
Abstract
BACKGROUND AND PURPOSE: Coiling of complex aneurysms is still difficult even with current adjuvant techniques. This study sought to evaluate the safety and effectiveness of a combination of multicatheter plus stent or balloon for the treatment of complex aneurysms.
MATERIALS AND METHODS: All complex aneurysms that underwent coiling with the combination technique were identified from prospectively maintained neurointerventional data bases. “Complex aneurysm” was defined as a wide-neck aneurysm with branch incorporation into or a deep lobulation of the sac. The clinical and angiographic outcomes were retrospectively analyzed.
RESULTS: Sixty-two complex aneurysms (12 ruptured, 50 unruptured) in 62 patients (mean age, 57 years; male/female ratio, 12:50) were treated with a combination technique by using a multicatheter plus stent (n = 42, 3 ruptured) or balloon (n = 20, 9 ruptured). Treatment-related morbidity (grade 3 hemiparesis) occurred in 1 patient (1.6%). Except for 1 patient who had treatment-related morbidity, none of the other patients with unruptured aneurysms developed new neurologic symptoms at discharge. Nine of the 12 patients with ruptured aneurysms had good outcomes (Glasgow Outcome Score, 4 or 5) at the latest follow-up (mean, 32 months; range, 6–72 months), and 1 patient died from an initial SAH. Posttreatment control angiograms revealed complete occlusion in 27, neck remnant in 34, and incomplete occlusion in 1 aneurysm. At least 1 follow-up catheter or MR angiogram was available in 80.6% (n = 50) (mean, 21 months; range, 6–65 months). There were 4 minor and 3 major recurrences (14.0%).
CONCLUSIONS: In this case series, the combination technique by using multicatheter plus stent or balloon seemed safe and effective for the treatment of complex aneurysms.
Technical advances with devices such as catheters, balloons, and stents have widened the indications and improved the outcomes of coiling for the treatment of intracranial aneurysms. A wide-neck, branch incorporation into the sac and a lobulated sac are well-known anatomic features of aneurysms that make the conventional coiling procedure difficult. These complicated anatomic features increase the risk of incomplete coiling, complications such as compromise of the parent vessel or branching artery, and posttreatment recurrence. Some case series have already reported the feasibility of adjunctive techniques for aneurysms with difficult anatomic characteristics and have presented good procedural outcomes.1⇓⇓⇓⇓–6 However, the coiling procedure of an aneurysm with a wide neck plus an incorporated branch and/or lobulated sac still remains a technical challenge.6,7 In this regard, those aneurysms should be defined as “complex aneurysms.” On the other hand, a simple combination of already well-known techniques can make it easy to coil such complex aneurysms. To our knowledge, however, the feasibility and clinical and angiographic outcomes of combination techniques for these complex aneurysms have not yet been demonstrated. In this study, we evaluated the safety and effectiveness of a combination technique such as multicatheter plus stent or balloon for complex aneurysms.
Materials and Methods
All complex aneurysms that underwent coiling with the combination technique were identified from prospectively maintained neurointerventional data bases in 2 academic tertiary referral hospitals between July 2007 and June 2014. A “complex aneurysm” was defined as a wide-neck aneurysm with an incorporated branch into and/or a deep lobulation (more than one-third of the aneurysm height) of the sac; “wide neck” meant that the neck diameter was ≥4 mm or the dome-to-neck ratio was ≤1.5. During the study period of 7 years, 1307 patients with 1423 aneurysms were treated with coiling in the 2 hospitals. One hundred twenty-one (8.5%) of the 1423 aneurysms met the definition of complex aneurysms in this study. Patient informed consent was obtained before treatment. The institutional review board approved this retrospective study with a waiver of informed consent for study inclusion. All relevant clinical and imaging data were obtained from electronic medical charts, PACSs, and a prospectively registered neurointerventional data base. The clinical and angiographic outcomes were retrospectively analyzed.
