
Abstract
BACKGROUND AND PURPOSE: MR imaging–detected carotid intraplaque hemorrhage indicates vulnerable plaque with high stroke risk. Angiotensin II stimulates intraplaque hemorrhage in animal models, and the angiotensin system is highly regulated by vitamin D. Our purpose was to determine whether low vitamin D levels predict carotid intraplaque hemorrhage in humans.
MATERIALS AND METHODS: In this cross-sectional study, 65 patients with carotid disease underwent carotid MR imaging and blood draw. Systemic clinical confounders and local lumen imaging markers were recorded. To determine the association of low vitamin D levels with MR imaging detected intraplaque hemorrhage, we performed multivariable Poisson regression by using generalized estimating equations to account for up to 2 carotid arteries per patient and backward elimination of confounders. MR imaging detected intraplaque hemorrhage volume was also correlated with vitamin D levels and maximum plaque thickness. Thirty-five patients underwent carotid endarterectomy, and histology-detected intraplaque hemorrhage was correlated with vitamin D levels and total plaque area.
RESULTS: Low vitamin D levels (<30 ng/mL, prevalence ratio = 2.05, P = .03) were a significant predictor of MR imaging detected intraplaque hemorrhage, along with plaque thickness (prevalence ratio = 1.40, P < .001). MR imaging detected intraplaque hemorrhage volume linearly correlated with plaque thickness (partial r = 0.45, P < .001) and low vitamin D levels (partial r = 0.26, P = .003). Additionally, histology-detected intraplaque hemorrhage area linearly correlated with plaque area (partial r = 0.46, P < .001) and low vitamin D levels (partial r = 0.22, P = .03). The association of intraplaque hemorrhage volume with low vitamin D levels was also higher with ischemic stroke.
CONCLUSIONS: Low vitamin D levels and plaque thickness predict carotid intraplaque hemorrhage and outperform lumen markers of vulnerable plaque. This research demonstrates a significant link between low vitamin D levels and carotid intraplaque hemorrhage.
ABBREVIATIONS:
- AT1R
- angiotensin II type 1 receptor
- IPH
- intraplaque hemorrhage
- NADPH
- nicotinamide adenine dinucleotide phosphate
- PR
- prevalence ratio
Large-artery atherosclerosis, including carotid disease, is a significant cause of ischemic stroke and an important therapeutic target.1 Reports estimate that carotid disease accounts for 10%–15% of ischemic strokes.2,3 Additionally, recurrent stroke is more highly associated with carotid atherosclerosis than other causes.4,5 While only 10%–15% of patients with stroke have large-artery atherosclerosis, approximately one-third of early recurrence occurs in this group.6,7
These past estimates are based on whether moderate or severe stenosis is present, defined for the carotid arteries as NASCET stenosis of >50%.8 More recent studies have questioned stenosis, finding that other markers predict unstable plaque better, including intraplaque hemorrhage (IPH). Carotid IPH is a better estimate of recurrent stroke risk, with a ∼5-fold higher risk of recurrent stroke in all stenosis categories in multiple recent studies and meta-analyses.9⇓–11 Carotid IPH can be accurately detected with heavily T1-weighted sequences, including MPRAGE. Both MPRAGE and TOF have low false-negative rates (3% versus 4%), but the MPRAGE sequence has a lower false-positive rate (20%) compared with TOF (44%).12
Despite MR imaging detection of IPH, no treatment has been shown to reverse these lesions. A potential treatment target is the angiotensin system, a major determinant of carotid plaque instability and stroke risk.13 Angiotensin II stimulates adventitial neovascularity and is implicated in animal models of IPH.14 Angiotensin II increases plaque microvessel angiogenesis through the endothelial angiotensin II type 1 receptor (AT1R).15 AT1R activation leads to reactive oxygen species formation through the nicotinamide adenine dinucleotide phosphate (NADPH) oxidase and plaque inflammation.15 Extrapolating from this, inhibition of the angiotensin system may prevent or decrease IPH.
The angiotensin system is highly regulated by an endogenous inhibitory axis, including vitamin D and the vitamin D receptor.16 The vitamin D receptor is downregulated in atherosclerotic plaque in animal models.17 Vitamin D deficiency has been associated with increased intima-media and plaque thickness in subclinical carotid atherosclerosis.18 Serum vitamin D levels are negatively correlated with carotid intima-media thickness (r = −0.51).19 Prior studies have demonstrated a high prevalence of vitamin D insufficiency (<30 ng/mL, 63.6%) and increased stroke risk in the Mountain West population of the United States.20 This mirrors the prevalence of vitamin D deficiency (<20 ng/mL) in the United States as a whole (41.6%).21
Our purpose was to determine whether low vitamin D levels predict carotid IPH in patients with carotid disease. Our hypothesis was that low vitamin D levels are associated with carotid IPH when controlling for systemic and local plaque confounders. If confirmed, this pathway may represent an important treatment target in patients with carotid IPH.
