
Abstract
BACKGROUND AND PURPOSE: Few studies have shown MR imaging features and ADC correlating with molecular markers and survival in patients with glioma. Our purpose was to correlate MR imaging features and ADC with molecular subtyping and survival in adult diffuse gliomas.
MATERIALS AND METHODS: Presurgical MRIs and ADC maps of 131 patients with diffuse gliomas and available molecular and survival data from The Cancer Genome Atlas were reviewed. MR imaging features, ADC (obtained by ROIs within the lowest ADC area), and mean relative ADC values were evaluated to predict isocitrate dehydrogenase (IDH) mutation, 1p/19q codeletion status, MGMT promoter methylation, and overall survival.
RESULTS: IDH wild-type gliomas tended to exhibit enhancement, necrosis, and edema; >50% enhancing area (P < .001); absence of a cystic area (P = .013); and lower mean relative ADC (median, 1.1 versus 1.6; P < .001) than IDH-mutant gliomas. By means of a cutoff value of 1.08 for mean relative ADC, IDH-mutant and IDH wild-type gliomas with lower mean relative ADC (<1.08) had poorer survival than those with higher mean relative ADC (median survival time, 24.2 months; 95% CI, 0.0–54.9 months versus 62.0 months; P = .003; and median survival time, 10.4 months; 95% CI, 4.4–16.4 months versus 17.7 months; 95% CI, 11.6–23.7 months; P = .041, respectively), regardless of World Health Organization grade. Median survival of those with IDH-mutant glioma with low mean relative ADC was not significantly different from that in those with IDH wild-type glioma. Other MR imaging features were not statistically significant predictors of survival.
CONCLUSIONS: IDH wild-type glioma showed lower ADC values, which also correlated with poor survival in both IDH-mutant and IDH wild-type gliomas, irrespective of histologic grade. A subgroup with IDH-mutant gliomas with lower ADC had dismal survival similar to that of those with IDH wild-type gliomas.
ABBREVIATIONS:
- IDH
- isocitrate dehydrogenase
- max
- maximum
- min
- minimum
- rADC
- relative ADC
- rADCmean
- mean relative ADC
- TCGA
- The Cancer Genome Atlas
- WHO
- World Health Organization
Gliomas are a heterogeneous group of tumors, and the clinical aggressiveness and prognoses are diverse among different histopathologic grades and molecular subtypes. Previous studies have shown that histopathologic classification of diffuse gliomas has high interobserver variation and correlates imperfectly with clinical outcomes.1,2 Nevertheless, molecular markers, particularly isocitrate dehydrogenase (IDH) mutational status, have been demonstrated to be significant and more robust prognostic markers3 and have been incorporated into the classification of diffuse gliomas in the latest update of the World Health Organization (WHO) classification in 2016.4 IDH mutation, a powerful prognostic marker of improved survival in diffuse glioma, is found mainly in lower grade gliomas (WHO grades II and III), but also in glioblastoma (WHO grade IV), though at much lower frequency.5,6
Preoperative and noninvasive determination of molecular subtyping is of great value in the clinical management of patients with glioma. However, studies correlating MR imaging features with IDH-mutation status and patient survival in diffuse gliomas are scarce. Recently, we showed that the “T2-FLAIR mismatch sign,” detectable using conventional MR imaging, is a highly specific imaging biomarker for the IDH-mutant, 1p/19q noncodeleted molecular subtype in lower grade gliomas.7 Wang et al8 demonstrated that the absence of contrast enhancement was associated with longer progression-free and overall survival in patients with IDH1-mutated anaplastic gliomas. MR spectroscopy could detect 2-hydroxyglutarate, a metabolite that accumulates in IDH-mutant gliomas but did not discover a survival difference.9 Blood volume estimates obtained by MR perfusion have also provided potential markers for noninvasive assessment of IDH status.10
ADC can be calculated from DWI, and tumors with more freely mobile water molecules and lesser cellularity have higher ADC values.11 ADC has been shown to be a valuable imaging marker in the diagnosis of intracranial lesions as well as in grading brain tumors.11⇓⇓⇓–15 Therefore, we hypothesized that ADC values obtained from conventional MR imaging could correlate with molecular subtype and patient survival in adult diffuse gliomas.