Coiling with the Combination Technique
All patients with unruptured aneurysms who were scheduled for stent-assisted coil embolization received premedication with dual antiplatelet medication (aspirin, 100 mg, and clopidogrel, 75 mg) for at least 5 days. Dual antiplatelet medication was maintained for at least 3 months and then was changed to aspirin monotherapy. For patients with ruptured aneurysms who underwent stent placement, a bolus of dual antiplatelet medication (aspirin, 100–500 mg, and clopidogrel, 300 mg) was given just after completion of the procedure. After the introduction of a guiding catheter, a bolus of heparin, 3000 IU, was injected and then heparin, 1000 IU, was given as a booster every hour. For anterior circulation complex aneurysms, a 6F Shuttle guide sheath (Cook, Bloomington, Indiana) was placed in the relevant internal carotid artery. For posterior circulation complex aneurysms, a single 6F Shuttle sheath was placed in the dominant vertebral artery or 2 Envoy guiding catheters of 5F or 6F diameter (Codman & Shurtleff, Raynham, Massachusetts) were placed in the bilateral vertebral arteries.
The combination technique was initially used in 21 complex aneurysms, and in the remaining 41 complex aneurysms, it was performed in the same session after failure of 1 of the following: the multicatheter, balloon-assisted, or stent-assisted technique. Therefore, approximately 51% (62/121) of the complex aneurysms were treated with this combined technique during the study period. For ruptured aneurysms, the balloon was preferentially chosen as an adjunctive device. Preshaped or steam-shaped 0.010-inch Excelsior microcatheters (Stryker, Kalamazoo, Michigan) were used for aneurysm selection and coil delivery with a 0.014-inch microguidewire (Traxcess; MicroVention, Tustin, California; or Synchro; Boston Scientific, Natick, Massachusetts). The adjunctive balloons in this study were HyperForm/HyperGlide (Covidien, Irvine, California) and Scepter C balloons (MicroVention). The stents used in this study included Enterprise (Codman & Shurtleff) and Neuroform (Stryker) stents.
Outcome Measures
“Treatment-related morbidity” was defined as the development of any new neurologic deficit due to treatment-related complications that were still present at discharge. “Treatment-related mortality” was defined when the patient died from treatment-related complications during clinical follow-up. The clinical outcomes of the patients with subarachnoid hemorrhage were evaluated by the Glasgow Outcome Score. A good outcome was defined as a Glasgow Outcome Score of 4 or 5. The clinical outcome at the latest follow-up was defined as the final outcome. If the latest clinical follow-up was >3 months at the point of the analysis of this study, a telephone interview was obtained to determine the patient's clinical status.
Immediate postcoiling angiographic outcome was analyzed according to the Raymond scale. Follow-up angiographic outcome was classified into 3 categories: improved/stable, minor recurrence when the recurred aneurysm did not require retreatment, and major recurrence when the recurred aneurysm required retreatment. The need for retreatment was determined on the basis of a discussion among 2 neurointerventionists and 3 vascular neurosurgeons in a weekly neurovascular conference.
Results
The Table summarizes the characteristics of complex aneurysms and the results of the combination technique by using the multicatheter plus stent or balloon.
Summary of complex aneurysms and the results of the combination technique using multicatheter plus stent or balloon
Sixty-two complex aneurysms (12 ruptured and 50 unruptured) in 62 patients (mean age, 57; male/female ratio = 12:50) were treated with a combination technique either multicatheter plus stent (n = 42, 3 ruptured) or balloon (n = 20, 9 ruptured). Treatment-related morbidity occurred in 1 patient (1.6%) who had a grade 3 right hemiparesis due to an embolic occlusion of the incorporated left anterior choroidal artery, but there was no treatment-related mortality. Except for that patient, no other patient with an unruptured aneurysm developed a new neurologic symptom. Nine of the 12 patients with ruptured aneurysms exhibited good outcomes (Glasgow Outcome Score of 4 or 5) at the last follow-up (mean, 32 months; range, 6–72 months), and 1 patient died as a consequence of the initial subarachnoid hemorrhage. Posttreatment control angiograms showed complete occlusion in 27, neck remnants in 34, and incomplete occlusion in 1 aneurysm. At least 1 follow-up angiogram was available in 80.6% (n = 50; mean, 21 months; range, 6–65 months). Seven (14%) of the 50 patients were followed by MR angiography alone. Recurrence occurred in 7 aneurysms (14.0%), including 4 minor and 3 major recurrences.
