
Article Figures & Data
Figures
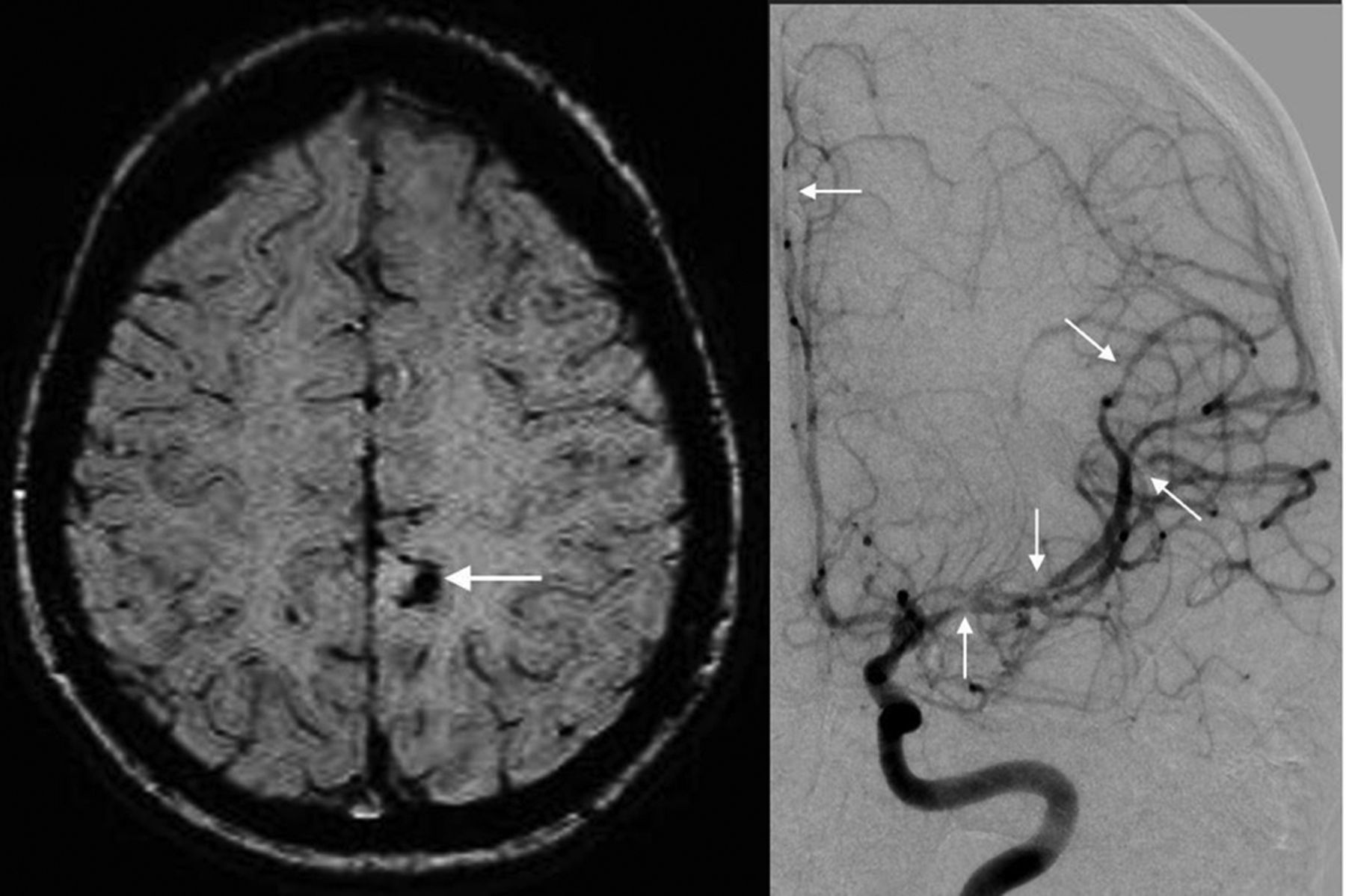
- Fig 1.
