
Abstract
SUMMARY: Spontaneous intracranial hypotension is caused by spinal CSF leaks, but the site of the leak is not always detected on spinal imaging. We report on the additional value of decubitus positioning during CT myelography in enhancing the detection of subtle leaks.
ABBREVIATIONS:
- CTM
- CT myelography
- CVF
- CSF venous fistula
- SIH
- spontaneous intracranial hypotension
Spontaneous intracranial hypotension (SIH) is a condition caused by spinal CSF leaks, either into the epidural space or into an adjacent vein, known as a CSF venous fistula (CVF).1,2 Detection of CSF leakage on spinal imaging helps confirm the diagnosis and is critical to guiding treatment.3 Targeted treatment with epidural patching or surgery is important in refractory cases but requires accurate localization of a leak site.4 However, spine imaging does not demonstrate the leak site in approximately half of patients with known SIH.5,6 These cases with negative findings on imaging are thought to be due to a low-flow CSF leak or occult CVF.2
Imaging techniques that can help improve detection of occult leaks are therefore desirable. We have observed that placing a patient in the lateral decubitus position for CT myelography (CTM) facilitates the detection of CSF leaks in some patients with SIH.
Materials and Methods
Subjects
This is a retrospective series of 5 patients with SIH treated between February 2016 and February 2018 in which an etiology of CSF leak was identified on CTM performed with the patient in the lateral decubitus position. The leak was not seen on previously performed prone or supine CTM. The work in this study was approved by the Duke University Medical Center institutional review board and is compliant with the Health Insurance Portability and Accountability Act.
All subjects met International Classification of Headache Disorders, 3rd ed (https://www.ichd-3.org/) criteria for SIH. Brain MR imaging with contrast was performed before spine myelography. In all cases, subjects had undergone at least 1 myelogram with standard prone or supine positioning, which had not definitively localized a leak.
Decubitus Myelogram Technique
Decubitus CTM was performed on the basis of a subtle abnormality seen on the initial nondecubitus CTM in 4 of 5 patients. In these patients, the decubitus CTM was obtained as part of a dynamic myelogram under fluoroscopy.7 In a dynamic myelogram, intrathecal contrast is injected with the patient in the decubitus position; in these 4 patients, the abnormality seen on the initial prone CTM determined whether right or left decubitus positioning was used. The patient was not rolled before CTM to maintain a high density of dependently layering contrast material, and the CTM was performed within 10–15 minutes after fluoroscopic imaging was completed.
In the remaining patient, decubitus CTM of the spine was performed because previous prone CT myelograms had been unrevealing. In this case, bilateral decubitus scans were obtained immediately after the initial prone CTM did not show a leak.
For all myelograms (both prone and decubitus), 10 mL of iopamidol containing 300 mg/mL of iodine (Isovue-M 300; Bracco, Princeton, New Jersey) was used. All scans were performed on a single 64–detector row CT scanner (Discovery 750HD; GE Healthcare; Milwaukee, Wisconsin) using the following parameters: helical scan mode, rotation time = 0.8 seconds, pitch = 0.969, tube voltage = 120 kV(peak), automated exposure control, tube current = 300–800 mA, noise index = 19.5, slice thickness = 2.5 mm, interval = 2.5 mm, reconstruction thickness = 0.625 mm. Initial prone myelograms of the entire spine were obtained; when further interrogation of a suspected abnormality was desired, the scan was limited to the area of interest to decrease the radiation dose.
Image Analysis
The effect of decubitus positioning on the density of intrathecal contrast media was measured by placing an ROI over the thecal sac immediately adjacent to the identified leak. In cases in which a CSF venous fistula was detected, the density of the draining vein was similarly measured, as previously described.8
Results
The mean subject age was 54.2 years (range, 31–72 years). Three subjects were women. Pretreatment brain MR imaging showed evidence of SIH in all cases. Spine MR imaging was performed before myelography in 3/5 subjects and was negative for CSF leak in all cases. The mean number of CTM examinations performed before the decubitus myelogram was 1.6 (range, 1–3).