Discussion
Endovascular coiling has been increasingly used for wide-neck aneurysms due to rapid advances in devices and techniques.1⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–12 However, if wide-neck aneurysms have an incorporated branch and/or deeply lobulated sac, coiling is more difficult and there is potentially an increased risk of incomplete coiling, a thromboembolic event, or branching occlusion and posttreatment recurrence. The unique configuration of this aneurysm usually demands a more elaborate coiling technique and can be recognized as a complex and difficult aneurysm in view of the coiling procedure.
To some extent, the multicatheter technique can handle the wide-neck aneurysm via interleaving 2 or 3 coils or locking the first or second coil to make a stabilizing coil basket, and it is useful for accessing the lobulated sac by separating the catheter positions.5,6,8,13 In a recent case series, treatment-related morbidity and mortality with a dual-microcatheter technique were 1% and 2%, respectively.5 This technique can also intentionally protect the incorporated branch by placing 1 catheter or coil into the branch.6,11,12,14 Although balloons and stents were originally designed for preventing coil prolapse and enhancing coil-packing attenuation, slight overinflation of a compliant balloon or “gator backing” of open cell stent struts can additionally protect the branch incorporated with the parent artery of a wide-neck aneurysm.6,7,15
A combination technique is intended to provide the advantages of both the multicatheter technique and a stent or balloon technique. In the combination technique, a balloon or stent is used to protect the aneurysm neck, and multicatheters are used to form and stabilize the coil basket to preserve the incorporated branch (Fig 1) and/or to uniformly pack the lobulated sac with coils (Fig 2).16 This approach may be a relatively complex procedure, even though it uses already known devices. There may also be complications associated with additional instruments, such as an increase in thromboembolic events and device-related problems. For these reasons, in this study, treatment via the combination technique was initially planned in only one-third of the complex aneurysms, while in two-thirds of the aneurysms, a conventional multicatheter, balloon-, or stent-assisted technique was initially attempted. For the complex aneurysms initially treated with the combination technique, it was anticipated that the multicatheter, balloon, or stent alone could not achieve preservation of an incorporated branch or stability of the coil basket due to a wide neck with incorporated branches and/or deep lobulation (Fig 3).