Reversible cerebral vasoconstriction syndrome in a 21-year-old woman with a thunderclap headache, who thereafter became encephalopathic. SWI (A) shows a small hemorrhage (arrow). Catheter DSA via the left ICA (B) demonstrates multifocal areas of narrowing of the anterior cerebral artery and MCA segments (arrows).
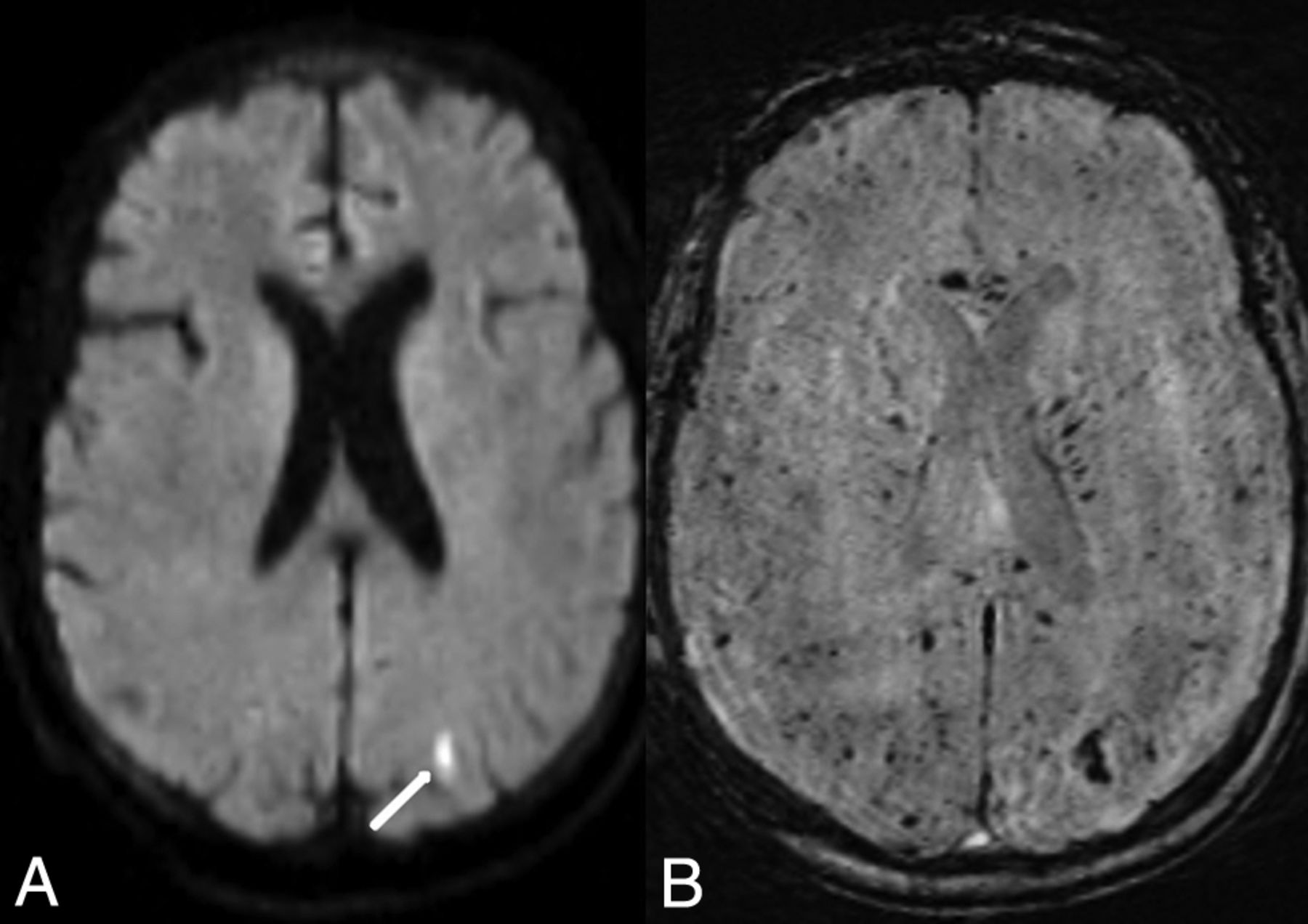
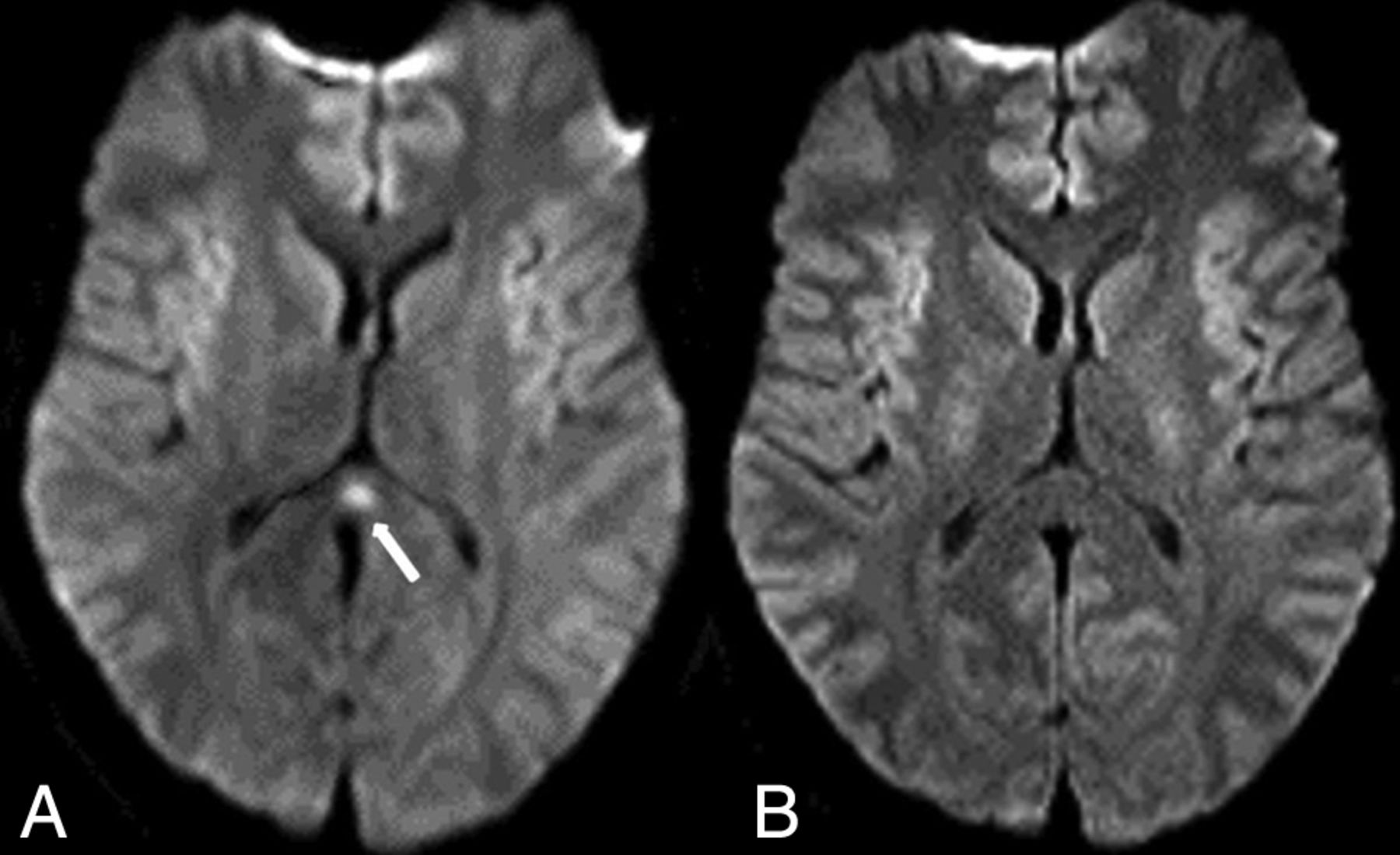
- Fig 2.
