
Abstract
BACKGROUND AND PURPOSE: Differences in structural brain connectivity that underlie inattention have been previously investigated in adolescents with attention deficit/hyperactivity disorder, but not in the context of premature birth, which is often associated with attentional problems. The purpose of this study was to identify the neural correlates of attentional problems in adolescents born prematurely and determine neonatal predictors of those neural correlates and attention problems.
MATERIALS AND METHODS: The study included 24 adolescents (12.5 ± 1.8 years of age; 12 girls, 12 boys) who were born prematurely and underwent MR imaging of the brain and cognitive assessment, both shortly after birth and as adolescents. Structural connectivity was assessed at adolescence using diffusion tensor imaging and tractography.
RESULTS: Of the 24 subjects, 12 had attention deficits. A set of axonal pathways connecting the frontal, parietal, temporal, and occipital lobes had significantly lower fractional anisotropy in subjects with attentional problems. The temporoparietal connection between the left precuneus and left middle temporal gyrus was the most significantly underconnected interlobar axonal pathway. Low birth weight and ventriculomegaly, but not white matter injury or intraventricular hemorrhage on neonatal MR imaging, predicted temporoparietal hypoconnectivity in adolescence. However, neither birth weight nor other neonatal characteristics were associated with attention deficits directly.
CONCLUSIONS: We identified an aberrant structural brain connectivity pattern, involving temporoparietal hypoconnectivity, in prematurely born adolescents with attentional problems. We also identified birth weight as a potential neonatal predictor of the temporoparietal hypoconnectivity. These findings add to our understanding of the neural basis and etiology of inattention in adolescents after premature birth.
ABBREVIATIONS:
- ADHD
- attention deficit/hyperactivity disorder
- AAL
- Automated Anatomical Labeling
- FA
- fractional anisotropy
- FDR
- false discovery rate
- TOVA
- Test of Variables of Attention
- WMI
- white matter injury
About 1 in 10 children are born prematurely and, as a result, enter the world with a higher risk of several health problems as well as early death.1 Those who survive often have life-long neurodevelopmental problems, with attention deficit being among the most consistently reported cognitive impairment related to prematurity.2 This deficit impacts daily functioning, and many individuals meet the formal diagnostic criteria for attention deficit/hyperactivity disorder (ADHD).3 It is essential to better understand the underlying neurologic causes of attentional problems and their etiologies to develop effective interventions.
Diffusion tensor imaging allows noninvasive assessment of white matter microstructure.4 This methodology enables 3D visualization of white matter properties and has been used for several decades to study neurologic and psychiatric disorders in an attempt to relate white matter abnormalities to clinical manifestations.5 A commonly used metric derived from DTI is fractional anisotropy (FA). A general, simplified interpretation is that higher FA represents higher white matter integrity in specific brain regions. With regard to attentional problems, several studies have focused on the FA in the brains of individuals with ADHD, reporting both higher6⇓–8 and lower9⇓–11 FA values compared with healthy controls. The effects of premature birth on DTI parameters have also been investigated, showing that children born prematurely tend to have lower FA values in several regions of the brain consistently from infancy to adulthood.12⇓⇓⇓–16
Recently, neurologic and psychiatric disorders, including ADHD, are increasingly being viewed not as anomalies of focal brain regions but rather as disorders arising from disruption of distributed brain networks (connectomes).17 These networks are modeled as sets of nodes, with pairs of nodes connected by edges. In a structural connectivity study, cortical and subcortical gray matter structures typically play the role of nodes, whereas tractography-derived white matter connections between them serve as edges. This network approach differs in an important way from the voxel-based DTI approaches in that it moves away from focal abnormalities to network-level disruptions and offers new explanations of observed dysfunctions.
To date, there are 3 studies examining white matter network properties in youth with ADHD.18⇓–20 The main findings include aberrant connectivity of the frontal and striatal regions,18⇓–20 but also parietal,18,20 occipital,18,20 temporal,20 and cerebellar regions.19 One additional study used T1-weighted images and showed differences in topologic properties of structural covariance networks in youth with ADHD compared with controls.21 However, there have been no studies examining structural connectivity associated with inattention in adolescents born prematurely. This is an important gap in knowledge because understanding the underlying mechanisms of attentional dysfunction is crucial for the development of targeted interventions. The purpose of this study was to identify network-level neural correlates of attentional problems in adolescents born prematurely and assess neonatal predictors of those neural correlates.