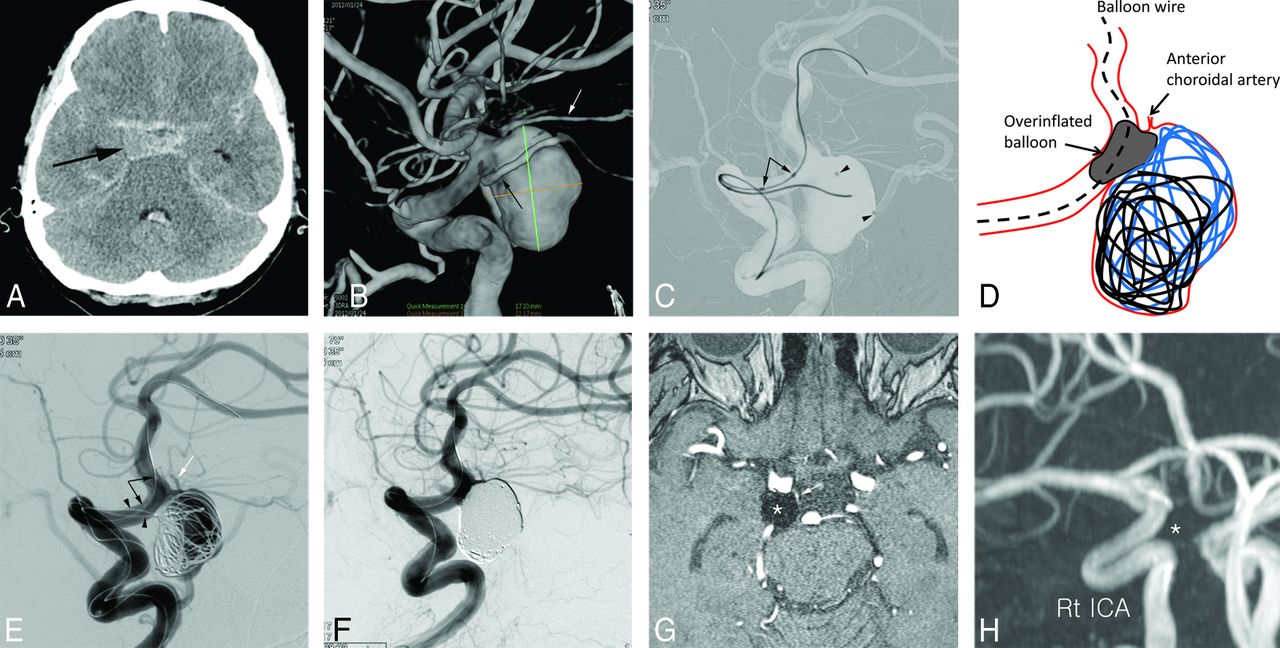
A 58-year-old man presenting with Hunt and Hess grade 3 subarachnoid hemorrhage. A, Unenhanced CT shows diffuse subarachnoid hemorrhage in the basal cistern. The arrow indicates the ruptured aneurysm. B, The 3D reconstruction image shows a 17-mm posterior communicating artery (black arrow) aneurysm with incorporation of the anterior choroidal artery (white arrow). C, A spot image shows HyperForm balloon (arrow) navigation after positioning 2 microcatheters (arrowheads) in the aneurysm sac. D, An illustration explains the technique for treating this aneurysm. During the protection of the anterior choroidal artery by an overinflated balloon, a stable coil frame basket is made by interleaving 2 coils. E, Angiogram after balloon deflation confirms a stable coil basket without compromising the origin of the incorporated anterior choroidal artery (white arrow). Arrowheads indicate 2 microcatheters for coil delivery, and black arrows indicate proximal and distal balloon markers. F, Completion control angiogram shows complete occlusion of the aneurysm sac with preservation of the incorporated anterior choroidal artery. The 40-month follow-up MR angiogram source (G) and MIP reconstruction (H) images show no recurrence (asterisk) and a patent anterior choroidal artery (white arrow).

A 27-year-old woman with underlying Moyamoya disease and an unruptured basilar tip aneurysm. A, The 3D reconstruction image shows an unruptured basilar tip aneurysm with a deep lobulation. B, A spot image shows coil placement after positioning 2 microcatheter tips (arrowheads) in the large and small lobes of the sac, respectively, and horizontal stent placement (arrows) via the posterior communicating artery. C, Completion control angiogram shows uniform coil packing of the lobulated sac, resulting in complete occlusion of the aneurysm.