Materials and Methods
This was a retrospective study using data from the publicly available National Institutes of Health/National Cancer Institute–approved databases of The Cancer Genome Atlas (TCGA; https://cancergenome.nih.gov) and The Cancer Imaging Archive (http://www.cancerimagingarchive.net/),16⇓–18 from which all 461 cases with imaging data were reviewed, and only cases of treatment-naïve diffuse gliomas (WHO grades II–IV) with available DWI and ADC maps were included. WHO grade, the status of 3 validated molecular prognostic markers (IDH mutation, 1p/19q codeletion, MGMT promoter methylation), and survival data were retrieved from The Cancer Genome Atlas. MR images were reviewed, in consensus, by 2 board-certified neuroradiologists (with 8 and 17 years of experience) who were blinded to pathologic and molecular diagnosis. The order of cases viewed was randomized to avoid bias.
Each tumor was scored for 9 MR imaging features according to the following criteria modified from the Visually Accessible Rembrandt Images MR imaging feature set19: T2 signal intensities (higher than gray matter or mixed [the presence equal to or darker than that of gray matter part]); T2 homogeneity (homogeneous or heterogeneous); margin (well-defined or not well-defined [either infiltrative or irregular]); edema (none to minimal or mild to marked); enhancing pattern (non-/minimally enhancing or enhancing); portion of enhancing area (<50% or ≥50%); the presence of cystic areas (presence or absence); and the presence of necrotic areas (presence or absence). We investigated the relationship among 9 different MR imaging features and 3 molecular markers (IDH mutation, 1p/19q codeletion, and MGMT promoter methylation) as well as WHO grade and overall survival.
Diffusion-weighted images were analyzed using OsiriX Imaging Software (http://www.osirix-viewer.com). ADC measurements were generated by manually drawing 3 nonoverlapping ROIs ranging from 40 to 60 mm2 within the region of lowest ADC values within the solid component of each tumor on ADC maps. The ADC value was also calculated from contralateral normal-appearing white matter by drawing a single ROI with a size similar to that of a tumoral ROI. We obtained mean, minimum (min), and maximum (max) ADCs of each tumor, respectively, by averaging the 3 ROIs; and relative ADC (rADCmean, rADCmin, and rADCmax) was calculated by dividing the tumor ADC by the ADC of the contralateral normal-appearing white matter.
Statistical Analysis
The Kolmogorov-Smirnov test was used to determine whether the numeric data (age and relative ADC values) for each group were normally distributed. Independent variables (clinical parameter and MR imaging features) were compared using the χ2 test among different molecular groups. Normally distributed continuous variables (eg, age) were compared using the independent t test or ANOVA test, and non-normally distributed continuous variables (rADCmean, rADCmin, and rADCmax) were compared using the Mann-Whitney U test among different molecular groups. The intraobserver reliability of ADC value measuring was tested using intraclass correlation coefficients. The optimal cutoff value of each rADC was obtained from receiver operating characteristic curve analysis when the Youden index reached a maximum. Survival curves were estimated and plotted by the Kaplan-Meier method with log-rank tests to compare Kaplan-Meier curves among groups. Variables were first analyzed by the univariate model. MR imaging features and clinical and molecular parameters (including age, sex, WHO grade, MGMT promoter methylation status, IDH mutation status, and 1p/19q codeletion status) with statistical significance in univariate analysis (P < .05) were entered into a Cox proportional hazards ratio model for multivariate analysis. Statistical significance was defined as P < .05 for all tests. The statistical analyses were performed using the statistical software package SPSS 23.0 (IBM, Armonk, New York) and R statistical and computing software, Version 3.3.2 (http://www.r-project.org).
Results
A total of 131 (59 [45%] IDH wild-type and 72 [55%] IDH-mutant) gliomas were included in this study. Of the 72 IDH-mutant tumors, 26 (36%) were 1p/19q codeleted and 46 (64%) were non-1p/19q codeleted. Patients in the IDH wild-type group (mean, 60 ± 12.2 years) were significantly older than those in the IDH-mutant group (mean, 45.1 ± 13.9 years), and patients with IDH-mutant, 1p/19q codeleted gliomas (mean, 50.7 ± 13.9 years) were older than those with IDH-mutant, non-1p/19q codeleted gliomas (mean, 41.9 ± 12.9 years) (P = .01).
