
Abstract
BACKGROUND AND PURPOSE: Whether architectural characteristics of ruptured brain AVMs vary across the life span is unknown. We aimed to identify angioarchitectural features associated with brain AVMs ruptured early in life.
MATERIALS AND METHODS: Patients with ruptured brain AVMs referred to 2 distinct academic centers between 2000 and 2018 were pooled and retrospectively analyzed. Imaging was retrospectively reviewed for angioarchitectural characteristics, including nidus size, location, Spetzler-Martin grade, venous drainage, and arterial or nidal aneurysm. Angioarchitecture variations across age groups were analyzed using uni- and multivariable models; then cohorts were pooled and analyzed using Kaplan-Meier and Cox models to determine factors associated with earlier rupture.
RESULTS: Among 320 included patients, 122 children (mean age, 9.8 ± 3.8 years) and 198 adults (mean age, 43.3 ± 15.7 years) were analyzed. Pediatric brain AVMs were more frequently deeply located (56.3% versus 21.2%, P < .001), with a larger nidus (24.2 versus 18.9 mm, P = .002), were less frequently nidal (15.9% versus 23.5%, P = .03) and arterial aneurysms (2.7% versus 17.9%, P < .001), and had similar drainage patterns or Spetzler-Martin grades. In the fully adjusted Cox model, supratentorial, deep brain AVM locations (adjusted relative risk, 1.19; 95% CI, 1.01–1.41; P = .03 and adjusted relative risk, 1.43; 95% CI, 1.22–1.67; P < .001, respectively) and exclusively deep venous drainage (adjusted relative risk, 1.46, 95% CI, 1.21–1.76; P < .001) were associated with earlier rupture, whereas arterial or nidal aneurysms were associated with rupture later in life.
CONCLUSIONS: The angioarchitecture of ruptured brain AVMs significantly varies across the life span. These distinct features may help to guide treatment decisions for patients with unruptured AVMs.
ABBREVIATION:
- HR
- hazard ratio
The most devastating complication of brain AVMs is their rupture, leading to intracranial hemorrhage,1 responsible for considerable morbidity and mortality. The management of patients with unruptured brain AVMs relies on the evaluation of the risk-benefit balance between invasive treatment and follow-up. The optimal approach is yet to be determined in pediatric patients,2 in whom decisions are made more complex by the potential long life span and cumulative risk of rupture. Previous data have shown that brain AVM angioarchitecture evolves across time.3,4 On the basis of the common model of “wear and tear,” brain AVMs are believed to rupture in sectors with more severe arterial and venous vasculopathies and increased frailty features, more frequently seen in adults than during childhood. Nonetheless, intracranial hemorrhage remains the most common revelation in children, and brain AVMs represent the leading etiology of intracranial hemorrhage in the pediatric group; thus, the identification of individual biomarkers associated with impending or higher risk of rupture is of crucial importance to guide therapeutic management. Several angioarchitectural brain AVM characteristics (deep location, exclusive deep venous drainage, associated aneurysms, or venous ectasia)5-7 have been identified as being more prevalent in ruptured than in unruptured brain AVMs, but these data are derived mostly from adult samples and remain scarce in pediatric populations.1,8 Furthermore, such findings do not formally allow identifying characteristics associated with earlier rupture, due to the great risk of recognition biases (eg, the higher prevalence of a biomarker in the ruptured population does not indicate that this biomarker is responsible for a rupture earlier in life).
In this retrospective multicentric cohort of children and adult patients with first brain AVM rupture, we aimed to determine brain AVM angioarchitectural characteristics associated with rupture early in life.