Transient global amnesia in a 60-year-old woman with a sudden onset of amnesia who had a punctate (2 mm) abnormality in the left hippocampus (arrow) on DWI (A), with corresponding hypointensity (arrow) on SWI (B). The symptoms and the punctate focus were resolved 2 days later, as noted on DWI (C).
- Fig 3.
Thrombotic microangiopathy in a 66-year-old woman with severe thrombocytopenia from chronic lymphocytic leukemia who presented with altered mentation. The initial MR imaging findings were negative (not shown). Ten days later, a punctate focus of reduced diffusion (arrow) was noted in the left posterior occipital lobe on DWI (A) with innumerable punctate foci on SWI related to TMA (B); however; there were no abnormalities on FLAIR or postcontrast T1WI (not shown). The symptoms resolved 3 days later.
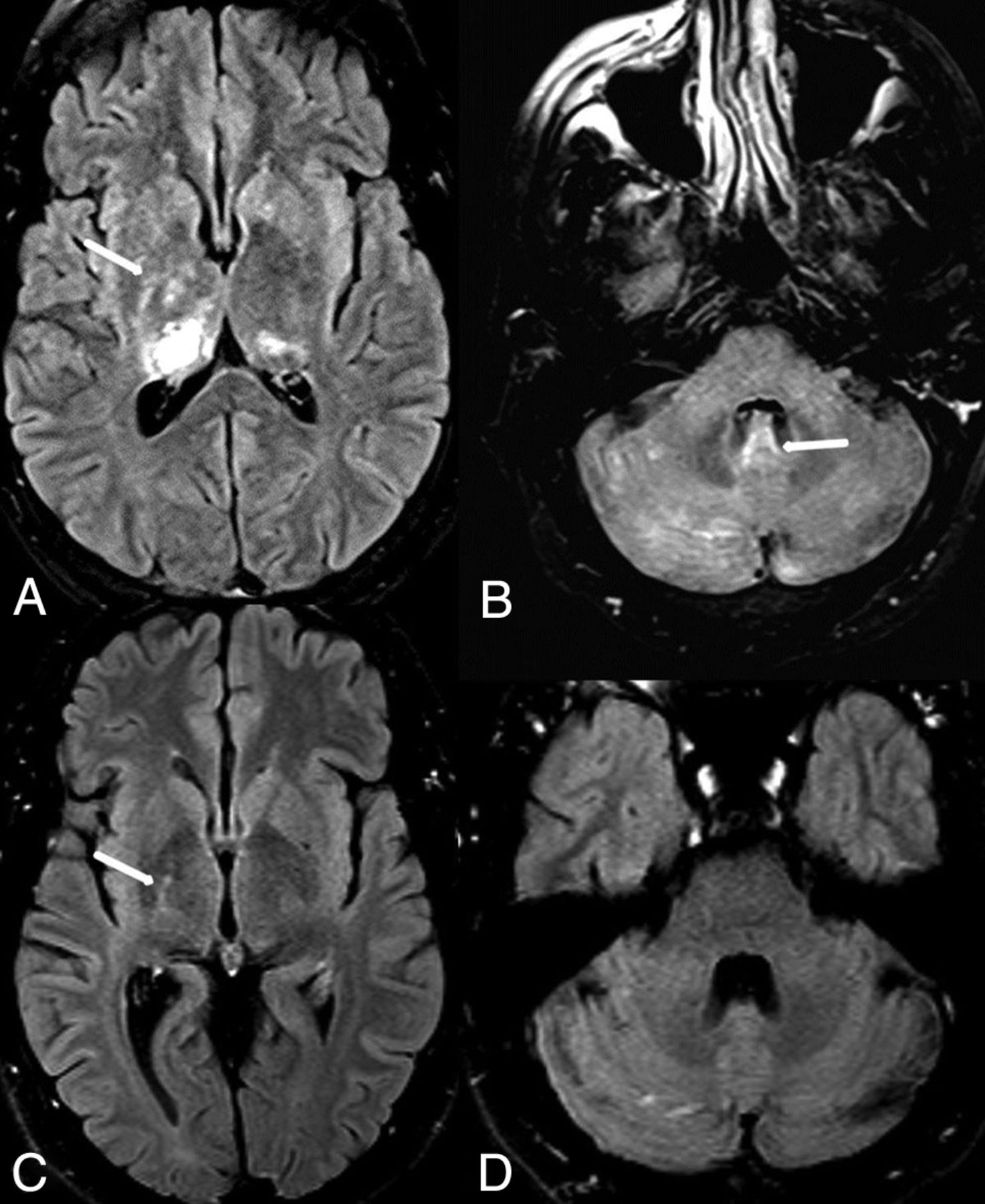
- Fig 4.