Decubitus imaging revealed a CVF in the 4 cases in which a subtle abnormality was questioned on a prior CTM (Figs 1⇓⇓–4). The fistulas in each of these 4 cases were located at the T7, T8, T10, or T11 nerve roots, respectively, all on the left. All 4 CVFs were associated with nerve root sleeve diverticula, a common association reported in other series.7 In the case in which bilateral decubitus CTM was performed, a low-flow CSF leak into the epidural space was detected at T10–11, which was not seen on the prior CTM (Fig 5).

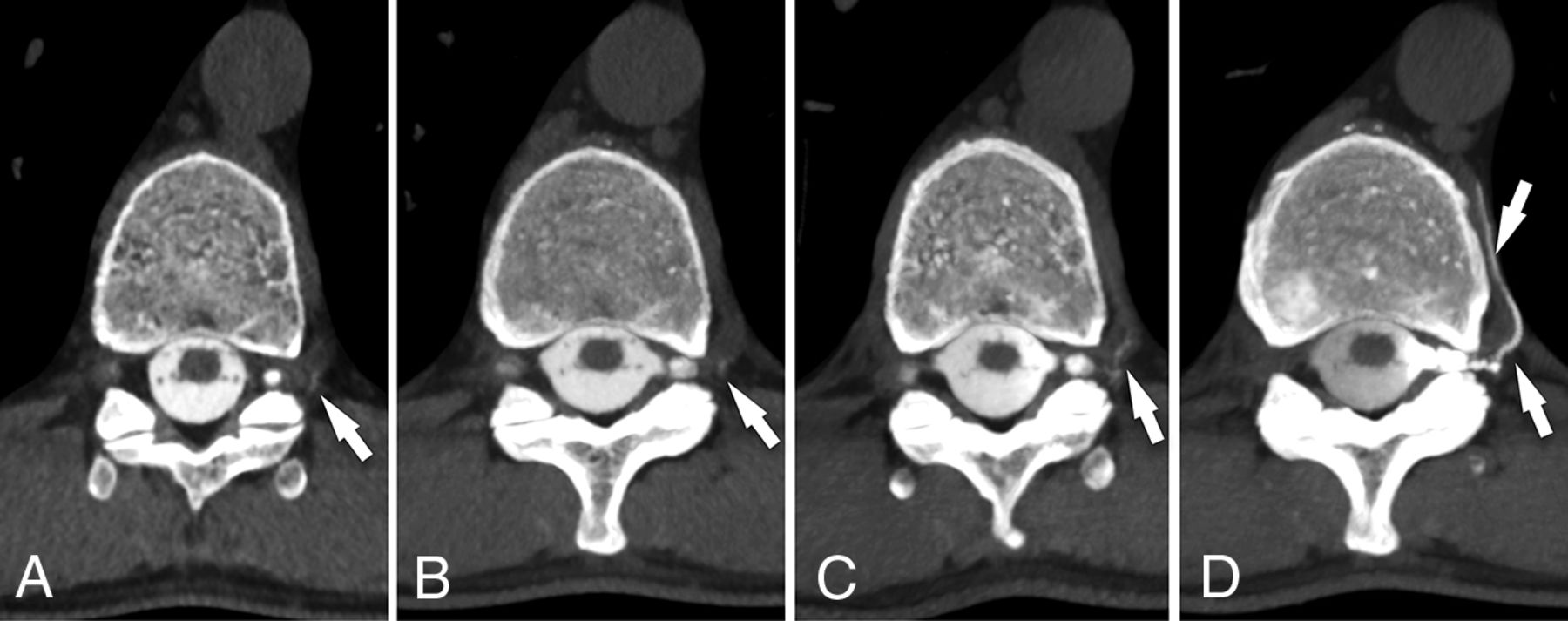
CSF venous fistula visualized best on decubitus CTM. Axial prone CTM image (A) and maximum-intensity-projection image of the same level (B) show subtle linear contrast (arrows) lateral to the T11 nerve root. The patient was turned to the left lateral decubitus position and re-scanned 13 minutes later. Axial MIP image (C) from that scan shows increased intravascular contrast with the patient in the decubitus position, suggestive of a CSF venous fistula (arrow). Axial MIP image (D) from a CTM performed after dynamic myelography on a subsequent day with the patient maintained in the decubitus position after contrast injection shows extensive filling of a paraspinal vein distal to the fistula (arrows).