MATERIALS AND METHODS
Pediatric Cohort
Pediatric patients with nontraumatic intracranial hemorrhage referred to a pediatric quaternary care center (Necker-Enfants Malades University Hospital), the coordinating center for the French Pediatric Stroke Network, are prospectively collected into an inception retrospective (2003–2008) and prospective (2008–ongoing) registry, described in detail elsewhere.9,10 This registry was retrospectively queried to identify children with first ruptured brain AVMs. Patients meeting the following criteria were retrospectively screened for inclusion: 1) 28 days to 18 years of age at the time of symptom onset; 2) having nontraumatic intracerebral, intraparenchymal, or intraventricular hemorrhage; and 3) having a ruptured brain AVM.
Adult Cohort
Records of adult patients with brain AVMs referred to a distinct tertiary care center (Pitié-Salpêtrière University Hospital) between January 1, 2003, and February 1, 2018, as described in detail elsewhere,11 were retrospectively reviewed. Adult patients with ruptured brain AVMs, naive to any previous targeted treatment, were retrospectively screened for inclusion.
Data Acquisition
Clinical, demographic, and imaging data (brain 1.5T MR imaging, brain CT, cerebral conventional angiography) were retrospectively assessed. Data included age at presentation, sex, admission Glasgow Coma Scale score, hemorrhage location and volume (AxBxC/2 method12), as well as brain AVM angioarchitectural features (nidus size; maximal 2D diameter; location; Spetzler-Martin grade;13 venous drainage pattern as deep, superficial, or mixed; and nidal or arterial aneurysm). Per guidelines, we assessed the presence of deep venous drainage if the internal cerebral veins, basal veins, or precentral cerebral vein participated in the nidus venous drainage.14 All data were acquired in consensus by a distinct pair of interventional neuroradiologists (1 senior and 1 junior) in each cohort.
Ethics
All aspects of the study were in accordance with the General Data Protection Regulation and actual French law and ethics in health-related research. Institutional review board approval was obtained under the reference of Comité de Protection des Personnes Ile de France 3, 18062012. As in all observational studies with retrospective analysis of routinely acquired data, written informed consent was waived, and patients or children’s parents could oppose the use of their health-related data. The article was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement.15
Statistics
Continuous variables were expressed as mean ± SD or median (interquartile range) as appropriate. Categoric variables were expressed as absolute numbers with percentages. We compared variable differences between the adult and pediatric cohort (using 18 years of age as a cutoff) univariable analyses with the t test, Mann-Whitney U test, χ2 test, and multivariate analysis of variance as appropriate. Variables associated with the pediatric cohort in univariable analyses at P < .1 were entered into a multivariable nominal logistic regression model; then, a backward elimination was used to eliminate nonsignificant variables. Considering age at presentation as a continuous variable, used as the time to rupture, we performed survival analyses. Data were not censored because birth was the chosen initiation of time to the event and intracranial hemorrhage presentation was the event. We first ran Kaplan-Meier analyses with significance testing with the log-rank test to determine univariate predictors of early rupture. Then we conducted univariable Cox proportional hazards analysis to calculate the unadjusted hazard ration (HR) for the risk of rupture. Variables with P < .1 in univariable Cox analysis were included in multivariable Cox proportional hazards models to determine adjusted HRs of early rupture. Two-sided P values < .05 were considered statistically significant. All statistical analyses were performed using JMP Pro 14.0 (SAS Institute).
