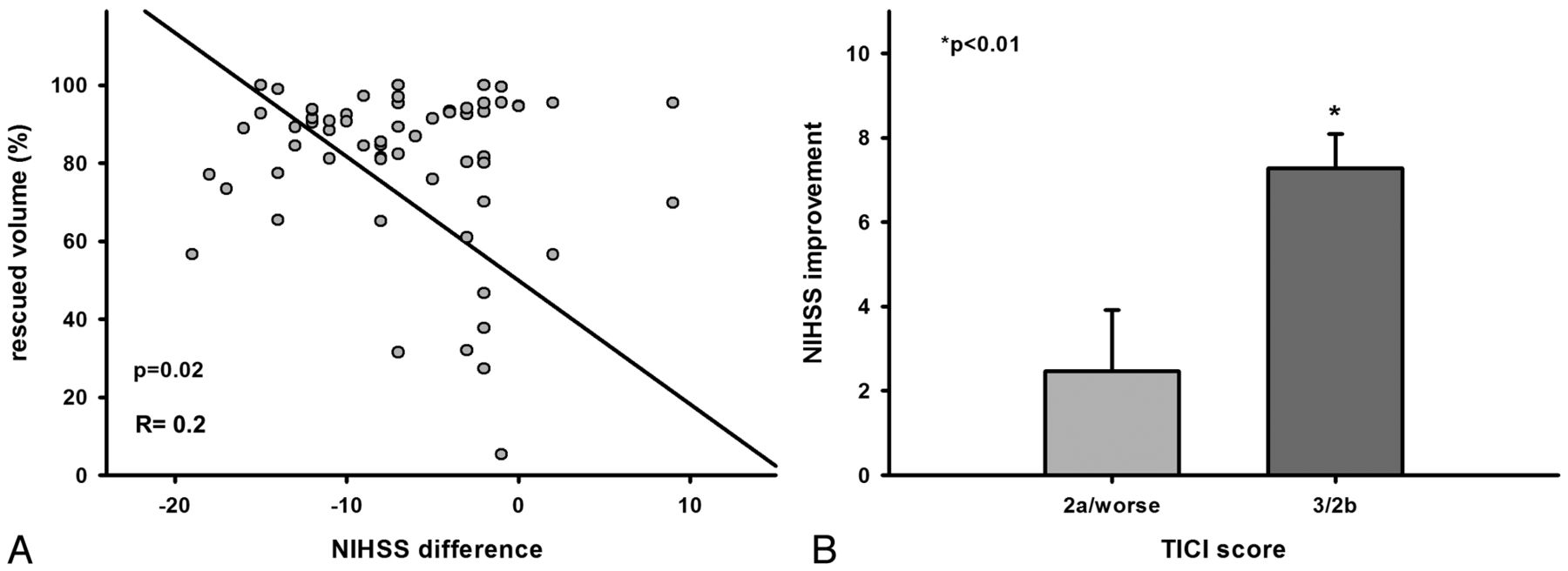
Regarding the short-term clinical outcome, there was a highly significant correlation between the percentage of rescued brain tissue and the difference in the NIHSS score between admission and discharge (P < .02) (Fig 6). The greater the amount of rescued brain tissue, the more dramatic was the clinical improvement (Fig 6A). Again, the post-MTE TICI score was highly significantly associated with short-term NIHSS development. A recanalization TICI score of 3/2b resulted in an NIHSS improvement of 7.3 ± 0.8 points, whereas a poorer recanalization improved on the NIHSS by only 2.5 ± 1.5 points (P < .01; Fig 6B) over time. Thus, the benefit of a good MTE result with consideration of the short-term NIHSS improvement was striking (global odds ratio, 1.4 for NIHSS improvement >10 points; 95% CI, 1.2–1.7).

A, There is a clear correlation between the amount of rescued brain tissue and short-term NIHSS development: the greater the amount of brain tissue that was rescued, the more dramatic the clinical improvement, as measured by the difference in NIHSS at admission and on the day of discharge. B, Again, the results of MTE predict the short-term outcome, as measured by the improvement in NIHSS.
DISCUSSION
CTP is an easy-to-use and widely available diagnostic tool for measuring and visualizing the amount of endangered brain tissue after acute occlusion of an intracranial blood vessel and the subsequent breakdown in oxygen supply and other nutrients to neurons. Since its first description,25 the concept of the penumbra has changed the view of ischemic stroke among treating physicians from a “catastrophe to be accepted” to a “treatable” disease. Generally, the penumbra is defined as a hypoperfused tissue in which the cerebral blood flow is too low to maintain neuronal electrophysiologic activity, which will lead to infarct after some time.
