
Article Figures & Data
Figures
- Fig 1.
A 45-year-old man with several months of night-time predominant, right-sided midthoracic pain relieved by ibuprofen. A, Prone axial noncontrast CT image shows a small osteolytic lesion with a central mineralization in the right T5 superior articular facet (black arrow). B, Prone axial noncontrast CT image shows the radiofrequency ablation probe in the nidus of the osteoid osteoma (black open arrow). C, Prone axial noncontrast CT image shows an 18-ga spinal needle placed in the right T4–T5 neural foramen for temperature monitoring, carbon dioxide injection, and cooled dextrose 5% in water infusion. Note the gas tracking into the soft tissue and within the epidural space (white arrow).
- Fig 2.
A 14-year-old boy with painful right transverse process C7 osteoid osteoma (A, arrow). Preprocedural neck CT angiography demonstrates the course and location of the right vertebral artery (B, arrow). C, Thermal monitoring and protection are achieved by placement of a thermocouple and spinal needle in the right C7–T1 neuroforamen. D, RF ablation is performed by using a bipolar navigational probe with slight posterior articulation of the probe tip for optimal positioning.
- Fig 3.
A 13-year-old girl who had cervicothoracic junction pain due to a T1 osteoblastoma. Axial (A) and sagittal (B) CT demonstrates an osteolytic lesion within the anterior aspect of the T1 spinous process with cortical thickening and sclerosis surrounding the lesion. C, Prone axial maximum-intensity-projection image of a T1 osteoblastoma during laser ablation demonstrates 2 posterior laser photoelectrodes (black arrow) within the lesion and 2 anterior spinal needles (white arrow) placed for temperature monitoring.
- Fig 4.
A 17-year-old boy with low back pack due to a right L4 aneurysmal bone cyst. A, Axial T2-weighted image demonstrates an expansile lesion in the right L4 transverse process, pedicle, and posterior vertebral body with multiple fluid-fluid levels, most compatible with aneurysmal bone cyst. B, Axial CT image during cryoablation of the transverse process portion of the lesion. Note the hypoattenuating ice ball (white arrows) extending beyond portions of the lesion into the soft tissues. A spinal needle (black arrow) was placed into the epidural space for temperature monitoring and carbon dioxide injection (white asterisk) into the epidural space. C, Axial CT image during cementoplasty of the right L4 pedicle and posterior vertebral body components of the lesion. D, Axial T2-weighted image 3 months posttreatment demonstrates near-complete resolution of the expansile component of the tumor (white asterisk) and hypointense cement (white arrow) in the right pedicle and posterior vertebral body.
- Fig 5.
A 46-year-old man with upper back pain due to an aggressive T3 hemangioma. A, Axial contrast-enhanced CT scan demonstrates an aggressive T3 hemangioma with intraosseous and extraosseous components. B, Axial prone intraprocedural CT scan during a venogram performed via an 18-gauge needle in the left pedicle/vertebral body. Note extensive vascularity in the vertebral body and in the soft tissues surrounding the vertebral body, including the epidural space. C, Sagittal maximum-intensity-projection CT of a T3 venogram before alcohol ablation demonstrates a vascular lesion with epidural flow. Ethanol ablation was followed by vertebral augmentation for stabilization of the vertebral body. D, Post-alcohol ablation and vertebral augmentation CT demonstrates cement filling the vertebral body and the hyperattenuating ablated extraosseous component posterior to the vertebral body (white arrow).
- Fig 6.
A 71-year-old man with chronic low back pain. A, Lateral radiograph of the lumbar spine shows an enlarged L2 vertebral body with cortical and trabecular thickening (asterisk), with a presumed diagnosis of Paget disease. B, Sagittal T1-weighted MR image of the lumbar spine shows vertically oriented trabecular thickening and enlargement of the L2 vertebral body (asterisk). C, Fluoroscopic image during vertebral augmentation shows cement filling the L2 vertebral body. At the conclusion of the procedure, the patient reported complete resolution of back pain.
- Fig 7.
A 49-year-old woman with chronic midback pain. A, Sagittal STIR MR image of the thoracic spine demonstrates a large Schmorl node (arrow) along the superior endplate of the T10 vertebral body with associated hyperintensity. B, Lateral fluoroscopic image of the lower thoracic spine during kyphoplasty demonstrates filling of the anterior half of T10 vertebral body extending to surround the Schmorl node. Before the procedure, the patient had 6/10 pain. After the procedure, there was near-complete resolution of pain.
- Fig 8.
A 55-year-old man with cement leakage following radiofrequency ablation and vertebral augmentation. Sagittal (A) and axial (B) fat-suppressed T1-weighted contrast-enhanced MR images show hypointense cement within the epidural space, compatible with a leak (A and B, white arrow). Note enhancing granulation tissue along the transpedicular needle tracts (B, black arrows).