RESULTS
Patient Population and Baseline Characteristics
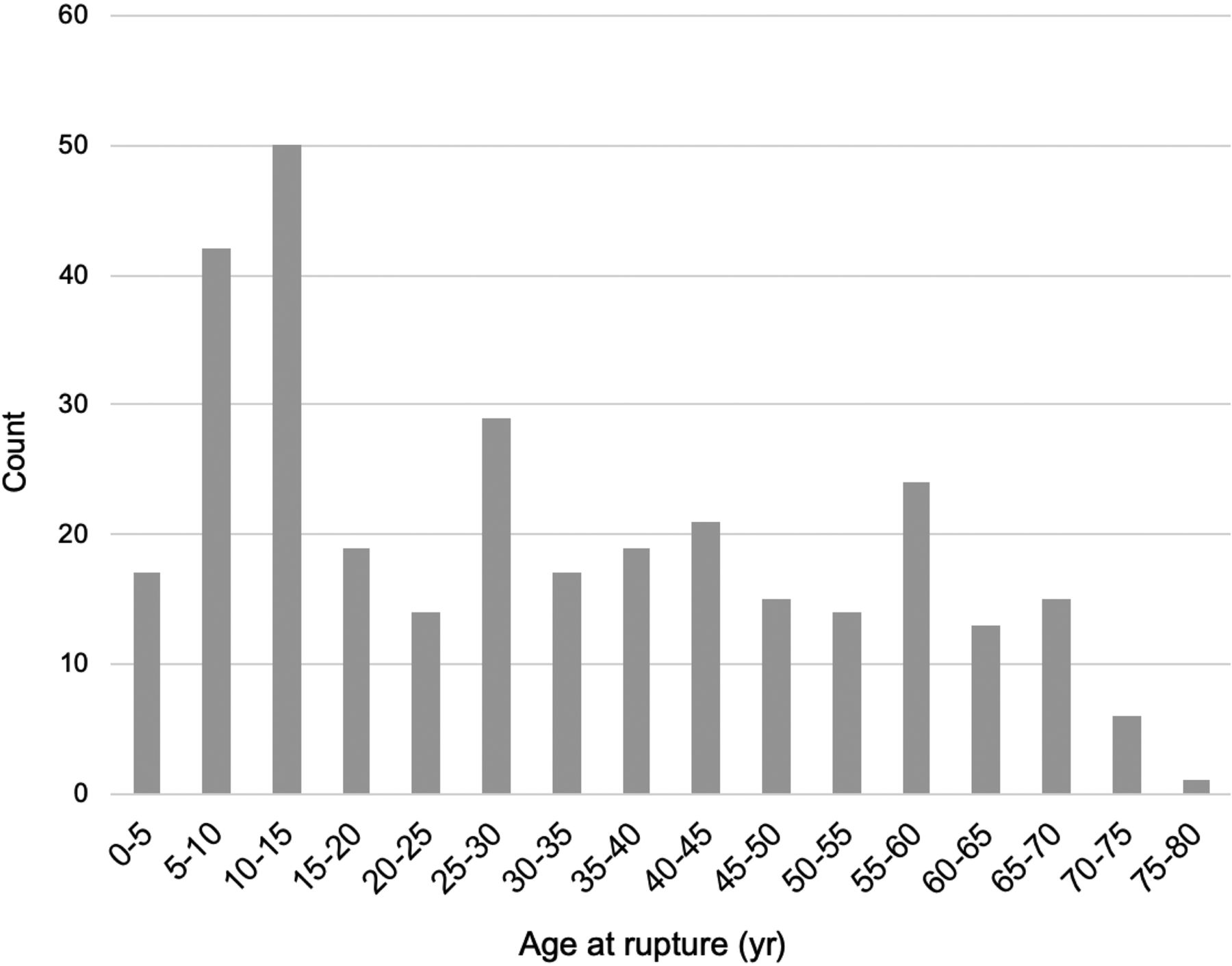
A total of 122 children (mean, 9.8 ± 3.8 years of age) and 198 adult patients (mean, 43.3 ± 15.7 years of age) were included in the analysis. There was no difference regarding the female proportion (45.9% versus 42.9%, P = .62) or baseline Glasgow Coma Scale score between children and adults, respectively (11.6 ± 3.9 versus 12.4 ± 3.7, P = .09) (Table 1). Age distribution at rupture is presented in Fig 1.

Age distribution at rupture in the study sample.
Baseline clinical and imaging characteristicsa
Hemorrhages were most commonly supratentorial, with no difference among cohorts (76.7% versus 72.7%, P = .45). Intracranial hemorrhage volumes were significantly larger in adults than in children (19.8 ± 16.7 versus 38.6 ± 35.5 mL, P < .001).