Correlation between Conventional MR Imaging Features and Molecular Subtypes
Among the conventional MR imaging characteristics, IDH wild-type gliomas were more likely to exhibit enhancement (P < .001), >50% enhancing area (P < .001), absence of cystic area (P = .013), the presence of necrosis (P < .001), and the presence of edema (P < .001). Within the IDH-mutant group, there were no MR imaging characteristics to differentiate 1p/19q codeletion status using the features tested (Table 1).
MR imaging features and IDH-mutation and 1p/19q codeletion status
Correlation between rADC Values and Molecular Subtypes
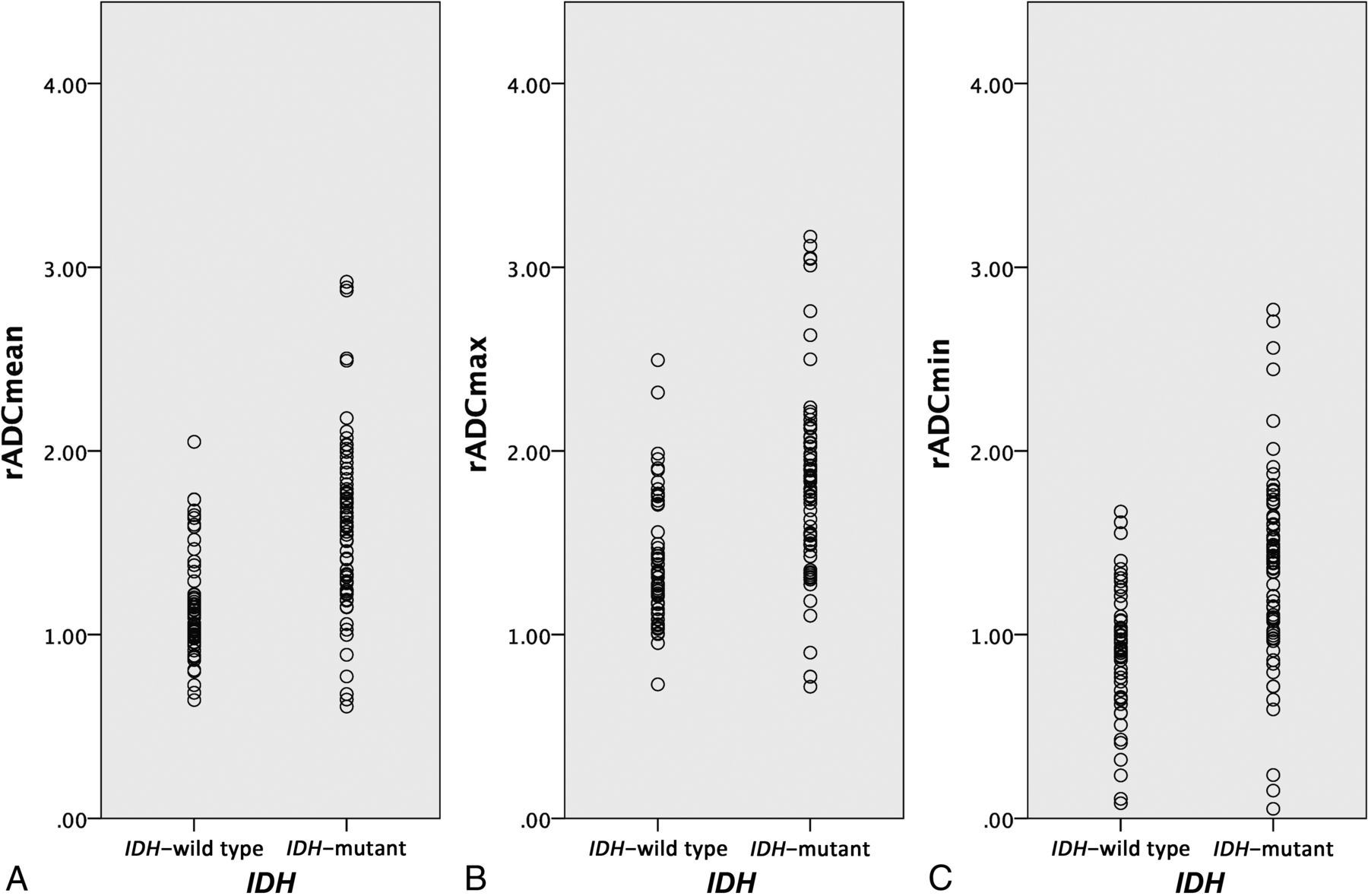
Median rADCmean, rADCmin, and rADCmax values of IDH wild-type gliomas were significantly lower than those of IDH-mutant gliomas (P < .001) (Fig 1 and Table 1). Within the IDH-mutant glioma cohort, rADC values trended lower in 1p/19q codeleted gliomas than in noncodeleted gliomas; however, this trend did not reach statistical significance. Receiver operating characteristic analysis identified an rADCmean of 1.2 as the optimal cutoff value to differentiate IDH wild-type and IDH-mutant gliomas irrespective of WHO grade, with the best combination of sensitivity (81.9%) and specificity (74.6%) and area under the curve (0.790; 95% CI, 0.707–0.869; P < .001). In the analysis of intraobserver reliability, the intraclass correlation coefficients indicated a good correlation of the first evaluator (intraclass correlation coefficient, 0.951; 95% CI, 0.829–0.987; P < .001) and the second evaluator (intraclass correlation coefficient, 0.926; 95% CI, 0.785–0.975; P < .001).

Boxplot representation of rADCmean values by glioma IDH genotype.
Correlation between rADC and Overall Survival
Median overall survival was 25.4 months (95% CI, 19.0–31.7 months), and overall cumulative survival rates were 79% at 1 year, 59% at 2 years, 42% at 3 years, and 36% at 5 years in all 131 cases. Univariate survival analysis found survival to be significantly related to 6 MR imaging features, including T2 homogeneity, enhancing pattern, enhancing areas, presence of necrosis, rADCmean, and rADCmin values, in addition to age, WHO grade, MGMT promoter methylation status, IDH-mutation status, and 1p/19q codeletion status.