Materials and Methods
Clinical Study Design
This was a cross-sectional study of patients with carotid disease, defined as ≥2-mm-thick carotid plaque. Patients were consecutively recruited from neurovascular outpatient and inpatient services. Exclusions included patients younger than 18 years of age, prisoners, pregnancy, or those with contraindications to MR imaging (eg, pacemakers). There were no exclusion/inclusion criteria for carotid stenosis other than complete occlusion. Sixty-five patients were recruited and completed carotid MR imaging and blood draw.
Ethics.
Institutional review board approval was obtained along with informed consent from all subjects. In subjects with impaired decisional capacity, legal authorized representative consent and patient assent was obtained.
Serologic Analysis of Vitamin D and Angiotensin II
All patients underwent blood draw following IV placement for MR imaging. Samples were taken directly to the Associated Regional and University Pathologists for serum vitamin D analysis by quantitative high-performance liquid chromatography tandem mass spectrometry (25-hydroxyvitamin D2 and D3; http://ltd.aruplab.com/Tests/Pub/2002348) and plasma angiotensin II analysis by quantitative immunoassay (http://ltd.aruplab.com/Tests/Pub/0098771). Vitamin D levels were considered low/insufficient at <30 ng/mL. Angiotensin II levels were considered high at >18 ng/L.
Research MR Imaging Protocol
Images were obtained on 3T MR imaging scanners (Trio, Verio, Skyra and Prisma scanners; Siemens, Erlangen, Germany) with custom-made carotid coils.22 Each MR imaging included brain DWI and carotid MPRAGE sequences acquired with custom neck coils described below.
Subject-Specific Radiofrequency Coils
A modular system of subject-specific radiofrequency coil arrays was used to maximize signal to noise.23 The head coil provides head immobilization, essential to carotid imaging.24 Either 7-channel or 9-channel coils were used, connected to preamplifiers through low-resistance connectors, allowing them to be interchanged to fit necks of different shapes and sizes. These coils can image simultaneously with clinical head coils without extra positioning hardware.
Carotid MPRAGE and IPH Determination
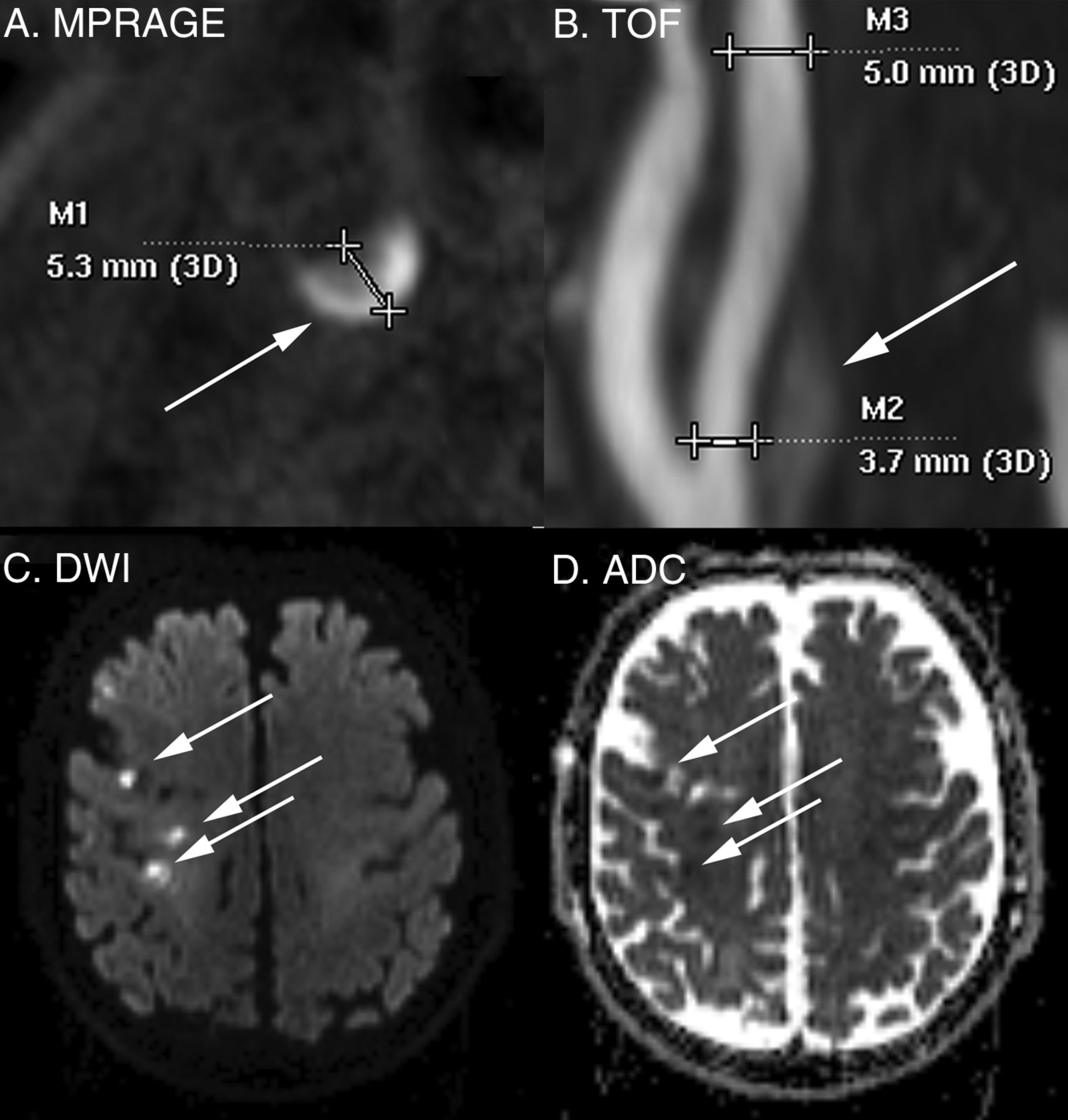
MPRAGE parameters were the following: 3D, TR/TE/TI = 6.39/2.37/370 ms, flip angle = 15°, FOV = 130 × 130 × 48 mm3, matrix = 256 × 256 × 48, voxel = 0.5 × 0.5 × 1.0 mm3, fat saturation, acquisition time = ∼5 minutes as described previously.25 Images were obtained from 20 mm below to 20 mm above the carotid bifurcation at a 1.0-mm section thickness. Carotid IPH was defined by MPRAGE-positive plaque with ≥2-fold signal compared with the sternocleidomastoid muscle (Fig 1).26 We have previously shown that MPRAGE-positive plaque corresponds to carotid IPH on histology.26 IPH volume was determined quantitatively with volumes traced from the PACS.