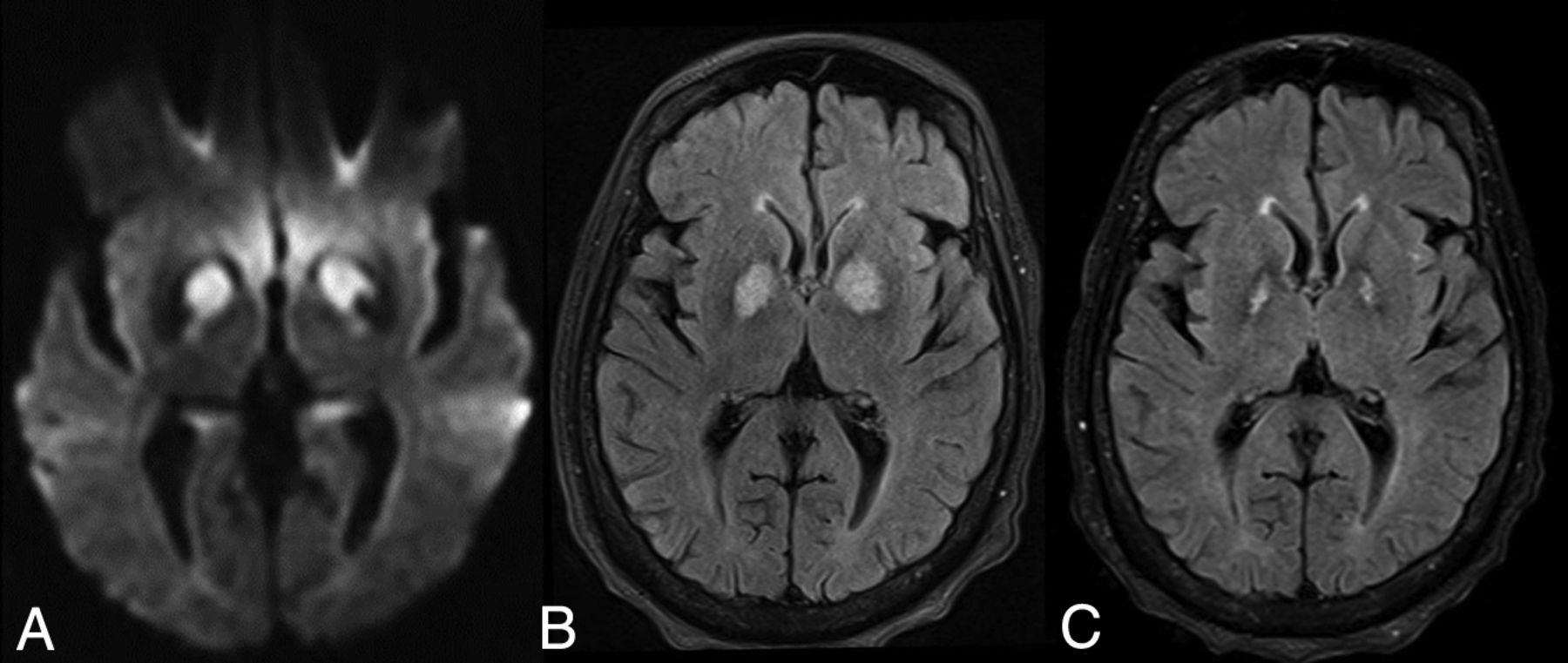
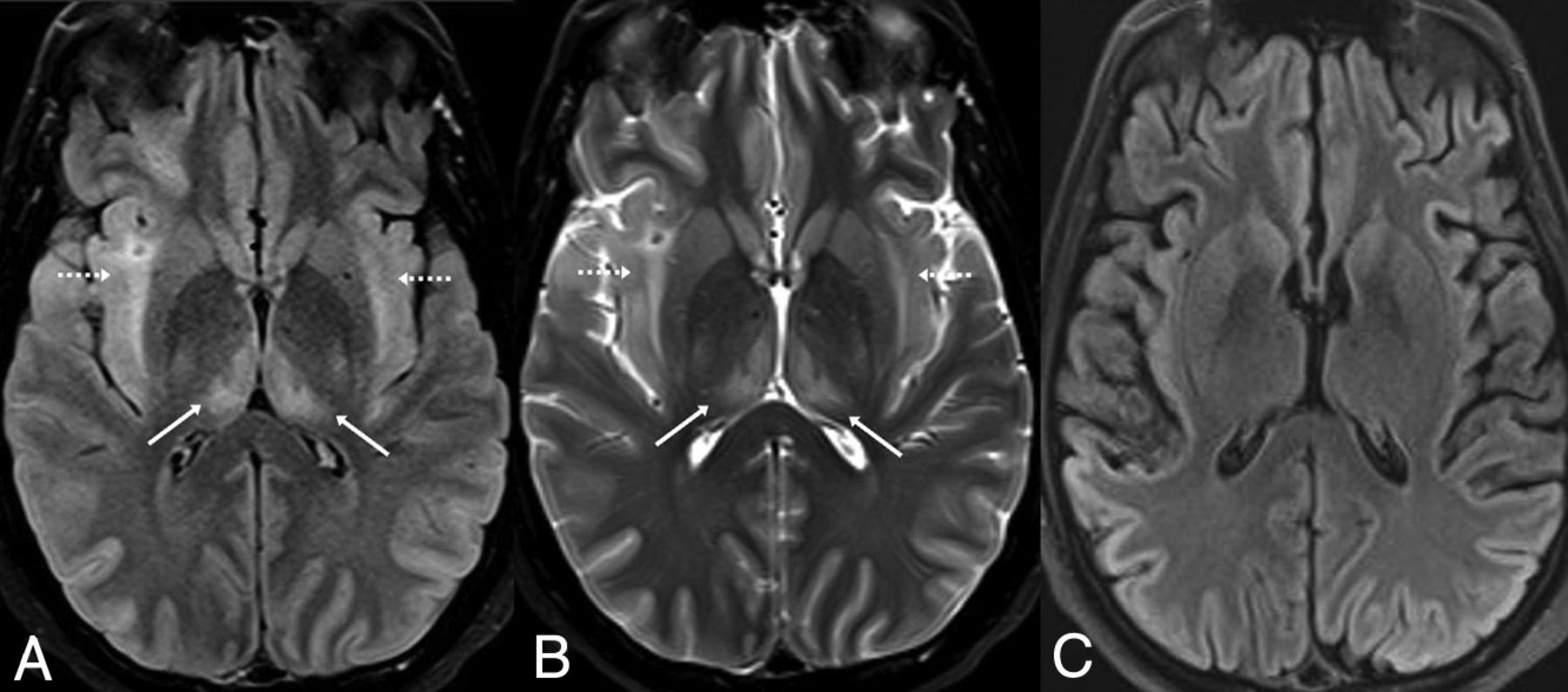
Powassan viral encephalitis in a 43-year-old man with altered mentation, who had negative blood cultures for bacteremia, but positive immunoglobulin M for Powassan virus. On FLAIR (A), hemorrhages are noted of the thalami, right greater than left, also with right basal ganglia hyperintensity (arrow). Innumerable tiny foci are noted on FLAIR (B) within the cerebellar hemispheres and of the cerebellar vermis (arrow). Five months later, the symptoms and abnormal signal were almost resolved, as demonstrated on follow-up FLAIR (C and D). There was only mild residual signal in the posterior limb of right internal capsule (C, arrow).