Multivariate analysis identified IDH status and rADCmean as the only prognostic factors that independently impacted overall survival after considering the WHO grade, MGMT promoter methylation, and 1p/19q codeletion status and adjusting for patient age. Specifically, IDH-mutant gliomas had significantly longer overall survival (median, 62.0 months) than IDH wild-type gliomas (median, 14.7 months) (P < .001 by log-rank test; age-adjusted hazard ratio, 13.5; 95% CI, 4.8–38.4; P < .001 by multivariate Cox analysis). Overall cumulative survival rates were 97% at 1 year, 71% at 3 years, and 61% at 5 years in IDH-mutant gliomas, and 76% at 1 year and 13% at 3 years in IDH wild-type gliomas. Gliomas with higher rADCmean had longer overall survival compared with those with lower rADCmean (P = .001 by univariate regression; age-adjusted hazard ratio, 0.17; 95% CI, 0.1–0.6; P = .004 by multivariate Cox analysis). No statistically significant differences were noted for the remaining MR imaging features, WHO grade, MGMT promoter methylation status, and 1p/19q codeletion status in multivariate analysis.
By means of the area under a time-dependent receiver operating characteristic curve for prediction of survival at 12 months, the optimal cutoff value of 1.08 for rADCmean could differentiate survival differences within both IDH-mutant and IDH wild-type gliomas. Patients having IDH-mutant gliomas with an rADCmean below the cutoff value of 1.08 had poorer survival than those with an rADCmean above 1.08 (P < .001). In addition, median survival associated with IDH-mutant gliomas with a low rADCmean was very poor. Survival time for this group was similar to that of those with IDH wild-type gliomas with either high or low rADCmean (Table 2 and Fig 2). Finally, the rADCmean cutoff value of 1.08 could also distinguish a survival difference within IDH wild-type gliomas (P < .041).
Comparison of overall survival by relative ADC and glioma IDH-mutation status

Kaplan-Meier survival curve subclassification for the present study by relative ADC and IDH genotype. Censored patients are annotated by a asterisks or plus signs. Results of the analysis are provided in Table 2. IDHmut indicates IDH-mutant; IDHwt, IDH wild-type.