Carotid and brain MR imaging. Carotid IPH and maximum plaque thickness were detected by using the MPRAGE sequence as shown in this representative image with right-sided carotid IPH (A). 3D TOF MRA was used alongside duplex sonography in all patients to determine lumen findings, as in this subject with 26% stenosis by NASCET criteria (B). Stroke was determined by using the American Heart Association criteria supplemented with DWI, as in this example with recent right MCA distribution infarcts (C and D).
Carotid Lumen Measurements
All non-IPH carotid lumen measurements were determined by consensus of 2 reviewers, blinded to brain MR imaging and clinical covariates. The entire carotid plaque was considered 1 unit, from 20 mm above to 20 mm below the bifurcation. Maximum plaque thickness was measured in the transverse plane on MPRAGE images, perpendicular to the center axis of the lumen (Fig 1). Lumen markers (stenosis, ulceration, and intraluminal thrombus) were determined from noncontrast TOF with parameters as follows: 3D, TR/TE = 25/4.02 ms, flip angle = 20°, FOV = 160 × 160 × 90 mm, matrix = 256 × 256, section thickness = 0.64 mm, 144 sections, acquisition time = ∼3.5 minutes. In all cases, duplex sonography was performed before study entry and was used as a complementary measure of stenosis. In cases of >70% stenosis by either TOF or sonography or when stenosis measurements disagreed, lumen stenosis was confirmed by using contrast CTA or MRA. The percent diameter stenosis was determined with NASCET criteria, with a submillimeter measurement tool and [(a − b)/a] × 100%, where b is the diameter of maximal stenosis and a is the diameter of the ICA distal to the stenosis (Fig 1).27⇓–29 Multivariable regression was performed by using both NASCET and millimeter stenosis (b), first described on CTA.30 No near-occlusions were found in this dataset, as defined by visible bulb stenosis, a distal ICA diameter of ≤3 mm, and a distal ICA/distal external carotid artery ratio of ≤1.25.29,30 Ulceration was determined by using a size threshold of 2 mm.31 Intraluminal thrombus was determined by a filling defect and confirmed in all cases with contrast CTA or MRA.32
Ischemic Stroke Determination
Ischemic stroke was determined by using the American Heart Association definition of CNS infarction: brain or retinal cell death attributable to ischemia based on the following: 1) imaging evidence of cerebral or retinal ischemia in the carotid distribution, or 2) clinical symptoms persisting for ≥24 hours, with other etiologies excluded.33 We reviewed neurovascular clinic or inpatient charts to determine the presence of recent stroke occurring at the time of recruitment. Asymptomatic (“silent”) recent infarcts were included as strokes and determined on brain DWI performed in all patients to supplement clinical determination of infarct by showing acuity and distribution (Fig 1). DWI-positive carotid territory infarcts were detected using DTI trace images, which are superior to conventional DWI in detecting recent infarcts.34,35 The DTI parameters were 2D, 128 × 128 matrix, 3-mm section thickness, b=2000, 20 directions. Brain DWI was interpreted by a Certificate of Added qualification–certified neuroradiologist.