Materials and Methods
Participants and Clinical Information
The study was approved by the local institutional review board, and all participants in the study provided written informed assent, and their parents or legal guardians provided written informed consent in accordance with the Declaration of Helsinki. Prematurely born adolescents who were enrolled in a longitudinal MR imaging study of preterm infants were invited to return for optional MR imaging and neuropsychological testing at 10–14 years of age. Inclusion criteria for the cohort were birth before 33 weeks' gestation. Exclusion criteria included clinical evidence of a congenital malformation or syndrome, congenital infection, or clinical status too unstable for MR imaging. The group included in this study consisted of 24 adolescents (10–14 years of age; average age, 12.5 ± 1.8 years; 12 girls and 12 boys) who were born prematurely (including 11 extremely premature subjects, <28 weeks' gestation) and came for the 10- to 14-year follow-up visit and had both neuropsychological and diffusion MR imaging data available.
Neonatal Clinical Assessments
Trained research nurses blinded to the MR imaging findings reviewed medical records and extracted clinical data. Maternal and antenatal variables included exposure to prenatal steroids as well as maternal age, primiparity, maternal smoking, placenta previa, preeclampsia, and twin gestation.
Demographic variables included gestational age at birth, birth weight, and sex. The z score for birth weight was calculated. Perinatal variables included placental abruption, chorioamnionitis, and mode of delivery, which was classified as vaginal or cesarean delivery. Chorioamnionitis was diagnosed clinically (maternal fever, >38°C during labor or fetal tachycardia with uterine tenderness, treated with antibiotics).22 Neonatal variables included duration of mechanical ventilation, infection, hypotension, symptomatic patent ductus arteriosus, necrotizing enterocolitis, neonatal surgery, and chronic lung disease. Neonates with culture-positive sepsis, clinical signs of sepsis with blood culture negative for sepsis, or meningitis were classified as having infection. Hypotension was defined as a period of sustained low blood pressure treated with intravenous fluid bolus and/or inotropes. Neonates with clinical signs of patent ductus arteriosus (prolonged systolic murmur, bounding pulses, and hyperdynamic precordium) and evidence of left-to-right flow through the patent ductus arteriosus on echocardiogram were classified as having symptomatic patent ductus arteriosus. Necrotizing enterocolitis was diagnosed according to the Bell stage 2 criteria.23 Chronic lung disease was defined as an oxygen requirement at 36 weeks' postmenstrual age.
Neonatal MR Imaging
MR imaging scans were obtained after birth as soon as the neonates were clinically stable and again near term-equivalent age when possible. A custom MR imaging–compatible incubator with a specialized neonatal head coil was used to provide a quiet, well-monitored environment for the neonates, minimizing patient movement and improving the signal-to-noise ratio.24 MR imaging scans were acquired using a 1.5T scanner and a specialized, high-sensitivity, neonatal head coil built into the MR imaging–compatible incubator. MR imaging scans included axial spin-echo T2-weighted images (TR = 3 seconds; TE = 60 and 120 ms; FOV = 240 mm with a 256 × 256 matrix; slice thickness = 4 mm; gap = 2 mm) and sagittal volumetric 3D spoiled gradient-echo T1-weighted images (TR = 36 ms; minimum TE; FOV = 180 mm; 1.0-mm isotropic). A single pediatric neuroradiologist (A.J.B.) blinded to the clinical history (other than premature birth) evaluated all MR images. The severity of the white matter injury (WMI) on T1-weighted MR imaging was scored according to our published criteria as none, mild (≤3 areas of signal abnormality, each <2 mm in diameter), moderate (>3 areas of signal abnormality or areas of signal abnormality of >2 mm but <5% of the hemisphere involved), or severe (>5% of hemisphere involved).25 WMI was further classified as absent/mild or moderate/severe. Neonates were diagnosed with mild ventriculomegaly if the largest atrial ventricular diameter (at the level of the glomus of the choroid plexus) measured 8–10 mm and with moderate/severe ventriculomegaly if it measured >10 mm.26 Intraventricular hemorrhage was classified according to the Papile grading system.27
Adolescent Attention Assessments