Discussion
Mutations in the IDH genes are among the most important diagnostic and prognostic markers of diffuse gliomas.20 Patients with IDH-mutant gliomas have significantly longer survival compared with those with IDH wild-type gliomas, and management of these 2 molecular subgroups differs significantly. Previous studies have investigated the potential of various conventional and advanced MR imaging characteristics, including perfusion, diffusion tensor, and MR spectroscopy, in identifying genetic subtypes of diffuse gliomas.10,21,22 Here, our results indicate that rADC values correlate with IDH mutation status as well as survival in both IDH-mutant and IDH wild-type diffuse gliomas, independent of their WHO grade. Additionally, using rADC, we could identify a particularly poor prognosis subset of IDH-mutant gliomas, with outcomes similar to those in patients IDH wild-type disease. Most important, determining the rADC value is a simple approach that requires no specialized software; hence, our findings potentially have immediate clinical impact.
The mechanism by which IDH-mutant and IDH wild-type gliomas differ in terms of the rADC is not clear; however, it may be related to tumor cellularity. In many previous studies, DWI has shown utility for preoperative grading and outcome of gliomas and for evaluating the response to therapy in patients with glioblastoma.13,23⇓⇓⇓–27 ADC values provide quantitative information that reflects Brownian motion of water molecules within a scanned area and are determined by many factors. Mainly, differences in ADC have been attributed to tumor cellularity but also to the presence of necrosis or cysts and water content in interstitial space.11,13,28 ADC has been shown to correlate inversely with tumor cellularity on histologic examination, one of the main features of the WHO classification of brain tumors. Our results demonstrate that most IDH-mutant gliomas exhibit higher rADCmean values and MR imaging features accordant with their low-grade features, while most IDH wild-type gliomas show necrosis and a lower rADCmean in solid portions, likely representing higher cellularity, which is associated with higher grade features.
Previous studies have observed an association between ADC and IDH status in gliomas. One study of 37 anaplastic astrocytomas showed that the minimum ADC (cutoff point, 0.95 × 10−3 mm2/s) had acceptable discrimination (area under the curve, 0.711; 95% CI, 0.534–0.887) to predict the IDH status.29 Another retrospective study of 112 cases by Tan et al30 demonstrated that fractional anisotropy and ADC from diffusion tensor imaging can detect IDH1 mutation in astrocytomas, with the ratio of ADCmin being the best metric for detecting IDH mutation, regardless of the WHO grade. We found that rADCmean can differentiate IDH wild-type from IDH-mutant gliomas with excellent discrimination, regardless of WHO grade. Our study also emphasizes MR imaging and ADC values correlating well with molecular subtype.
The main novel finding of our study is that preoperative rADC values can distinguish favorable and unfavorable prognosis within both IDH-mutant and IDH wild-type glioma subgroups. While IDH-mutant gliomas generally behave less aggressively and have a better prognosis compared with their IDH wild-type counterparts, we identified a small subset (12.5%) of IDH-mutant gliomas with low rADCmean values and poor overall survival, which was only slightly better (24 months) than that of IDH wild-type gliomas but was not statistically significant. Concordantly, a study by Jiao et al31 revealed that a small subgroup (11.7%) of patients with IDH-mutant gliomas across all grades had a dismal prognosis (median survival of 22 months), more similar to IDH wild-type gliomas and glioblastomas in their cohort. These tumors had distinct genetic characteristics, lacking the typical concurrent genetic alterations observed in IDH-mutant gliomas. In addition, a recent study of The Cancer Genome Atlas identified a small subset (5.5%) of IDH-mutant gliomas with markedly worse survival than other IDH-mutant gliomas, and these tumors were associated with relatively decreased global DNA methylation.32 Together, these data clearly indicate that a subgroup of IDH-mutant gliomas behaves as aggressively as their IDH wild-type counterparts. Although whether the malignant subgroups across these datasets represent the same biology is unknown, our results suggest that rADC values can potentially identify this aggressively behaving IDH-mutant subgroup.