Clinical Characteristics
Clinical characteristics were determined by chart review, including cerebrovascular risk factors of age, male sex, diabetes, hypertension, hyperlipidemia, renal insufficiency, body mass index, and smoking status. We recorded the following cerebrovascular medications: antiplatelets, anticoagulants, statins, and antihypertensives, including antiangiotensin medications: angiotensin-converting enzyme inhibitors and angiotensin receptor blockers.
Histologic Processing
In 35 patients who underwent carotid endarterectomy, each specimen was fixed in 10% neutral buffered formalin for histology. The ratio of the fixative to the specimen was at least 10:1. Specimens were decalcified in 1% Enhanced Decalcification Formulation (SL85–32; Statlab, Lewisville, Texas). Tissue cassettes were processed on an automated Vacuum Infiltrating Processor (Sakura, Alphen aan den Rijn, the Netherlands), embedded in paraffin wax, sectioned at 3- to 4-mm intervals, and stained with hematoxylin-eosin.
Histology Interpretation of IPH
A pathologist outlined recent IPH by using hematoxylin-eosin, blinded to MPRAGE results. “Recent” IPH was defined by intact red blood cells or degenerated red blood cells on hematoxylin-eosin. Each carotid area positive for IPH was then compared with vitamin D levels.
Statistical Analysis
Statistical modeling was performed by using generalized estimating equations to account for data clustering, with up to 2 carotid arteries per patient. Carotid arteries were treated as separate units grouped within subjects because IPH may be associated with local carotid plaque markers (eg, plaque thickness) and systemic clinical factors (eg, age). Because >1 marker for IPH was being studied, potential confounding was investigated on the outcome variable, IPH. Therefore only 1 data table was required with P values from univariable generalized estimating equation Poisson regression models. Poisson regression directly estimates the prevalence ratio (PR), which is more intuitive to interpret than an odds ratio from a logistic regression approach (Zou and Donner36). Next, all potential confounders with P < .20 from a univariable model were placed in an initial multivariable generalized estimating equation Poisson regression model for IPH, then eliminated in a backward fashion until all remaining variables met the threshold P < .10. A liberal significance criterion, P < .10, was used to protect against residual confounding (Maldonado and Greenland37).
For hypothesis testing of markers predictive of IPH, we used the traditional P < .05. In binary outcome models, 5 outcome events for every predictor variable are sufficient to avoid overfitting.38 With 48 carotid plaques positive for IPH and 80 negative for IPH, 48/5 or 9.6 or up to 9 predictor variables could be included in the model without overfitting, exceeding the number of variables in our final model. Additionally, we identified the following potential confounders with a scientific basis for confounding the association between vitamin D and IPH: angiotensin, angiotensin-converting enzyme inhibitor use, and angiotensin receptor blocker use. Because of the high potential for these to confound the vitamin D and IPH association, we used a combination of the 10% change in estimate and backward elimination and kept these potential confounders in a secondary analysis even though they were eliminated in the primary analysis. We also calculated IPH volume as a continuous variable and used a linear mixed-effects regression model to correlate carotid IPH with maximum plaque thickness and vitamin D levels, again accounting for up to 2 carotid arteries per patient. For the histology-outlined IPH area correlation with vitamin D levels, a random intercept linear regression model was used with an autoregressive correlation structure repeated-measures analysis of the 35 subjects that had underwent carotid endarterectomy. In this analysis, the “time” repetition variable was each histology slide, and the “group” variable was each carotid plaque. All statistical analyses were performed with STATA 13.1 (StataCorp, College Station, Texas).
Results
Clinical Characteristics
Sixty-five patients were recruited, with a mean age 72.3 ± 8.3 years, 90.8% men and 3.1% minorities. Patients had multiple cerebrovascular risk factors (69.2% current or prior smokers, 87.7% hypertensive, 84.6% hyperlipidemic, 44.6% diabetic) and were aggressively managed before enrollment (84.6% on antihypertensives, 89.2% on statins, 81.5% on antiplatelets) (On-line Table). These characteristics reflect the high prevalence of carotid disease in our population.