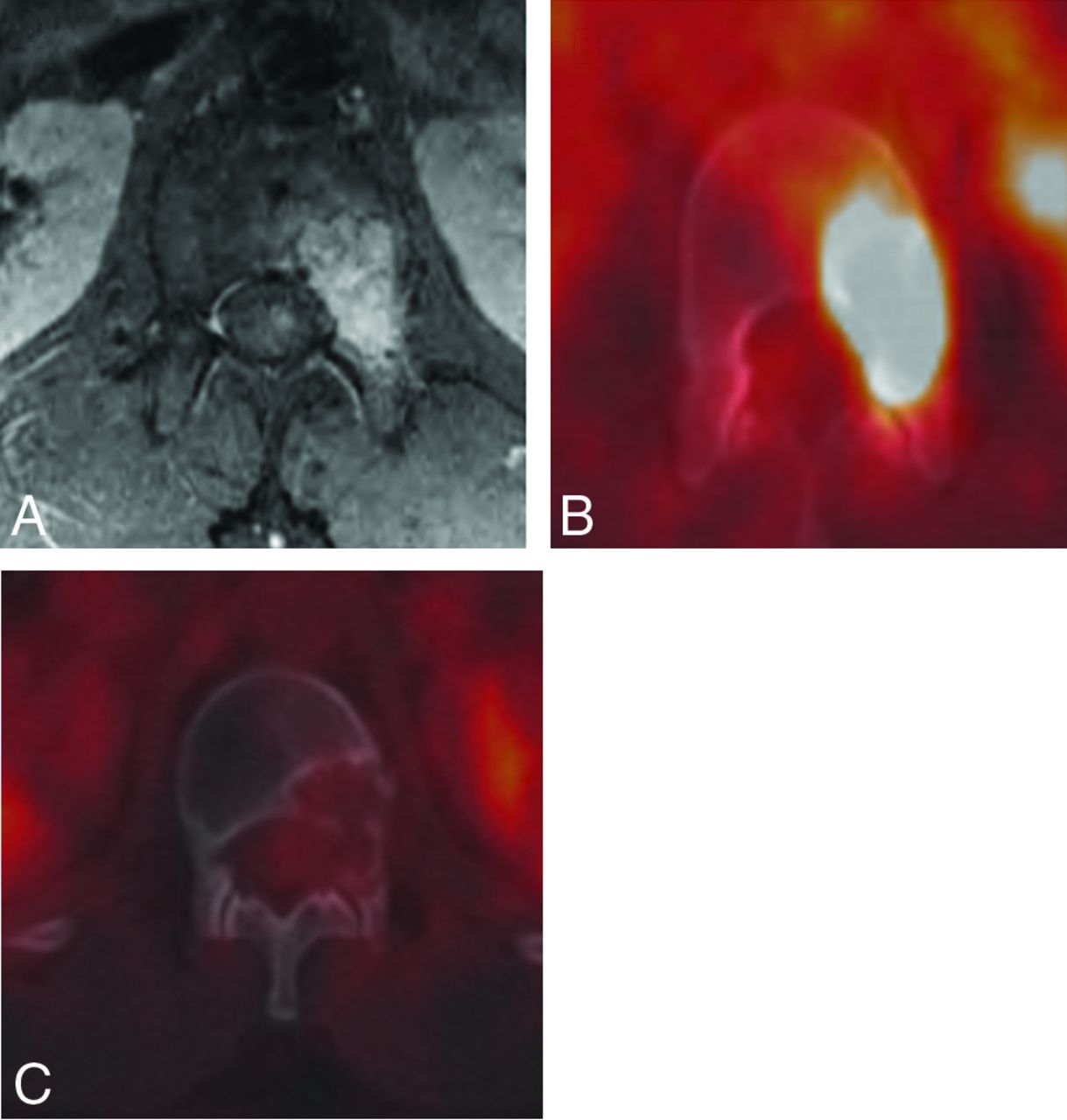
- Fig 9.
A 21-year-old man with L1 pseudomyogenic hemangioendothelioma. A and B, MR imaging and PET-CT demonstrate an enhancing hypermetabolic bone marrow–replacing lesion within the L1 vertebra involving the left pedicle and posterior vertebral body. C, PET-CT performed 1 year following RFA demonstrates no evidence of residual or recurrent tumor.









Tables
Summary of benign spine lesions and preferred treatment modalities
Benign Spine Lesion Recommended Treatment Modality Osteoid osteoma Radiofrequency ablation, laser ablation Osteoblastoma Cryoablation (if large or coexisting soft-tissue component)
Radiofrequency ablation, laser ablationAneurysmal bone cyst Cryoablation (due to involvement of posterior elements, soft-tissue component, and large size) Cementation if extensive vertebral body involvement or pathologic fracture Preablation embolization suggested Hemangioma Vertebral augmentation, alcohol ablation Paget disease Vertebral augmentation Schmorl node Vertebral augmentation





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}