Furthermore, our study highlights how detection of robust imaging-phenotype correlations can be significantly improved by analyzing glioma datasets by molecular subtype rather than by histopathologic classification. We evaluated MR imaging features and prognosis in diffuse gliomas across lower and higher grades in the current study and demonstrated the power of rADCmean to differentiate IDH-mutation status and discrete survival subgroups beyond WHO grade. While many previous studies have demonstrated an inverse relationship between ADC and astrocytoma grade,12,13,28 other studies have shown substantial overlap of ADC values between high-versus-low-grade gliomas3,24,33,34 and no significant differences between grade II versus III35 or grade III versus IV.36,37 These observed variations of ADC in predicting tumor grade are likely due to limitations that make the exact histopathologic classification challenging, with high interobserver variability2 and molecular constituent and clinical behavior being likely different in tumors with the same histopathologic grade.3,4,38,39 Similar to a recent meta-analysis by Zulfiqar et al,27 which showed that low ADC values correlate independently with poor survival in malignant astrocytomas (grades III and IV), we found an inverse relationship between rADCmean values and prognosis for both IDH-mutant and IDH wild-type tumors independent of WHO grade.
One limitation of our study is its retrospective design, which was necessary to include a relatively large number of patients and to correlate with survival, which is relatively long in patients with IDH mutation. A second limitation is that the studied patients had been scanned on different MR imaging magnet types, and ADC maps were generated by diffusion-weighted imaging or diffusion tensor imaging of all collected data. However, a previous study has verified that ADC datasets from 3-directional DWI and 6-directional diffusion tensor imaging could be analyzed together.40 We calculated the rADC to minimize the differences among absolute ADC values across platforms. Third, the treatment regimen applied to each patient was not available to us in many cases. This issue might have potentially impacted the outcome and survival in each case. However, IDH status has been repeatedly shown to be an independent marker of prognosis in independent datasets.4 Finally, the ADC value has previously been reported to predict 1p/19q codeletion status, a marker of oligodendroglioma, in lower grade gliomas.35,41 In the study by Johnson et al,41 the ADC values were calculated from sampling both the highest and lowest ADC areas. However, we did not detect a significant correlation between rADC values and 1p/19q codeletion status. Further investigation of the optimal methods of measuring ADC and physiology correlates of ADC values in genetically defined oligodendroglioma is needed.
Our results require independent confirmation, incorporating emerging molecular markers and accounting for different treatment strategies. However, our results expand on and refine the existing correlation between DWI and tumor genetic markers and highlight its potential role as an independent imaging biomarker that can aid in substratification of patients with gliomas, both IDH-mutant and IDH wild-type. Here, we were able to identify a subset of aggressive IDH-mutant gliomas using ADC values easily obtained from common clinical MR images. Ongoing accumulation of tumorigenesis knowledge, together with imaging studies stratified by molecular subgroup rather than histopathologic features, will likely identify additional robust genetic-imaging-clinical phenotype correlations that will improve early detection of clinically meaningful glioma molecular subtypes.
Conclusions
We demonstrate that ADC values obtained from DWI correlate with IDH-mutation status and overall survival in adult diffuse gliomas. IDH wild-type gliomas showed low ADC values and poor survival compared with IDH-mutant gliomas. Within IDH-mutant gliomas, a small subgroup with lower ADC values had dismal survival, similar to that in IDH wild-type gliomas. ADC values correlated with survival in patients with IDH-mutant and IDH wild-type gliomas regardless of WHO grade. Preoperative ADC estimates may corroborate with molecular subtypes as a prognostic marker and potentially enhance risk stratification, especially within IDH-mutant gliomas.
Footnotes
Chih-Chin Wu and Rajan Jain contributed equally to the article.
Disclosures: Dimitris Placantonakis—UNRELATED: Grants/Grants Pending: National Institutes of Health, R01 NS102665, NY State Stem Cell Program - DOH01-STEM5-2016-00221//C32595GG*; Patents (Planned, Pending or Issued): method for treating high-grade gliomas*. *Money paid to the Institution.
References
- Received April 25, 2018.
- Accepted after revision July 2, 2018.
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Identification of Multiclass Pediatric Low-Grade Neuroepithelial Tumor Molecular Subtype with ADC MR Imaging and Machine Learning
- MR Imaging Characteristics and ADC Histogram Metrics for Differentiating Molecular Subgroups of Pediatric Low-Grade Gliomas
- Prognostic Value of Preoperative MRI Metrics for Diffuse Lower-Grade Glioma Molecular Subtypes
- New Radiological Classification of Glioma and validation with the survival analysis