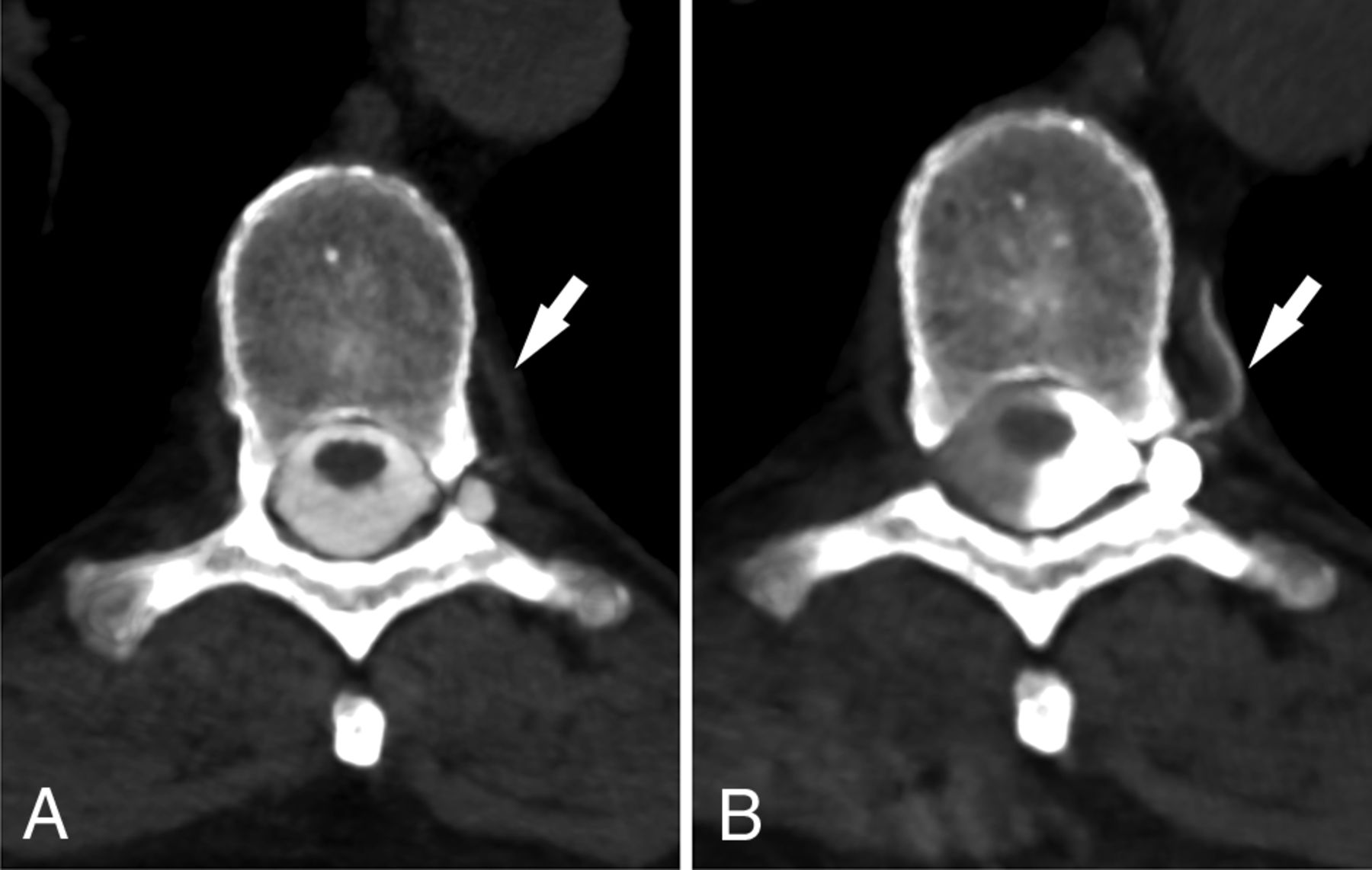
CSF venous fistula visualized best on decubitus CTM. Axial prone CT myelogram (A) shows subtle filling of a network of paraspinal veins (arrow) lateral to the nerve root and in the adjacent spinal segmental vein (arrowhead). Axial image (B) from a decubitus CTM performed after dynamic myelography on a subsequent day shows increased filling of the lateral veins (arrow) and segmental vein (arrowheads), making the CVF much more conspicuous.