A 59-year-old woman presenting with an unruptured right ophthalmic artery aneurysm. A, The 3D reconstruction shows a wide-neck and shallow aneurysm with incorporation of the ophthalmic artery. Arrows indicate the ophthalmic artery. Unsubtracted angiogram (B) and flat panel CT (C) after Neuroform stent placement show 2 microcatheter tips in the aneurysm sac, one of which faces the ophthalmic artery origin. Black arrows indicate the struts of the Neuroform stent, and white arrows indicate the ophthalmic artery. Note that the 1 catheter tip (white arrowhead) faces the ophthalmic artery origin and the other catheter tip (black arrowhead) faces the aneurysm dome. D, While a helical 1.5 mm × 2 cm coil (arrowheads) occupies the region (arrow) where the ophthalmic artery branches off and the stent protects the aneurysm neck, an initial coil basket is successfully formed by using the other catheter. E, After retrieval of the protection coil, the initial coil basket is stable and the region from which the ophthalmic artery branches off is well-preserved. F, Completion angiogram indicates that the aneurysm was nearly completely embolized with intentional preservation of the region from which the ophthalmic artery (arrows) branches off. G, The 6-month follow-up MR angiogram source image shows no recurrence. The arrow indicates the ophthalmic artery origin, and arrowheads indicate the coiled aneurysm.
Given the accumulation of experience since the previously reported cases series,6,9,11,12 the complexity of the technique used has not limited the ability to obtain satisfactory results. In the cases focused on preserving an incorporating branch, interleaving 2 coils stabilized the initial coil basket to preserve the incorporated branch, while the overinflated balloon prevented coils from moving toward the incorporated branch (Fig 1). In other cases with a very wide neck and a shallow aneurysm with an acute-angled incorporating branch, a multicatheter-plus-stent system was a more reliable choice than a multicatheter-plus-balloon system (Fig 3). Overall, stents (67.7%) have been used more than balloons (32.3%) for covering the wide neck, but in ruptured cases, balloons (75.0%) were preferred because stents may be associated with hemorrhagic complications.17 For cases with a very wide neck and deep lobulation, each lobe of the aneurysm was selected by using 2 microcatheters that had different distal tip shapes (preshaped or steam-shaped). Each lobe could be completely embolized with different coils suitable for the respective shape and size during the protection of the parent artery from coil protrusion by the stent (Fig 2).
When using the combined technique for a branch-incorporated aneurysm, the embolizing coil size was matched to the aneurysm depth, rather than the largest or mean diameter of the aneurysm, with an oversized stent or a supercompliant balloon (HyperForm). When the incorporated branch was intended to be protected with a coil, the appropriate preshaped or steam-shaped catheter was used for facing the origin of the incorporated branch (Fig 3 and On-line Fig 1). Usually, for facing the catheter tip to the origin of an ophthalmic artery or an acutely angled middle cerebral artery branch, a preshaped S (Stryker Neurovascular, Fremont, California) or steam-shaped S catheter was useful. As a protection coil for a small incorporated branch, a helical coil with size matched to or slightly greater than the size of the origin of the incorporated branch was chosen (Fig 3 and On-line Fig 1). The complex or 3D coil was occasionally useful for protection of a relatively larger incorporated branch such as a fetal-type posterior cerebral artery. For the deeply lobulated and shallow aneurysm without an incorporated branch, the appropriate preshaped or steam-shaped catheters were chosen for facing each catheter tip to the respective lobe of the aneurysm. Then each coil size was matched to or slightly greater than the largest size of each lobe. If possible, the stent size was matched to the parent artery size. The balloon was not overinflated, with room for coil placement. Thus, most often 2 coils were packed in each lobe partially intermingling at the confluence of each lobe (Fig 2). After we made a stable coil basket, smaller helical coils were always used for further coil packing without breaking the initial shape of the coil basket.