In the present study, we showed that the penumbra, as detected by CTP, is a potential target for rescue by endovascular mechanical recanalization. With a complete recanalization in 78.1% of our patient group, we found significantly higher recanalization rates than in the now more historical MERCI and the Multi-MERCI trials. Even compared with recently published studies such as IMS-III and MR RESCUE, we can show significantly higher recanalization rates with the use of second-generation stent retrievers compared with recanalization rates of <45% in IMS-III and 67% in MR RESCUE.26,27 Both studies used a more generous definition of the term “successful” recanalization than the definition that we used, with a definition of TIMI 3/2 in IMS-III and TICI 3–2a in MR RESCUE. Both studies would have an even smaller recanalization rate with our definition of a “successful” recanalization with a TICI score of 3/2b. These low recanalization rates may be the main reason why both studies could not show the superiority of endovascular treatment compared with intravenous tPA alone; the SWIFT study proved that there is a clearly positive correlation between successful recanalization and clinical improvement, measured by the mRS28 or the NIHSS, as we show in the present work. As a result of these trials, in our opinion, a fast and preferably complete recanalization is the main goal of every (not just endovascular) stroke therapy and is, besides the time to treatment,29 the single most important independent prognostic factor.
In our study, the final infarct size after good recanalization was significantly smaller than after poor or unsuccessful MTE. Both subgroups did not show any significant differences between age, sex, initial NIHSS score, or initial infarct size measured by the ASPECTS. Parsons et al4 showed in 2005 that without major reperfusion, the final infarct size closely matches the size initially predicted by CTP. Although this concept is still often discussed, it was successfully implemented in a recent study to select patients undergoing a new intravenous thrombolysis.30 Hence, we can postulate that the difference between the initial deterioration in CTP and the final infarct size can be attributed predominantly to the treatment effect of endovascular mechanical recanalization. Although other factors (size of the clot, location of the clot, etc) might also play a role, the fact that we found a significant difference in the amount of rescued brain tissue between different MTE results further supports the conclusion that the benefit can be attributed to the treatment. Therefore, we suggest that the large difference between final infarct size and initial CTP must be attributed to the quality of recanalization.
Considering the impressive amount of rescued brain tissue specified as possibly endangered, with a prolonged MTT in CTP, the highly significant difference between the recanalization results was striking. Although one must admit that the infarct size in early CCTs after MTE tends to be underestimated compared with that in DWI, and therefore the >80% rescue rate may be exaggerated, we performed a method less prone to examiner bias: the ASPECTS, which is known to be nearly as sensitive to ischemic changes as DWI31 when used by trained examiners. With the help of this well-established tool, we found the same highly significant correlation between recanalization result and amount of rescued brain tissue. We tried to minimize the underestimation of the infarct by having 2 people independently assess the CCTs in 3 separate rounds. Nevertheless, one of the major weaknesses of the present study is the use of CT-based techniques rather than an MRI-based protocol. Although this MRI-based patient selection and protocol to investigate the development of the infarct lesions after endovascular treatment may be more advanced, it is a setup that few centers can keep on hand. Even in our high-volume neurointerventional center, follow-up MRI after MTE has been established as a routine for approximately 2 years. Therefore, our aim was to investigate whether it was possible to achieve the same goal with a technically less demanding and especially less time-consuming method.
Besides the limitations with the use of a CT-based evaluation rather than an MRI-based approach, we must admit that the present study is designed as retrospective and did not recruit in a prospective manner. All consecutive patients matching the inclusion and exclusion criteria were enrolled, minimizing the bias of a retrospective study. Additionally, we did not recruit a control group. However, in the present work, patients with a futile or partially successful recanalization served as an internal control group.
Although there have been some indications that the use of CBF is superior to CBV in determining and predicting the final infarct size and infarct core, respectively,4 we used the MTT/CBV ratio on purpose because most commercial semi-automatic CTP evaluation tools in a clinical setup still use the ratio. Therefore, in our opinion, it was justified to use this somehow “old-fashioned” method.
Similar to recently published results,32,33 we also found a clear correlation between the volume of rescued brain tissue and short-term clinical improvement, as measured by the difference in the NIHSS. In our opinion, this finding is particularly important because both successful recanalization and minimizing the infarct size for no clinical benefit may be satisfying for the interventionalist but meaningless for the patient and the treating clinician. However, it would be useful to have a tool for early prediction of the short- to mid-term outcome. In light of our data and the above-mentioned previous studies, we propose that the evaluation of infarct size and amount of rescued brain tissue could be used as a tool to sensitively predict the clinical course over the days and possibly weeks after ischemic stroke.
CONCLUSIONS
In the present work, we found that acute ischemic stroke treatment with stent-retriever–based endovascular mechanical recanalization and subsequent fast and lasting cerebral reperfusion can result in the rescue of a large amount of endangered brain tissue with a highly significant correlation to the clinical improvement of the patients.
Footnotes
B.F. and O.K. contributed equally to this work.
Data previously presented by Dr Friedrich at: Annual Meeting of the American Society of Neuroradiology, May 21, 2013; San Diego, California and awarded with the Michael Brothers Memorial Award.
REFERENCES
- Received June 27, 2013.
- Accepted after revision August 6, 2013.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}