AVM Characteristics
Pediatric-to-Adult Comparisons.
In univariate analyses, brain AVMs in the pediatric group were more frequently deeply located (56.3% versus 21.2%, P < .001) and larger (24.2 ± 14.3 versus 18.9 ± 14.3 mm, P = .002) with less frequent nidal (15.9% versus 23.5%, P = .03) and prenidal arterial aneurysms (2.7% versus 17.9%, P < .001). There was no significant difference in venous drainage patterns, Spetzler-Martin grade, and nidus location.
After we adjusted for sex, nidus size, pre- or nidal arterial aneurysm presence, and supratentorial location, the nidus size (adjusted OR, 0.95 per millimeter increase; 95% CI, 0.93–0.97; P < .001), prenidal aneurysms (adjusted OR, 28.9; 95% CI, 5.6–148; P < .001), and nidal aneurysms (adjusted OR, 2.6; 95% CI, 1.1–5.3; P = .006) showed a significant association with rupture during adulthood. When we forced adjustment for the venous drainage pattern in the same model, deep venous drainage appeared as a risk factor for rupture during childhood (adjusted OR, 0.55; 95% CI, 0.30–0.99; P = .04).
Birth-to-Rupture Survival Analyses.
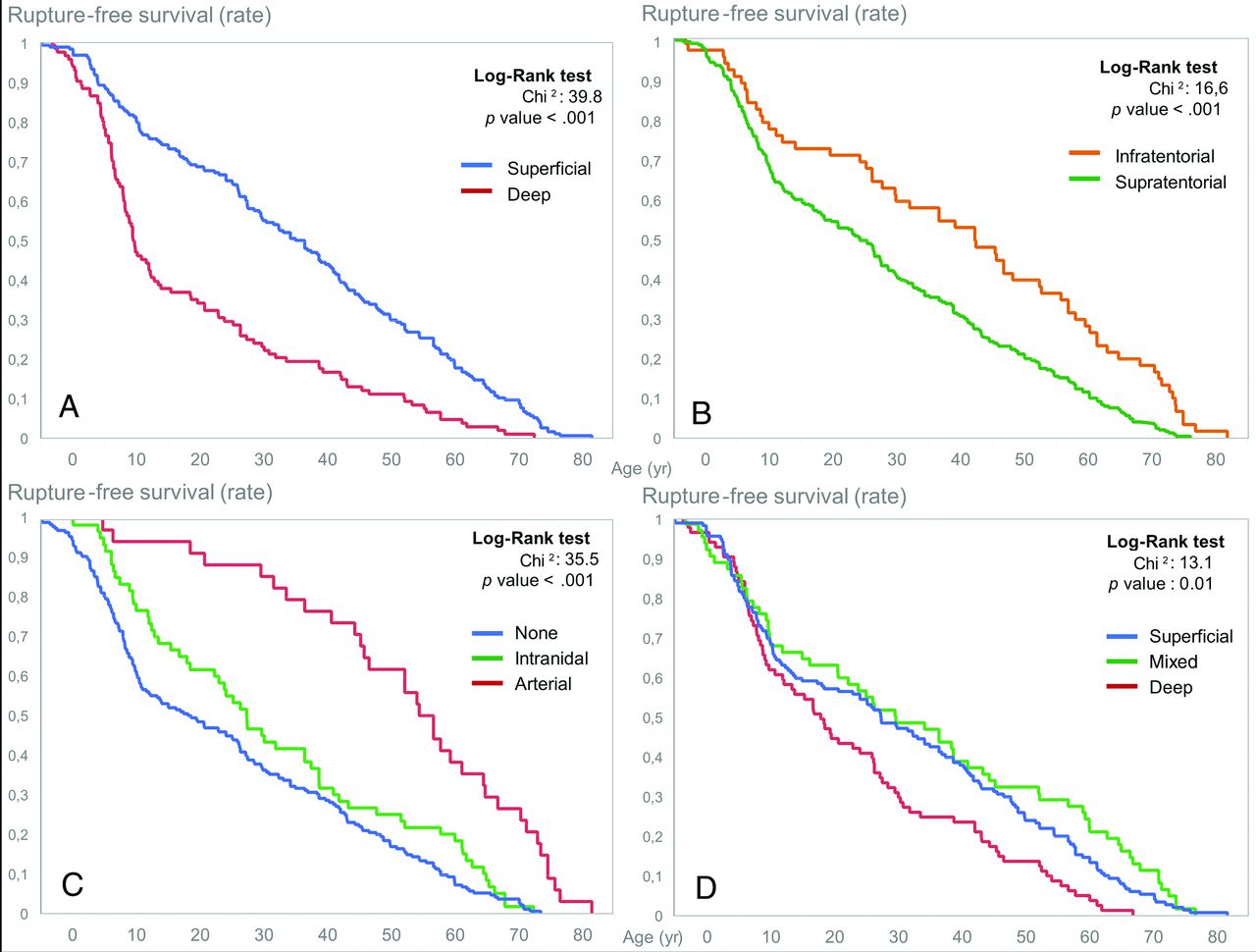
In univariate survival analysis, AVM supratentorial location, deep location, and exclusively deep venous drainage were associated with earlier rupture (log-rank, P < .05 for all), whereas nidal or prenidal arterial aneurysms were associated with later rupture (log-rank, P < .001) (Fig 2). There was no rupture-free survival difference based on the presence of any deep venous drainage (log-rank, P = .61).

Rupture-free survival according to brain AVM characteristics, Kaplan-Meier survival curves, delay until rupture (age in years), and brain AVM location (A and B), aneurysm presence (C), and venous drainage pattern (D).
Similar predictors were found in univariable Cox regression, and the fully adjusted proportional model found AVM supratentorial and deep locations (HR, 1.19; 95% CI, 1.01–1.41; P = .03 and HR, 1.43; 95% CI, 1.22–1.67; P < .001, respectively) and the absence of an aneurysm (HR, 0.62; 95% CI, 0.46–0.83; P < .001) to be associated with earlier rupture (Table 2).
Uni- and multivariable proportional hazards for time to rupture