A psychologist blinded to imaging findings administered performance-based measures and parent report forms targeting attention. Attentional problems in most subjects (n = 17 of the 24 subjects included in this study) were evaluated using the Test of Variables of Attention (TOVA), a continuous performance test used to measure the speed and accuracy of attentional processing.28 Negative TOVA Attention Comparison Scores were interpreted as indicative of attentional problems. Six subjects were evaluated using the Conners Comprehensive Behavior Rating Scales, suitable for assessing children ages 6–18. Conners attention t-scores of >60 were interpreted as indicative of attentional problems. One subject was evaluated using the Child Behavior Checklist.29 The Child Behavior Checklist attention t-scores of >66 were interpreted as indicative of attentional problems. The comparability of ADHD-related metrics has been previously reported for the TOVA and Child Behavior Checklist,30 for the Conners Rating Scales and Child Behavior Checklist,31,32 and for the TOVA and Conners Rating Scales.33
Adolescent MR Imaging Data Acquisition and Processing
Each adolescent underwent an hour-long MR imaging protocol using a 3T MR750 MR imaging scanner (GE Healthcare, Milwaukee, Wisconsin) and a 32-channel Nova Medical head coil (Siemens, Erlangen, Germany). The scan included a standard T1-weighted sequence and a spin-echo echo-planar DTI sequence (TR = 7.5 seconds, minimum TE, FOV = 25.6 cm with a 128 × 128 matrix, slice thickness = 2 mm). Diffusion-sensitizing gradients were applied at a b-value of 1000 s/mm2 along 30 noncollinear directions. An array spatial sensitivity encoding technique acceleration factor was set to 2, resulting in a sequence scan time of 4 minutes.
Preprocessing was performed using the FMRIB Software Library (FSL 5.0.8; http://www.fmrib.ox.ac.uk/fsl)34 and Matlab (MathWorks, Natick, Massachusetts). A quality-assurance step was performed, in which diffusion volumes affected by motion were rejected35 and the remaining images were corrected for eddy current distortions, affine head motion, and b-vector rotation. DTI reconstruction and deterministic whole-brain streamline fiber tractography were performed using the Diffusion Toolkit (TrackVis; http://www.trackvis.org/dtk/).36 For whole-brain tractography, the Fiber Assignment by Continuous Tracking algorithm37 with 1 seed per voxel was applied using the entire diffusion-weighted volume as the mask image. Streamlines were terminated if the tract curvature exceeded 35°, a value chosen on the basis of previous work in adolescents.38
Each brain was segmented into ROIs using the Automated Anatomical Labeling (AAL; https://omictools.com/aal-tool) atlas.39 Only 90 cerebral regions were considered, because the cerebellum is often affected by stronger artifacts and is not always fully covered in the FOV.38 T1-weighted data were registered to the B0 volume of the DTI dataset and to the Montreal Neurological Institute space template using the FMRIB Linear Image Registration Tool (FLIRT; http://www.fmrib.ox.ac.uk/fsl/fslwiki/FLIRT).40,41This step allowed the application of the AAL atlas in the DTI space to produce the 90 nodes of the network. The registration and segmentation results were visually inspected for errors. The resultant ROIs were dilated by 1 voxel. To define the connections between the ROIs, we considered only streamlines with at least 5 points, and we used the average FA value within voxels along streamlines connecting the ROIs as a proxy for the connectivity strength.
Statistical Analysis
Adolescent Structural Connectivity Analysis.
Our main assumption was that aberrant connectivity underlies attentional problems. To test whether significant associations between connectivity and attention exists, we performed t tests using attention as the grouping variable. We did not assume that the connections associated with this contrast of interest form a connected component. To control for the massive number of multiple comparisons, we applied a standard link-based controlling procedure, the false discovery rate (FDR). We used the implementation in Matlab by Zalesky et al42 with default parameters (a significance value of .05 and 1000 permutations). In this context, the FDR is referred to as a link-based controlling procedure because each link is treated independently for the sake of the family-wise error rate control.
The rest of the statistical analyses were performed using SPSS Statistics software (Version 25; IBM, Armonk, New York). Neonatal predictors of attentional problems in adolescence were tested using the Kruskal-Wallis test for continuous variables and the Fisher exact test for categoric variables. Neonatal predictors of abnormal structural connectivity associated with attentional problems in teens were investigated using a linear regression model with abnormal connectivity as the dependent variable and neonatal clinical and imaging metrics and the age at the adolescent MR imaging visit as independent variables. Additionally, the number of rejected diffusion volumes affected by motion was compared between the groups of adolescents with normal and abnormal attention using the independent-samples t test.