CSF venous fistula visualized best on decubitus CTM. Axial prone CTM image (A) shows possible increased density of a spinal segmental vein (arrow). Axial image (B) from a decubitus CTM performed after dynamic myelography on a subsequent day shows increased filling of the segmental veins (arrow), helping to confirm the diagnosis of CVF. Note the increased density of the left lateral thecal sac due to decubitus positioning.

CSF venous fistula visualized best on decubitus CTM. Axial prone CTM image (A) shows a perineural diverticulum, but no clear leak. Axial image (B) from a subsequent CTM obtained with the patient in the decubitus position after dynamic myelography shows clear filling of a segmental vein (arrows), confirming a CVF.

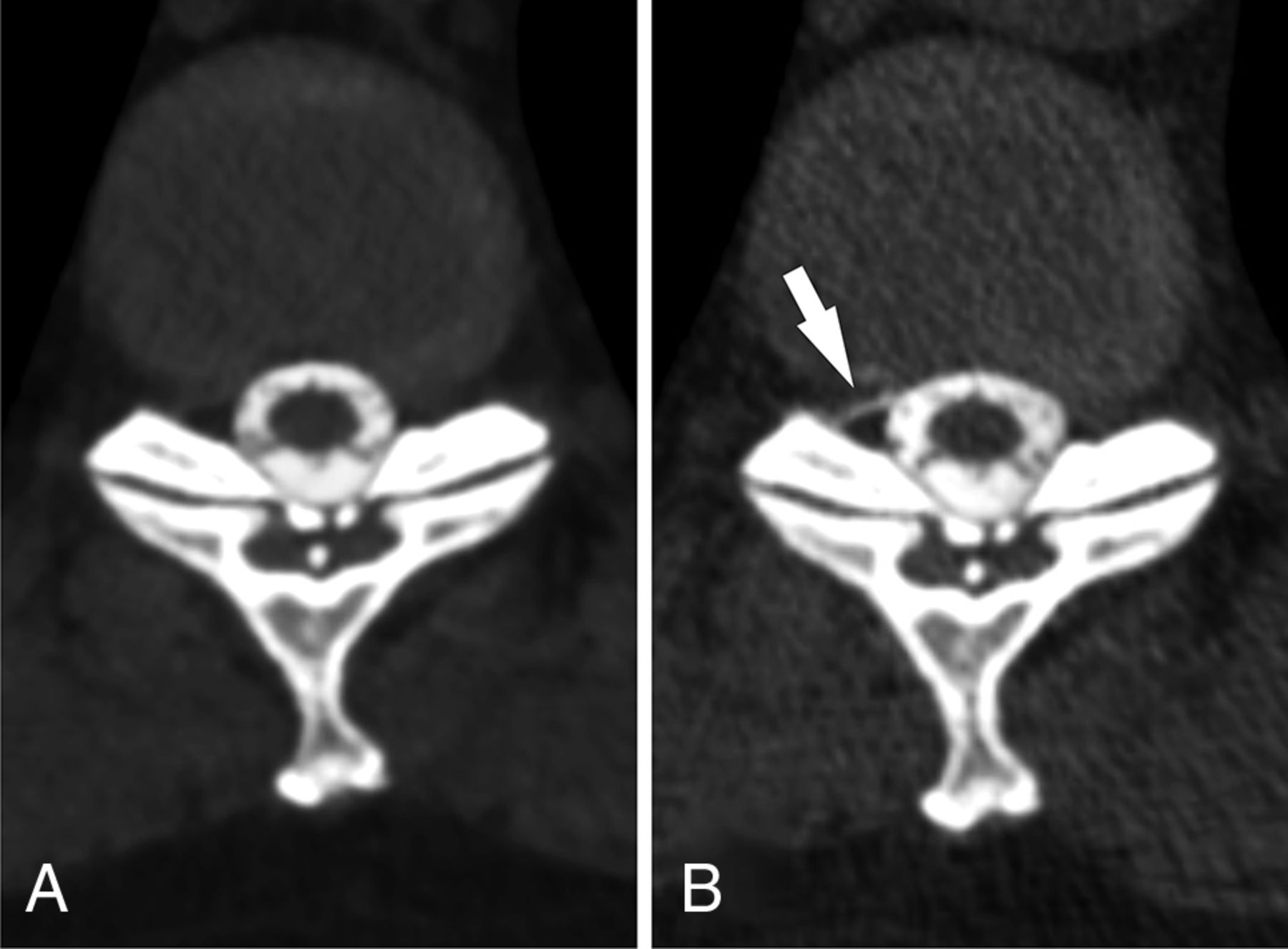
Low-flow CSF leak seen only on decubitus myelography. Axial prone CTM image (A) shows no CSF leak at the T10–11 level. The patient was turned into the left lateral decubitus position and re-scanned, again with the scan showing no leak (not shown). The patient was then turned to the right lateral decubitus position. An axial CTM image from the decubitus myelogram (B) obtained 6 minutes later shows a low-flow CSF leak not seen on prone myelogram (arrow).
On decubitus CTM, the mean density of intrathecal CSF at the leak site was 1944 HU (range 834–2960 HU), compared with 729 HU (range, 395–1253 HU) on the prior nondecubitus CTM, representing a mean increase of 301% on decubitus imaging.
For the cases of CVF, the mean density of the draining paraspinal veins on the decubitus CTM was 294 HU (range, 111–514 HU), compared with 104 HU (range, 28–288 HU) on prior nondecubitus CTM, a mean increase of 507%.
Discussion
This investigation demonstrates the additional yield of CTM performed with the patient in the lateral decubitus position in some patients with SIH when initial prone or supine CTM has not been revealing. In most patients in this series, the decision to perform decubitus imaging was prompted by an initial suspicion of a subtle abnormality on prior CTM, and decubitus myelography confirmed an abnormality at the initially suspected level in these cases. In at least 1 patient, however, decubitus CTM detected a leak that was not visible even in retrospect on prior imaging. Moreover, in the cases in which a CVF was suspected on prior CTM, the initial findings were often very subtle and decubitus myelography greatly increased diagnostic confidence. This increased confidence was a critical factor in committing the patient to surgery.7
Two factors may contribute to the increased detection of CSF leaks with the patient in the decubitus position. First, when intrathecal contrast is injected and the patient is allowed to remain in the decubitus position, the contrast concentration over the leak site is higher than if the patient is rolled. This is evident from our series, in which the mean density of the intrathecal contrast at the level of the leak increased by 301% with the patient in the decubitus position compared with the prone position.
