
Article Figures & Data
Figures
- Fig 1.
Left ICA angiogram, lateral view, depicts typical features of a capillary vascular malformation in the left frontal opercular region, with a subcentimeter vascular blush identified in the arterial (A) persisting into early venous phase (B, arrow), without evidence of arteriovenous shunting. On MR imaging, this appears as a focal region of hyperintensity on axial T2 FLAIR imaging (C, arrow), with fluffy enhancement on coronal gadolinium-enhanced T1-weighted imaging (D, arrow). No dilated arterial feeder or dilated draining vein is seen.
- Fig 2.
Lateral projection of right ICA angiogram (A–C) and axial T1-weighted gadolinium-enhanced MR imaging (D) demonstrate the typical imaging features of a capillary vascular malformation in a 17-year-old male patient with HHT. A focal subcentimeter blush (arrows) is identified on the arterial phase of a right carotid angiogram, in the frontal, temporal, and parietal regions, in keeping with multiple capillary telangiectasia. Magnified view of the right parietal lesion shows typical angiographic features, with vascular blush identified in the arterial (B) persisting into early venous phase (C); no arteriovenous shunting, dilated arterial feeder, or dilated draining vein are seen. MR imaging appearance of the right parietal lesion demonstrates the typical features of fluffy contrast enhancement in a superficial cortical/subcortical location, without abnormal vascular dilation (D, arrow).
- Fig 3.
Lateral view of a right ICA angiogram in a 43-year-old male patient with HHT demonstrates a capillary vascular malformation in the right anterior parietal region. A subcentimeter blush is seen in the arterial phase (A, arrow), which persists in the late arterial phase (B) without evidence of arteriovenous shunting.
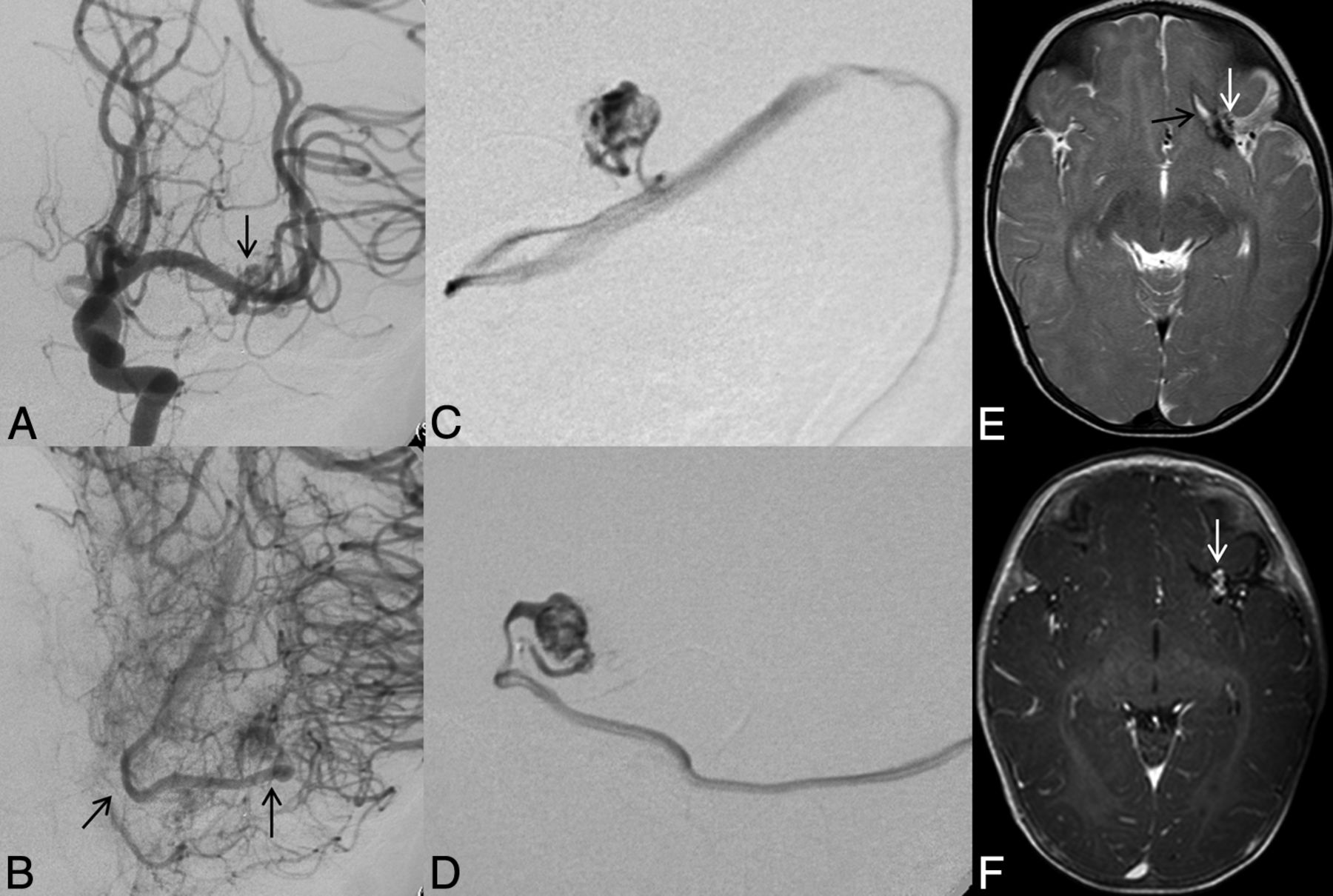
- Fig 4.