No matching of intelligence quotient (IQ) was performed in the analyses because this can be problematic in the case of children with attentional problems. On the traditional Wechsler IQ tests, the subtests tend to be rote, repetitive, and require attention and memory and are difficult for a child with attentional problems, and he or she may therefore perform slowly and/or inaccurately.43
Results
Of the 24 adolescents, 12 have been determined to have attention deficits (6 girls/6 boys). There were no statistically significant differences in the number of rejected diffusion-weighted volumes, indicating that adolescents' movements during the MR imaging scan did not differ depending on the attentional problems (t = 1.1, P = .28).
Neonatal Predictors of Attentional Problems in Adolescence
Details about the participants' neonatal characteristics grouped by attentional deficits can be found in Tables 1 and 2. The groups did not differ significantly by sex, gestational age at birth, or birth weight z scores (Table 1). However, there was a group difference in variables that denote increased illness severity, with infection, necrotizing enterocolitis, neonatal surgery, and intubation at birth reaching statistical significance (Table 1). Among neonatal scan results, only WMI at the first neonatal scan indicated a potential difference between the 2 groups with normal and abnormal attention (P = .05) (Table 2).
Neonatal clinical characteristics of the study participantsa
Neonatal scan results for study participants
Adolescent Structural Connectivity Correlates of Attentional Problems
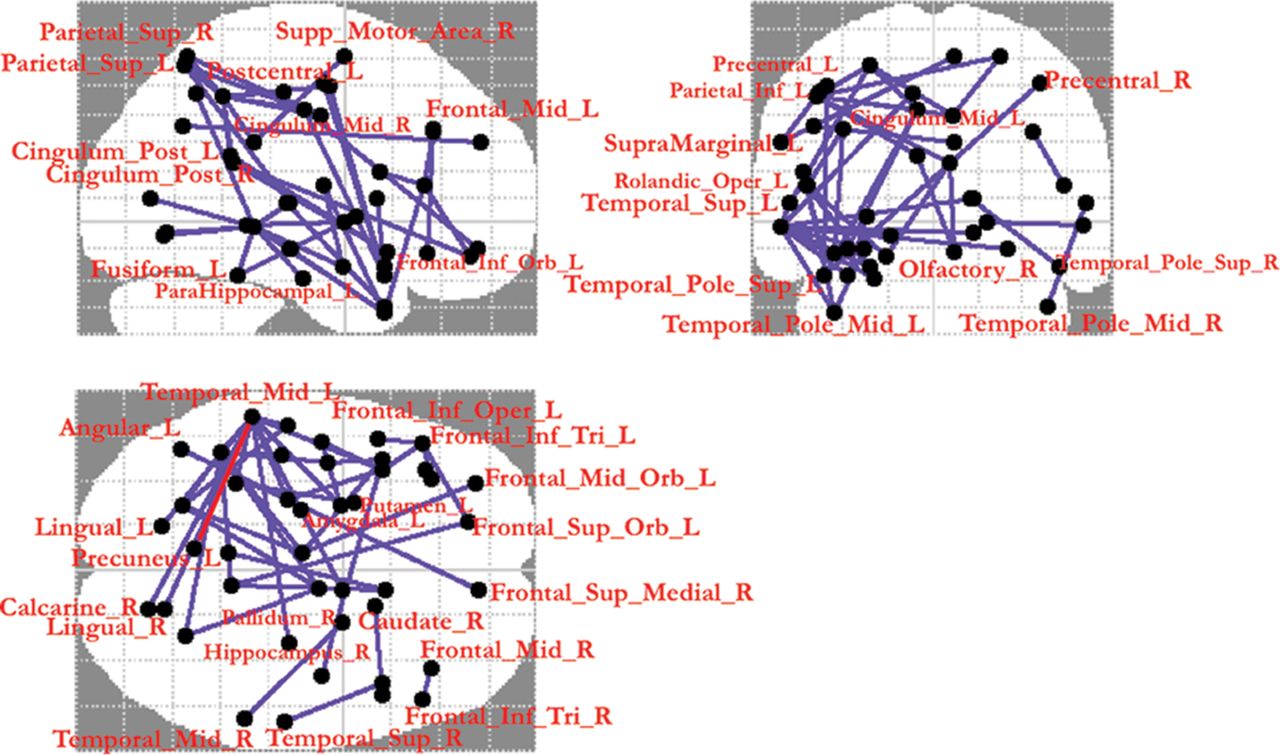
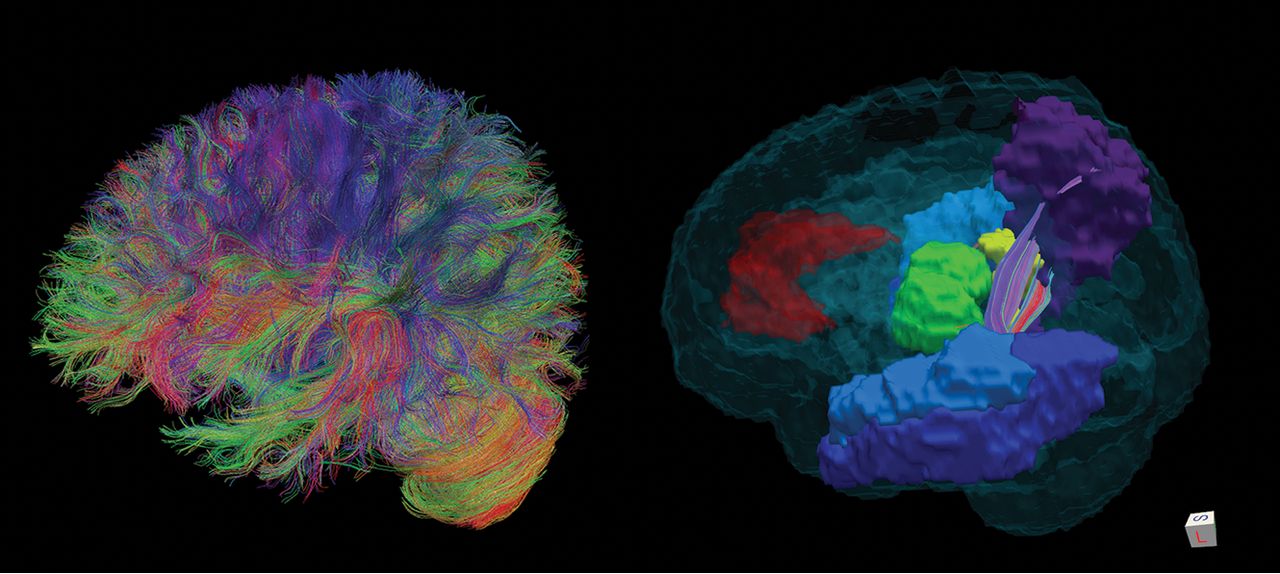