In the above-mentioned model, when we removed deep location to avoid confounding on the venous pattern, an exclusive deep venous drainage became a strong predictor of earlier rupture (adjusted relative risk, 1.46; 95% CI, 1.21–1.76; P < .001).
DISCUSSION
We found that supratentorial and deep locations and exclusive deep venous drainage were more frequently seen in pediatric than in adult ruptured brain AVMs and that these features were associated more generally with rupture earlier in life. We also found that nidal or afferent arterial aneurysms were more prevalent in brain AVMs that rupture later in the life span.
These results contribute to the evidence that various morphologic brain AVM characteristics are associated with brain AVM rupture at initial diagnosis. By inference, variables such as AVM size, deep venous drainage pattern, and associated arterial aneurysms have been considered “risk factors” for brain AVM hemorrhage in general.4,5,16⇓-18 Here, we extend knowledge by characterizing patterns associated with rupture across the life span, that is, factors that influence or are seen at earlier or later rupture.
Age group is long known to strongly influence the presentation of brain AVMs,2 and it has been shown that brain AVMs in children disproportionately present with intracranial hemorrhage compared with adults. This finding has led to the common belief that children are at higher risk for brain AVM rupture. Yet, the higher rates of hemorrhages in children with brain AVMs is debated because they may result from confounding by presentation. In other words, the higher rate of hemorrhage in children may only result from children having fewer reasons to undergo brain imaging and have a fortuitous (or near-fortuitous, for instance in headaches) discovery of their brain AVM, in turn raising the proportion of brain AVMs discovered after a rupture. This has been shown to be true even after correcting for a potential informative censoring (ie, the higher rate of preventive treatment in nonhemorrhagic pediatric brain AVMs).2 Other authors, alternatively, believe that the difference in hemorrhagic rates may be the result of biologic differences leading to more aggressive/frail brain AVMs that rupture early in children.