Left ICA catheter angiogram (A and B), microcatheter injection (C and D), axial T2-weighted (E), and contrast-enhanced T1-weighted MR imaging (F) demonstrate imaging findings of a typical arteriovenous malformation. Anteroposterior projection of a left ICA injection demonstrates filling of the AVM nidus through an enlarged anterior temporal branch of the left MCA in the early arterial phase (A, arrow). There is arteriovenous shunting with early venous drainage through an enlarged left inferior temporal vein (B, arrows). Microcatheter injection in frontal (C) and lateral (D) projections demonstrates a typical glomerular well-defined compact nidus supplied by a single terminal arterial feeder with shunting into a dilated vein. MR imaging shows the superficial location of the AVM, with vascular flow voids seen on T2-weighted imaging (E, arrow) and enhancement on postgadolinium T1-weighted imaging (F, arrow). Evidence of previous hemorrhage related to AVM rupture, with a slit-like hematoma cavity in the left inferior frontal lobe, and surrounding hemosiderin staining (E, black arrow).
- Fig 5.
Typical MR imaging features of an arteriovenous malformation in a 50-year-old male patient with HHT. Axial T2-weighted imaging demonstrates a cluster of flow voids in the left occipital lobe, in keeping with a vascular nidus (A). A linear flow void of the dilated draining vein is seen inferior to the nidus on axial T2 (B) and coronal postcontrast T1-weighted imaging (C). Axial MRA MIP demonstrates a compact glomerular-type nidus in the left occipital lobe (D).
- Fig 6.
Right ICA catheter angiogram in lateral (A) and frontal (B) projections demonstrates 2 separate high-flow single-hole pial arteriovenous fistulas, 1 in the right frontal lobe and 1 in the right temporal lobe. Arterial supply to each fistula is through a single enlarged right MCA branch, which empties directly into a large venous pouch. Venous drainage is superficial, with both fistulas draining through enlarged cortical veins to the superior sagittal sinus. On axial T2-weighted MR imaging (C and D) venous pouches appear as flow voids and exert mass effect on the adjacent right temporal lobe. Evidence of venous congestion with venous reflux through dilated transdmedullary veins to the deep venous system is demonstrated on a coronal reconstruction of CTA (arrows).
- Fig 7.
Lateral view of a left ICA angiogram in an 8-year-old male patient with HHT. Angiography in early arterial (A) and venous (B) phases demonstrates a high-flow single-hole pial arteriovenous fistula in the left frontal lobe. Arterial supply is through a single enlarged prefrontal branch of the left MCA, which empties directly into a large venous pouch. Venous drainage is superficial through an enlarged cortical vein to the superior sagittal sinus.







Tables
Characteristic Summarya Demographics Female sex 41/75 (55%) Age at enrollment (yr) (n = 75) 36.6 ± 19.9 Age at brain malformation diagnosis (yr) (n = 68) 30.1 ± 19.7 HHT-related symptoms Epistaxis 66/73 (90%) Anemia 20/72 (28%) GI bleeding 5/67 (7%) Pulmonary AVM 45/69 (65%) Liver VM 4/66 (6%) HHT-causing mutation ALK1 13/45 (29%) Endoglin 27/45 (60%) SMAD4 1/45 (2%) All test findings negative 4/45 (9%) Note:—GI indicates gastrointestinal; VM, vascular malformations.