A set of tracts connecting frontal, parietal, temporal, and occipital lobes, including frontal cortices and subcortical regions, had significantly lower FA values in adolescents with attentional problems compared with those with normal attention. Connections that survived the FDR correction are presented in Fig 1 and Tables 3 and 4. Connections of the left middle temporal gyrus were the most prevalent hypoconnected connections (10 connections), and among them, the most statistically significantly hypoconnected interlobular connection was the left precuneus–left middle temporal gyrus connection (test statistic: 4.18; average FA of 0.34 in the inattention group compared with 0.37 in the group with normal attention), which we explored further. Figure 2 shows an example of the participant's tractography streamlines going through the left precuneus and left middle temporal gyrus. None of the connections were stronger in the inattention group compared with the group with normal attention.

Results of the connection-wise group comparison of connectivity matrices using an FDR-corrected t test with 1000 permutations (P = .05). The connections highlighted in blue (46 edges, involving 44 nodes) were statistically significantly weaker in the attention deficit group. The connection highlighted in red, between the left precuneus and left middle temporal gyrus, was the most statistically significantly hypoconnected interlobular connection.
Structural connectivity analysis results (FDR-corrected)—connections with weaker connectivity in the inattention group that survived the FDR correctiona
AAL abbreviations and standardized names of the corresponding brain regions

Left: example of study participant's whole-brain tractography. Right: tractography streamlines going through the left precuneus (purple) and left middle temporal gyrus (blue). The anterior cingulate cortex is shown in red; the thalamus, in green.