A major concern about the combination technique for coiling of a complex aneurysm is a possibly increased risk of treatment-related complications resulting from unfavorable aneurysm geometry and the use of additional instruments. The overall incidence of treatment-related complications was reported to be 7.9%–17.1% and 9.4%–12.2% with balloon- and stent-assisted techniques, respectively.1,18⇓⇓–21 The multicatheter technique also ranged from 0% to 13.3%.5,13,22,23 Notably, in our series, treatment-related morbidity occurred in only 1 patient (1.6%), which is acceptable in comparison with the reported results from the literature focusing only on wide necks and is also remarkable because adding an adjunctive device may lead to an increase in adverse events like thromboembolism and intraprocedural rupture.24,25
Another concern is a possible increase in the recanalization rate after frequent incomplete coiling due to the complicated characteristics of the aneurysm. However, through the combination technique, only 1 incomplete coiling occurred in our study. Although there was a 14% recurrence (3 major and 4 minor recurrences) on follow-up imaging (mean, 21 months), this recurrence rate is favorably comparable with the results reported in the literature.4,15,20,21,24⇓–26 An intentional dog-ear remnant in coiling of a branch-incorporated aneurysm cannot be helped, though a dog-ear remnant may be a risk factor for recurrence. There was, however, no significant predictor of recurrence in this study. It may be due to the small number of cases included. Another explanation is that because an incorporated branch was mostly a small or tiny branch except for the posterior communicating artery, hemodynamic stress due to the incorporated branch might also be a little increased and less likely to affect the recurrence rate. In addition, in the case series of coiling of a branch-incorporated aneurysm, the recurrence rate was not greater than those in the literature.6 Finally, all 3 major recurrent aneurysms were successfully retreated by additional coiling without any complications.
A flow diverter may be an effective alternative to coiling for these complex aneurysms.27 Unfortunately, no type of flow diverter was launched in our country until November 2014, so it was not available during the study period.
Our series demonstrated that the combination technique is not related to a higher complication rate than a single adjunctive device for the treatment of complex aneurysms. Furthermore, the combination strategy for complex aneurysms had a safety and effectiveness favorably comparable with the single adjunctive endovascular techniques in previous studies.1⇓–3,8,9,13⇓–15,17⇓–19,22⇓⇓⇓–26
Our study had several limitations due to its retrospective design and the relatively small number of cases. Therefore, the selection bias was inevitable, but it might be somewhat lowered because our data of endovascular treatment were consecutively and prospectively registered. Second, although we preferred balloons to stents in ruptured cases on the basis of the literature,17,21 we were not able to demonstrate which device was better for complex aneurysms. Third, angiographic follow-up was not available in all cases; therefore, this lack of follow-up may have somewhat underestimated the recurrence rate. In addition, 7 of the 50 patients who underwent follow-up imaging were followed by MR angiography alone. This type of follow-up might underestimate the recurrence rate a little further.
Finally, this study did not have a control group. Many of the aneurysms might be coilable by using balloon remodeling or stent assistance, and even a single microcatheter. Actually, Kim et al reported a case series about the coiling of a branch-incorporated aneurysm by using multicatheter, balloon, or stent.6 Also, a lobulated aneurysm can be coilable by using a multicatheter or single catheter plus a balloon or stent. However, in our experience, this type of coiling took longer and was technically more demanding. In our own experience, the longer it took for coiling, the more frequently procedure-related (especially thromboembolic) complications occurred. Furthermore, in a few cases in which the aneurysm was shallow and had a wide neck and a branch incorporated, it was very difficult to complete coiling by using a single catheter plus balloon/stent or multicatheter. In our own cases in this study, we thought that a combination of multicatheter plus balloon or stent made the coiling time shorter and the procedure easier than multicatheter, balloon-remodeled, or stent-assisted technique alone. Therefore, despite these limitations, because this study showed satisfactory results in terms of safety and effectiveness, the combination technique described here may provide helpful information in daily practice.
Conclusions
In this small case series, the combination technique by using a multicatheter plus stent or balloon had very low morbidity and an acceptable recurrence rate for the treatment of a complex aneurysm with a wide neck and an incorporated branch or deep lobulation. The combination technique may be a viable option for coiling of complex aneurysms.
Footnotes
Disclosures: Dong Joon Kim—UNRELATED: Payment for Lectures (including service on Speakers Bureaus): Covidien, Comments: lectures on acute stroke management.
References
- Received April 22, 2015.
- Accepted after revision July 10, 2015.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.