Imaging and Clinical Characteristics by Vessel
Imaging and clinical characteristics were also listed by vessel and broken down by IPH status (positive versus negative) in the On-line Table. Each patient contributed 2 carotid plaques, with the exception of 2 carotid occlusions that were excluded, leaving 128 carotid arteries for the final sample. Stenosis was worse in carotid arteries with IPH-positive versus negative plaque (NASCET stenosis of 53.9% versus 35.7% and millimeter stenosis of 2.25 versus 3.17 mm, P = .003). Maximum plaque thickness was also higher (5.53 versus 4.08 mm, P < .001), and there was a higher prevalence of ulceration (64.6% versus 37.5%, P = .02) and intraluminal thrombus, though rare (6.3% versus 0.0%, P = .05). Some factors were potential confounders between IPH-positive and negative status (P < .20), requiring multivariable regression to determine essential IPH predictors.
Multivariable Generalized Estimating Equation Poisson Regression Analysis for Carotid IPH Prediction
Multivariable generalized estimating equation Poisson regression analysis was performed to determine predictors of carotid IPH from the On-line Table. The initial model included 9 predictors with P < .20: NASCET stenosis, millimeter stenosis, maximum plaque thickness, ulceration, intraluminal thrombus, high angiotensin II (>18 ng/L), vitamin D level ng/mL (continuous variable), low vitamin D level (<30 ng/mL), and male sex. Table 1 shows the final model after sequential backward elimination of confounders with P > .10. The final model included maximum plaque thickness (PR= 1.40; 95% CI, 1.18–1.67; P < .001) and low vitamin D levels (PR = 2.05; 95% CI, 1.06–3.96; P = .03) as significant predictors of carotid IPH. Table 2 illustrates the lack of confounding by angiotensin II, angiotensin-converting enzyme inhibitor, and angiotensin receptor blockers use.
Final MRI-IPH prediction modela
IPH prediction model with angiotensin system confoundersa
Linear Mixed-Effects Regression Model of IPH Volume with Maximum Plaque Thickness and Low Vitamin D Levels
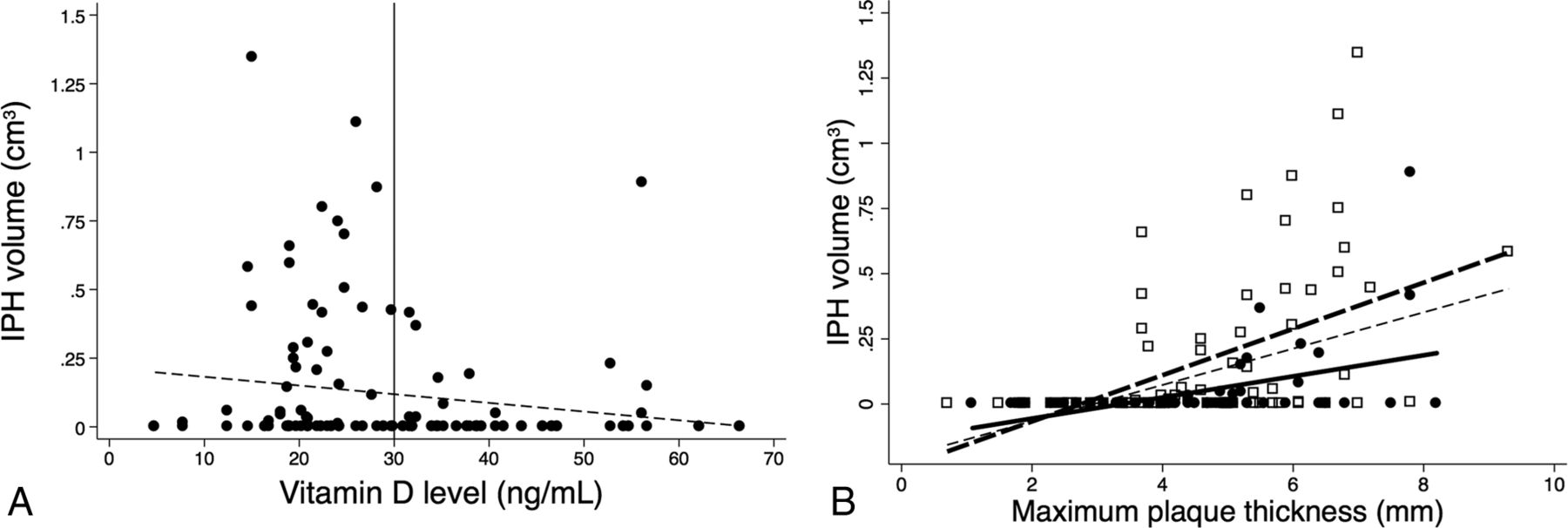
Carotid IPH volume significantly correlated with maximum plaque thickness (r = 0.45, P < .001) and low vitamin D levels (r = 0.26, P = .003) as depicted in the linear regression plot (Fig 2).