Neonatal Predictors of Abnormal Structural Connectivity Associated with Attentional Problems in Adolescents
Linear regression analysis was performed with left precuneus–left middle temporal gyrus connectivity as the dependent variable and neonatal clinical and imaging metrics and the age at the adolescent MR imaging visit as independent variables. Only low birth weight in grams and ventriculomegaly detected at the second neonatal scan independently and statistically significantly predicted hypoconnectivity between the left precuneus and left middle temporal gyrus (t = 4.874, P < .000 and t = 4.617, P < .000, respectively). None of the other variables showed statistical significance (neonatal clinical characteristics listed in Table 1 or neonatal scan results listed in Table 2, or age at the adolescent MR imaging visit). Similar results were obtained using the average FA as the dependent variable: Low birth weight and ventriculomegaly at the second neonatal scan independently and statistically significantly predicted average FA (t = 2.929, P = .010 and t = 2.385, P = .031, respectively). While low birth weight was associated with lower FA, ventriculomegaly was associated with higher FA.
Because only 1 subject had ventriculomegaly, we excluded this subject and performed linear regression with left precuneus–left middle temporal gyrus connectivity as the dependent variable and only birth weight as an independent variable. The results were t = 2.382, P = .027; R2 = 0.213. Figure 3 shows a scatterplot of the variables. The result remained significant when using birth weight z scores.

Linear regression: left precuneus–left middle temporal gyrus connectivity as a dependent variable and birth weight as independent variable.
Discussion
The results of this study indicate that attentional problems in adolescents who were born prematurely may be associated with a weaker structural connectivity among the frontal, parietal, temporal, and occipital lobes, including frontal cortices and subcortical regions. The resulting hypoconnected edges linked to attentional problems in our study are known to underlie general attentional processes. Specifically, the frontoparietal attentional network is known to facilitate voluntary spatial attention, whereas reorienting of attention recruits other brain areas, such as the temporoparietal junction and lateral inferior frontal cortex.44
Our findings are generally supported by previous literature reporting microstructural abnormalities in children formally diagnosed with ADHD and in prematurely born children, as well as by the structural network analysis literature in children with ADHD,18,19 though contradictory results have been reported.20 Among other regions, we detected lower connectivity of the left middle temporal gyrus to other regions in the subjects with attentional deficits. This finding is aligned with results published by Lei et al,45 who observed microstructural abnormalities in the left middle temporal gyrus in children with ADHD, inattentive type. Most interesting, they also observed microstructural disruptions within the right middle temporal gyrus in children with the combined ADHD types compared with controls. Our results indicate a weaker connectivity between the right pallidum and the right middle temporal gyrus in the group with attentional deficits, which is also consistent with those findings.
The conflicting findings within the ADHD literature are, however, of particular interest. Different etiologies might be the reason for some of these differences. Specifically, in a study by Beare et al,20 individuals with ADHD presented with a subnetwork of stronger connectivity encompassing bilateral frontostriatal connections as well as left occipital, temporal, and parietal regions, in which the white matter microstructure was associated with ADHD symptom severity. This result differs from those in 2 previous studies,18,19 as well as from the study described here. The prematurity status was, however, not reported in these prior studies. The only previous study linking prematurity, ADHD, and white matter metrics is the one by Skranes et al,14 which investigated the relationship between clinical findings and FA measurements in white matter of 34 adolescents born prematurely with very low birth weights compared with 47 age-matched controls born at term. In their study, high inattention scores on the ADHD Rating Scale (based on mothers' reports) correlated with low FA values in the right superior and left middle fasciculus.
Previous studies have reported that adolescents with very low birth weights are more likely to have attention and/or executive function deficits compared with controls,46,47 which is consistent with our findings. In our study, low birth weight and ventriculomegaly (but not white matter injury or intraventricular hemorrhage) detected on the neonatal MR imaging were associated with altered temporoparietal connectivity in adolescence. Because ventriculomegaly was only detected in 1 study participant, we do not draw any conclusions. The obtained results are summarized in the model in Fig 4. A potential explanation for the association of low birth weight (but not gestational age) with temporoparietal hypoconnectivity is the substantial risk of children with very low birth weights for perinatal hemorrhages and injury.48 The subsequent hypoconnectivity can be caused by perinatal white matter damage that has long-term effects on myelin disturbances, disorganization, or a reduced number of axons in projectional, commissural, and association tracts.14 Although neonatal white matter injury or intraventricular hemorrhage was not associated with hypoconnectivity in adolescence in our study, this may relate to the lower resolution of MR images 14 years ago when some of the neonatal scans were performed, as well as limited power to detect a difference between groups, given the small sample size. Lower birth weight was also associated with other markers of illness severity, which, in turn, were also linked to inattention, and it is likely that unmeasured variables are a source of residual confounding. Additionally, other factors (eg, parenting style, adverse events, and so forth) may have a strong influence on performance in attentional tasks.