Second, there appears to be an effect of gravity that promotes the flow of contrast through a leak or into a CVF that is on the dependent side of the thecal sac. In the patient with the low-flow leak, the contrast concentration in the thecal sac only increased slightly between the prone and decubitus scans (778 versus 835 HU), but the leak was only visible when the patient was in the decubitus position (Fig 5).
This investigation does not establish the sensitivity for decubitus CTM in leak detection because only cases positive for CSF leak were included in this initial report. Furthermore, it does not determine the overall additional diagnostic yield for decubitus CTM among all patients with SIH with initial negative findings on prone or supine CTM. Performing additional decubitus scans will necessarily increase the radiation dose; therefore, further investigation is needed to clarify when additional decubitus imaging is justified.
Conclusions
Decubitus CTM demonstrates CSF leaks not seen on conventional prone or supine CTM in some patients with SIH.
Footnotes
Disclosures: Linda Gray—UNRELATED: Board Membership: medical advisory membership for CSF Leak Association.
REFERENCES
- Received November 28, 2018.
- Accepted after revision December 22, 2018.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Density and Time Characteristics of CSF-Venous Fistulas on CT Myelography in Patients with Spontaneous Intracranial Hypotension
- Safety and Technical Performance of Bilateral Decubitus CT Myelography Using Standard versus Increased Intrathecal Iodinated Contrast Volume
- CSF-Venous Fistulas Arising Intraosseously within Bone Remodeled by Meningeal Diverticula
- Spontaneous Intracranial Hypotension in Children: A Multi-Institutional Review of Spinal CSF Leaks Localized on Advanced Myelography
- Myelographic Techniques for the Localization of CSF-Venous Fistulas: Updates in 2024
- Direct comparison of digital subtraction myelography versus CT myelography in lateral decubitus position: evaluation of diagnostic yield for cerebrospinal fluid-venous fistulas
- Diagnostic Yield of Decubitus CT Myelography for Detection of CSF-Venous Fistulas
- Temporal Characteristics of CSF-Venous Fistulas on Dynamic Decubitus CT Myelography: A Retrospective Multi-Institution Cohort Study
- Lateral Decubitus Dynamic CT Myelography with Real-Time Bolus Tracking (dCTM-BT) for Evaluation of CSF-Venous Fistulas: Diagnostic Yield Stratified by Brain Imaging Findings
- Diagnostic Performance of Decubitus Photon-Counting Detector CT Myelography for the Detection of CSF-Venous Fistulas
- A Novel Patient-Positioning Device for Dynamic CT Myelography
- Resisted Inspiration Improves Visualization of CSF-Venous Fistulas in Spontaneous Intracranial Hypotension
- Utility of Photon-Counting Detector CT Myelography for the Detection of CSF-Venous Fistulas
- Utility of Photon-Counting Detector CT Myelography for the Detection of CSF-Venous Fistulas
- Conebeam CT as an Adjunct to Digital Subtraction Myelography for Detection of CSF-Venous Fistulas
- The promise and challenges of CSF-venous fistula treatment
- Surgical Ligation of Spinal CSF-Venous Fistulas after Transvenous Embolization in Patients with Spontaneous Intracranial Hypotension
- Same-Day Bilateral Decubitus CT Myelography for Detecting CSF-Venous Fistulas in Spontaneous Intracranial Hypotension
- A Novel Endovascular Therapy for CSF Hypotension Secondary to CSF-Venous Fistulas
- Spinal Compliance Curves: Preliminary Experience with a New Tool for Evaluating Suspected CSF Venous Fistulas on CT Myelography in Patients with Spontaneous Intracranial Hypotension
- Decubitus CT Myelography for CSF-Venous Fistulas: A Procedural Approach
- Respiratory Phase Affects the Conspicuity of CSF-Venous Fistulas in Spontaneous Intracranial Hypotension
- MR Myelography for the Detection of CSF-Venous Fistulas