Linear regression of MR imaging–detected IPH volume, plaque thickness, and vitamin D status. Pooled data demonstrate the IPH volume negative correlation with vitamin D level (A) and correlation with maximal plaque thickness (partial r = 0.45, P < .001, thin dashed line) and low-versus-normal vitamin D levels (partial r = 0.26, P = .003; low vitamin D level: empty squares and thick dashed line; normal vitamin D levels: solid circles and thick solid line, B).
Carotid IPH Histology and Vitamin D Levels
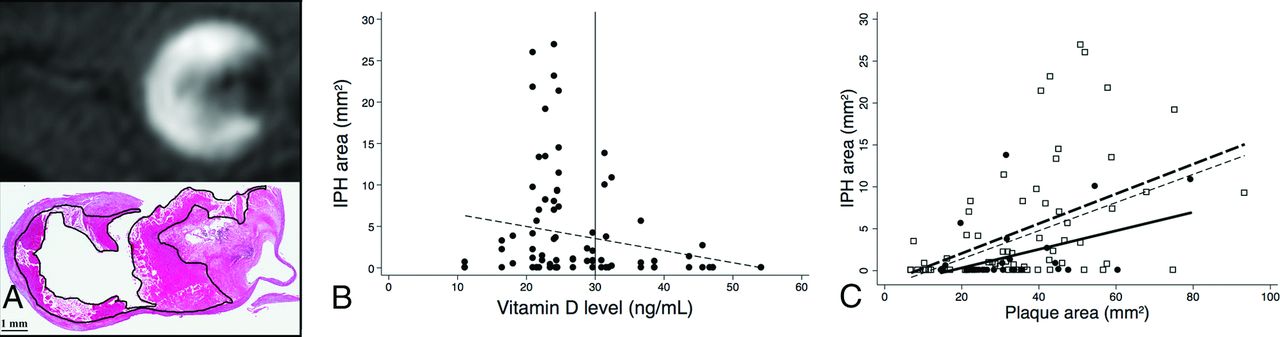
Histology-defined IPH area (Fig 3A) negatively correlated with vitamin D levels (Fig 3B). In addition, IPH area correlated with plaque area (partial r = 0.46, P < .001) and low-versus-normal vitamin D levels (partial r = 0.22, P = .03) (Fig 3C).

Linear regression of IPH area on histology, plaque area, and vitamin D status. Representative MPRAGE-positive plaque (upper image) and IPH area outlined on the corresponding hematoxylin-eosin stain (lower image) (A). Pooled data demonstrate the IPH area negatively correlating with vitamin D levels (B) and positively correlating with plaque area (partial r = 0.46, P < .001, thin dashed line) and low-versus-normal vitamin D levels (partial r = 0.22, P = .03, low vitamin D level: empty squares and thick dashed line; normal vitamin D level: solid circles and thick solid line) (C).
Carotid IPH, Vitamin D Levels, and Stroke
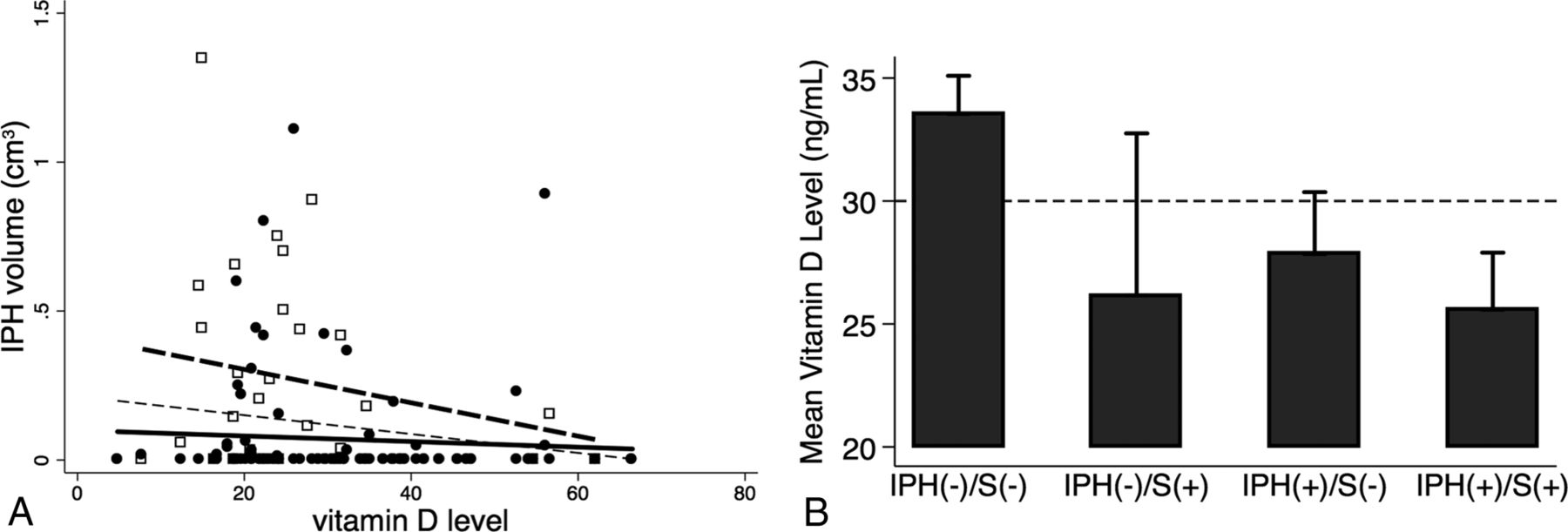
IPH volume more negatively correlated with vitamin D levels with ischemic stroke (hollow squares, thick dashed line, partial r = −0.21, P = .27) compared to without it (solid circles, thick solid line, partial r = −0.06, P = .53) (Fig 4A). Vitamin D levels were also lower in patients with versus without stroke in the setting of IPH-negative plaque (mean, 33.5 ± 13.2 ng/mL in 73 carotids versus 26.2 ± 17.4 ng/mL in 7 carotids, P = .17) and less so with IPH-positive plaque (27.8 ± 12.6 ng/mL in 25 carotids versus 25.6 ± 11.1 ng/mL in 23 carotids, P = .51) (Fig 4B).

Association of IPH volume, vitamin D levels, and ischemic stroke. IPH volume was negatively correlated with vitamin D levels as in Fig 2A (thin dashed line). When stratified by ischemic stroke status, IPH volume was more negatively correlated with vitamin D levels (hollow squares, thick dashed line, partial r = −0.21, P = .27) in ischemic stroke compared to without it (solid circles, thick solid line, partial r = −0.06, P = .53) (A). Vitamin D levels were also