A model that describes the relationship between neonatal characteristics of prematurely born children, structural brain connectivity at adolescence, and attention at adolescence. The model is supported by the findings of this study.
Several methodologic limitations need to be considered when interpreting our findings. First, a DTI-based tractography method was used to reconstruct structural brain networks, which is the most widely used tractography method but is limited in terms of its capacity for resolving crossing fibers.49 Second, our study did not include a typically developing control group or a group of term-born adolescents with attentional problems. Third, the assessment of attention in creating the binary variable of the attention/inattention group was nonuniform across subjects. Finally, the study sample was limited and included only 24 adolescents who came for the 10- to 14 year follow-up visit and had diffusion MR imaging data. Nevertheless, the main result of an aberrant structural connectivity associated with attentional problems was statistically significant after correction for multiple comparisons. This result contributes to our understanding of the mechanisms underlying the development of attentional deficits in children born prematurely and can help direct future studies.
It would be advantageous if future studies of aberrant neural networks in ADHD included information about the gestational age at birth (prematurity) of study participants. Another important step would be a comparison of 4 groups in 1 study: term-born adolescents without attention deficits, term-born adolescents with attention deficits, pre-term-born adolescents without attention deficits, and pre-term-born adolescents with attention deficits.
Conclusions
In this study, we examined network-level neural correlates of attentional deficits in adolescents born prematurely as well as neonatal predictors of those neural correlates and attentional problems. Our major findings are the hypoconnected axonal tracts in the frontal, parietal, temporal, and occipital lobes in adolescents with attentional problems, with temporoparietal connection being the most prominent and low birth weight being a predictor of this hypoconnectivity. This knowledge could lead to a better understanding of the mechanisms that play a role in the development of attentional deficits in children/adolescents born prematurely and could possibly lead to new therapeutic agents and additional interventions.
Acknowledgments
We would like to thank all of the study participants and their parents who made this work possible. We also thank Drs Bridget Johnson and Elizabeth Rogers for their help with the psychological assessments of the study participants. Finally, we thank Laurel Haeusslein, Veronica de Santiago, Shrey Goel, and Kristyn Casalino for the study coordination.
Footnotes
Disclosures: Olga Tymofiyeva—RELATED: Grant: National Institutes of Health, Comments: National Institutes of Health grants P01NS082330, R01HD072074, and R21AT009173*; Support for Travel to Meetings for the Study or Other Purposes: National Institutes of Health, Comments: National Institutes of Health grants P01NS082330, R01HD072074, and R21AT009173*. Dawn Gano—RELATED: Grant: National Institutes of Health*; UNRELATED: Grants/Grants Pending: PERF*. Robert J. Trevino—UNRELATED: Other: Summer Research Training Program at the University of California, San Francisco; Maximizing Access to Research Careers—Undergraduate Student Training for Academic Research (MARC U-STAR), Comments: During my time at the University of California, San Francisco, I was in a living arrangement provided by the Summer Research Training Program at the University of California, San Francisco. I am also partly funded by the MARC U-STAR Program through National Institutes of Health/National Institute of General Medical Sciences MARC U-STAR GM07717. Hannah C. Glass—UNRELATED: medicolegal consulting: various Grants/Grants Pending: National Institutes of Health, Cerebral Palsy Alliance, Pediatric Epilepsy Research Foundation. Donna M. Ferriero—RELATED: Grant: National Institutes of Health*; UNRELATED: Grants/Grants Pending: National Institutes of Health, Cerebral Palsy Alliance*; Royalties: Elsevier for an edited book*. A. James Barkovich—RELATED: Grant: National Institutes of Health, Comments: grant to look at differences in brain injuries and brain structure in children born before 32 weeks' gestational age*. Duan Xu—RELATED: Grant: National Institutes of Health*; UNRELATED: Grants/Grants Pending: National Institutes of Health*. *Money paid to the institution.
This study was supported by P01NS082330 to D.M.F., P.S.M., D.X., and A.J.B.; NICHD R01HD072074 to D.X. and O.T.; NCCIH R21AT009173 to O.T.; and the University of California, San Francisco, Research Evaluation and Allocation Committee and the J. Jacobson Fund to O.T. and D.X.
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or other funding agencies. The funding agencies did not play any role in study design or in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received May 11, 2018.
- Accepted after revision August 16, 2018.
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}