↵a Summary is the No. of observations with specified value over the total No. (and the percentage) or the mean ± SD.
Characteristic Summarya Size of maximal dimension (mm) (n = 80) 4.8 ± 2.1 Lobe Frontal 30/80 (38%) Parietal 16/80 (20%) Occipital 14/80 (18%) Temporal 10/80 (13%) Cerebellum 7/80 (9%) Brain stem 2/80 (3%) Thalamus/basal ganglia 1/80 (1%) Location Deep 3/80 (4%) Subcortical 14/80 (18%) Superficial 63/80 (79%) MRI visible 66/71 (93%) ↵a Summary is the No. of observations with specified value over the total No. (and the percentage) or the mean ± SD.
Characteristic Summarya Size of maximal dimension (mm) (n = 34) 18.3 ± 5.3 Eloquent 13/34 (38%) Deep venous drainage 5/31 (16%) Spetzler-Martin score 1 16/31 (52%) 2 12/31 (39%) 3 2/31 (6%) 4 1/31 (3%) 5 0/31 (0%) Lobe Frontal 14/34 (41%) Parietal 5/34 (15%) Occipital 4/34 (12%) Temporal 5/34 (15%) Cerebellum 2/34 (6%) Brain stem 2/34 (6%) Thalamus/basal ganglia 2/34 (6%) Location Deep 4/34 (12%) Subcortical 5/34 (15%) Superficial 25/34 (74%) Nidus en passage (vs terminal) 2/20 (10%) Diffuse nidus (vs sharp) 6/34 (18%) Pial-to-pial collateralization 5/31 (16%) Moyamoya-type changes 0/33 (0%) Stenoses on arteries 0/31 (0%) Type, pial (vs choroidal) 33/34 (97%) Associated aneurysms 0/30 (0%) Multiple draining veins 3/29 (10%) Venous ectasia 8/31 (26%) Venous reflux 1/29 (3%) Pseudophlebitic pattern 0/29 (0%) ↵a Summary is the No. of observations with specified value over the total No. (and the percentage) or the mean ± SD.
Characteristic Summarya Single hole with pouch 10/11 (91%) Lobe Frontal 4/11 (36%) Parietal 0/11 (0%) Occipital 3/11 (27%) Temporal 3/11 (27%) Cerebellum 0/11 (0%) Brain stem 0/11 (0%) Thalamus/basal ganglia 1/11 (9%) Location Deep 1/11 (9%) Subcortical 0/11 (0%) Superficial 10/11 (91%) Pial-to-pial collateralization 3/11 (27%) Moyamoya-type changes 1/11 (9%) Stenoses on arteries 1/11 (9%) Type, pial (vs choroidal) 2/11 (18%) Associated aneurysms 2/11 (18%) Multiple draining veins 5/11 (45%) Venous ectasia 11/11 (100%) Venous reflux 0/11 (0%) Pseudophlebitic pattern 3/11 (27%) ↵a Summary is the No. of observations with specified value over the total No. (and the percentage).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Current Practice: Rationale for Screening Children with Hereditary Hemorrhagic Telangiectasia for Brain Vascular Malformations
- Prevalence and Characteristics of Intracranial Aneurysms in Hereditary Hemorrhagic Telangiectasia
- Endovascular treatment in the multimodality management of brain arteriovenous malformations: report of the Society of NeuroInterventional Surgery Standards and Guidelines Committee
- Comparison of MRI, MRA, and DSA for Detection of Cerebral Arteriovenous Malformations in Hereditary Hemorrhagic Telangiectasia
- A theory for polymicrogyria and brain arteriovenous malformations in HHT
- Management of Brain Arteriovenous Malformations: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association
- Natural history of brain capillary vascular malformations in hereditary hemorrhagic telangiectasia patients
- Neurovascular Manifestations of Hereditary Hemorrhagic Telangiectasia: A Consecutive Series of 376 Patients during 15 Years
- Cerebrovascular Manifestations of Hereditary Hemorrhagic Telangiectasia