lower in groups positive-versus-negative for stroke in the setting of IPH-negative plaque (mean, 33.5 ± 13.2 ng/mL in 73 carotids versus 26.2 ± 17.4 ng/mL in 7 carotids, P = .17) and less so in the setting of IPH-positive plaque (27.8 ± 12.6 ng/mL in 25 carotid arteries versus 25.6 ± 11.1 ng/mL in 23 carotid arteries, P = .51) (B). S indicates carotid territory ischemic stroke status (positive or negative).
Carotid IPH Volume Follow-Up
Two patients were re-evaluated after 1 year (Fig 5). Both were treated with medical therapy (statins, antiplatelets, and antihypertensives) and both patients' primary care physicians were alerted to low vitamin D levels (<30 ng/mL). Patient 1 was supplemented, vitamin D increased (baseline/1 year: 18.1/26.8 ng/mL), carotid IPH volume decreased by 24.1% (baseline/1 year: 0.151/0.115 cm3), and he remained asymptomatic. Patient 2 was not supplemented, vitamin D levels decreased (baseline/1 year: 20.9/10.7 ng/mL), carotid IPH volume minimally decreased by 4.3% (baseline/1 year: 1.041/0.996 cm3), and he had sequential bilateral strokes.

Vitamin D supplementation and follow-up. A, Patient 1: Baseline (upper arrow) versus 1-year follow-up (lower arrow) with vitamin D supplementation and medical therapy, including statins and antiplatelet and antihypertensive medications, demonstrates decreased IPH volume in a patient with no interval stroke (vitamin D baseline/1 year: 18.1/26.8 ng/mL; carotid IPH baseline/1 year: 0.151/0.115 cm3, or 24.1% decreased IPH volume). The patient remained asymptomatic in the year between the 2 scans. B, Patient 2: Baseline (upper arrow) versus 1-year follow-up (lower arrow) without vitamin D supplementation but with medical therapy, including statins and antiplatelet and antihypertensive medications, demonstrates minimally changed IPH volume (vitamin D baseline/1 year: 20.9/10.7 ng/mL; carotid IPH baseline/1 year: 1.041/0.996 cm3, or 4.3% decreased IPH volume). In addition, this patient had bilateral strokes in the year between the 2 scans.
Discussion
This work shows that both the presence and volume of carotid IPH are strongly associated with plaque thickness and low vitamin D levels, and not necessarily with percentage stenosis or other measures of carotid architecture. This finding supports the idea that low vitamin D levels may play a role in atherosclerosis and stroke risk. Considering its multiple health benefits, vitamin D testing may be worthwhile in patients with vulnerable carotid plaque.