Among angioarchitectural characteristics of brain AVMs reported to be associated with rupture at presentation,1,6,8,18⇓⇓-21 smaller nidus size was long considered a major rupture risk factor in brain AVM natural history.22⇓-24 This could be interpreted as a contradiction to our finding because early rupture was associated with larger nidus size. However, in the absence of a control group comprising patients with unruptured brain AVMs, we cannot conclude about the absolute or relative risk of rupture but only infer from survival models that among patients who will experience a rupture, larger brain AVMs are likely to rupture earlier. Furthermore, larger nidi are more likely to become symptomatic in the absence of bleeding than smaller ones, with a higher risk for causing epilepsy or headaches, conditions for which children may be less likely to get brain imaging than adults; this feature may, in turn, explain the over-representation of smaller brain AVMs in previously reported samples of ruptured (versus unruptured) lesions. Furthermore, larger AVMs may uniquely express a hemodynamic or biologic feature that promotes early rupture, but the particular feature may be expressed at a low frequency, yielding to the alternate hypothesis that the risk of rupture may be generally lower for large AVMs, but when larger AVMs rupture, it happens earlier in life.
Recognition bias from previously published works may also explain our finding that supratentorial (rather than infratentorial) location was associated with earlier rupture, challenging the results of Ellis et al6 and Oulasvirta et al,8 who observed the opposite. These seemingly contradictory results likely reflect infratentorial brain AVMs only coming to clinical attention after a rupture, while supratentorial lesions may present with other symptoms. Our results, in that sense, add key additional data by establishing that among brain AVMs that first present with hemorrhage, both supratentorial location and larger AVMs are associated with earlier rupture.
We found arterial and intranidal aneurysms to be associated with rupture later in life. In previous studies, Hetts et al1 and Stapf et al25 found that aneurysms were significantly associated with later AVM diagnosis, and several converging reports indicate that arterial and nidal aneurysms are more common in older individuals and disproportionately more so in late hemorrhagic presentations.1,2,6,26 These data as well as our results indicate that these frailty features develop later in life, possibly due to chronic hemodynamic stress,27 mandate life-long follow-up to detect their appearance, and potentially indicate impending or higher risk of bleeding.18 Our results in that sense reinforce the assertion that aneurysms (whether arterial or nidal) are manifestations of wear and tear of AVMs forming through a cumulative damage processes and are, therefore, expected to be acquired across time and be expressed more frequently in older patients with AVMs.
The main limitations include the retrospective nature of our study and our results being derived from 2 distinct populations, when it is known that brain AVM characteristics may be heterogeneous across settings.28 We believe this feature to be a very unlikely source of confusion, given the geographic proximity of both including centers (3 kilometers) and the potential population pool differing only in age.
CONCLUSIONS
In this large sample of pediatric and adult patients with ruptured brain AVMs, we demonstrated significantly different architectural features according to age at rupture and showed that earlier rupture was associated with deep, supratentorial brain AVMs with exclusively deep venous drainage, whereas aneurysms (nidal or arterial) were associated with later rupture. Whether these differences reflect biases versus biologic differences in the natural history of brain AVMs along the life span deserves further study.
Footnotes
Disclosures: Nader Sourour—UNRELATED: Consultancy: Medtronic, Balt, MicroVention. Frederic Clarençon—UNRELATED: Board Membership: ArteDrone; Payment for Lectures Including Service on Speakers Bureaus: Penumbra, Stryker, Balt, MicroVention.
Paper previously presented at: French Days of Radiology, October 11–14, 2019; Paris, France.
References
- Received June 19, 2020.
- Accepted after revision August 6, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.