Low vitamin D levels have been linked to cardiovascular disease in many prior studies.39 Two cohort studies evaluating participants in the Framingham Heart Study (Offspring Cohort) and the Copenhagen City Heart Study found increased risk of ischemic stroke with lower vitamin D levels,40,41 and a low vitamin D level is an independent predictor of ischemic stroke volume.42 Most important, vitamin D supplementation decreases muscle atrophy, falls, hip fractures, and cognitive impairment and leads to functional improvement in patients with stroke.43,44 Vitamin D also has many direct beneficial effects on the vasculature. Within 1 minute of treatment, vitamin D increases endothelial cell nitric oxide production.45 Active vitamin D also improves endothelial function by decreasing AT1R and NADPH oxidase expression and increasing superoxide dismutase expression.46
An intriguing possibility is that low vitamin D levels may allow disinhibition of the local angiotensin system, leading to microvessel leakage of blood products. Alternatively, vitamin D may have an effect on the lipid-rich necrotic core where microhemorrhages occur. Most interesting, while statins have been shown to decrease the carotid lipid-rich necrotic core47 and decrease plaque inflammation,48 statins do not ensure plaque stabilization. In trials in patients with IPH, including those with symptomatic low-grade (<50%) carotid stenosis, there is an extremely high stroke recurrence rate (46.0% per patient-year), despite aggressive therapy with statins, aspirin, and antihypertensives.49 Most interesting, supplementing with vitamin D allows most statin-intolerant patients to tolerate statins and reach current low-density lipoprotein targets.50 This finding suggests an interaction between statins and vitamin D, and optimizing both may be important in treating patients with carotid IPH.
One limitation of our study is its cross-sectional nature, making it difficult to determine causation between low vitamin D levels and carotid IPH. Another limitation is that unknown confounders may exist that we did not have data to control for in the regression analysis. These would include variables related to both predictor (vitamin D) and outcome (IPH). While we evaluated multiple factors that may influence both vitamin D levels and carotid IPH, including age, sex, body mass index, angiotensin system markers, and carotid markers including plaque thickness, we did not find a significant association between IPH and any of the factors listed except for plaque thickness. Still, it is possible that low vitamin D levels are linked to some other undiscovered confounder or sedentary lifestyle, which even surveys may fail to appropriately quantify.51 Finally, our study recruited patients from the neurovascular clinic and inpatient settings who were predominantly overweight (average body mass index = 28.6), white (97%), and men (91%) and should be applied primarily to that population. Still, low vitamin D levels are highly prevalent in African American and Hispanic populations, and given the higher rates of stroke and heart attack in these groups, further study in such minorities would be worthwhile.
Despite these limitations, in patients with carotid IPH, vitamin D screening and supplementation may be warranted. A trial of vitamin D supplementation in patients with carotid disease with low vitamin D levels could clarify whether vitamin D reduces or prevents IPH. Randomized controlled clinical trials may be warranted to determine the effect of vitamin D on preventing or reversing carotid IPH and its influence on future stroke risk. The relationship between vitamin D levels and IPH could be further investigated in animal models, including the apolipoprotein E knockout mouse model of atherogenesis coupled with vitamin D deficiency or vitamin D receptor knockout models.
Conclusions
Vitamin D insufficiency was associated with both the presence and volume of carotid IPH in patients with carotid atherosclerosis. These results link low vitamin D levels with plaque vulnerability. Future clinical trials are needed to determine whether vitamin D supplementation can decrease IPH and subsequent stroke risk. Animal studies may also allow further insight into the role of vitamin D and receptor status in pathways leading to IPH.
Footnotes
Disclosures: Statistical analysis for this study was supported by the Study Design and Biostatistics Center grant* with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, grant 8UL1TR000105. J. Scott McNally—RELATED: Grants: Radiological Society of North America Research Scholar Grant* and University of Utah Intramural Seed Grant. Tina M. Burton—OTHER RELATIONSHIPS: Vascular Neurology Fellow at the National Institutes of Health/National Institute of Neurological Disorders and Stroke, from July 1, 2015, to present. Work related to this submission was performed prior to July 1, 2015. Jennifer J. Majersik—UNRELATED: Grants/Grants Pending: National Institutes of Health/National Institute of Neurological Disorders and Stroke. Dylan V. Miller—UNRELATED: Royalties: Elsevier Publishing; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: College of American Pathologists, United States and Canadian Academy of Pathology. *Money paid to the institution.
This work was supported by a Radiological Society of North America Research Scholar Grant; a University of Utah Intramural Seed Grant; and a grant for the Study Design and Biostatistics Center, with funding, in part, from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, grant 8UL1TR000105 (formerly UL1RR025764).
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology and the Foundation of the ASNR Symposium, April 25–30, 2015; Chicago, Illinois.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received November 6, 2015.
- Accepted after revision April 26, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}