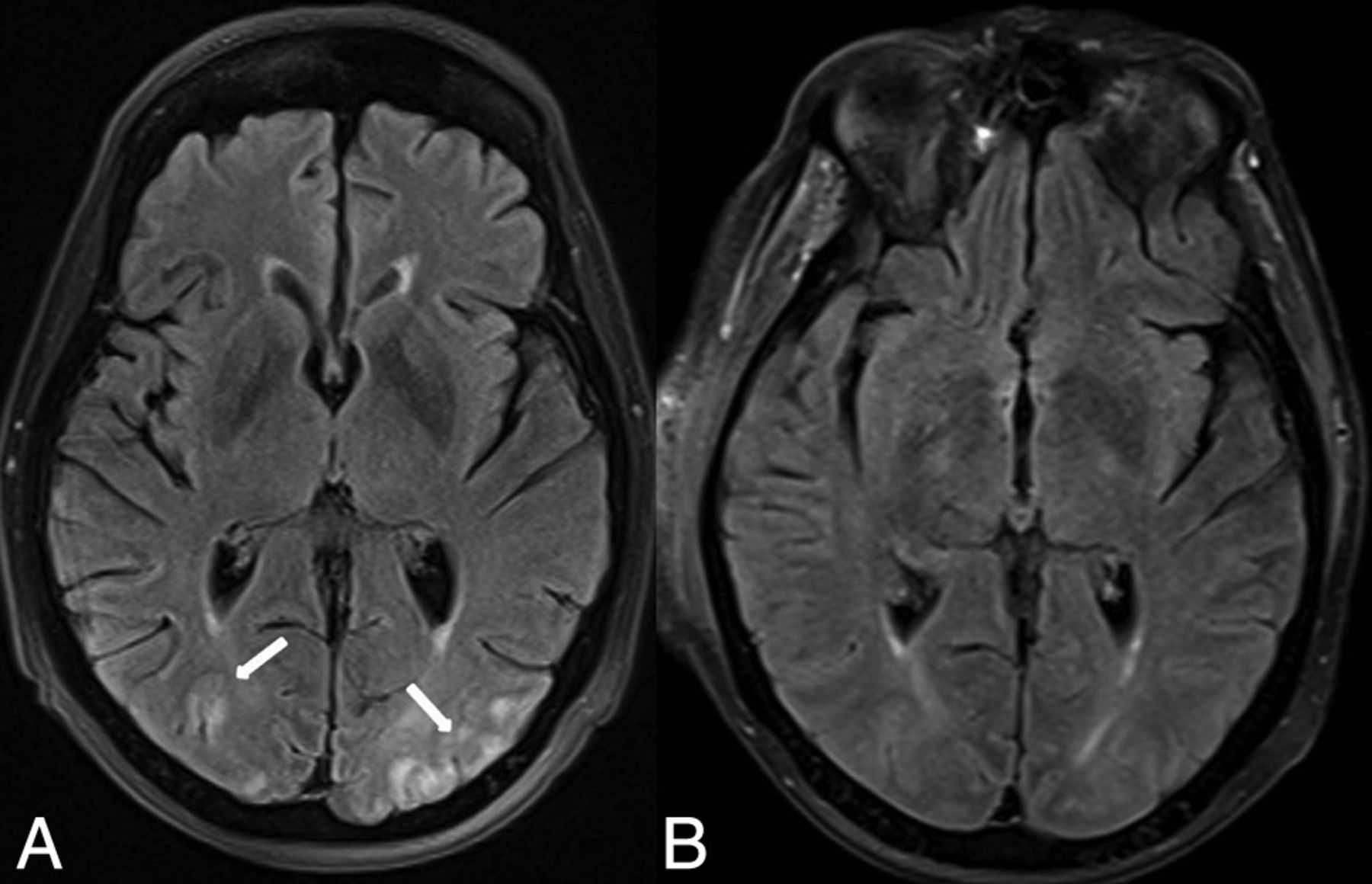
- Fig 5.
PRES in a 72-year-old woman with esophageal cancer, treated with cisplatin, 5-fluorourocil, and radiation therapy. The patient presented with altered mental status. On FLAIR (A), there are cortical/subcortical posterior occipital abnormalities typical of mild PRES (arrows). The symptoms and FLAIR MR imaging findings resolved 1.5 months later (B).
- Fig 6.
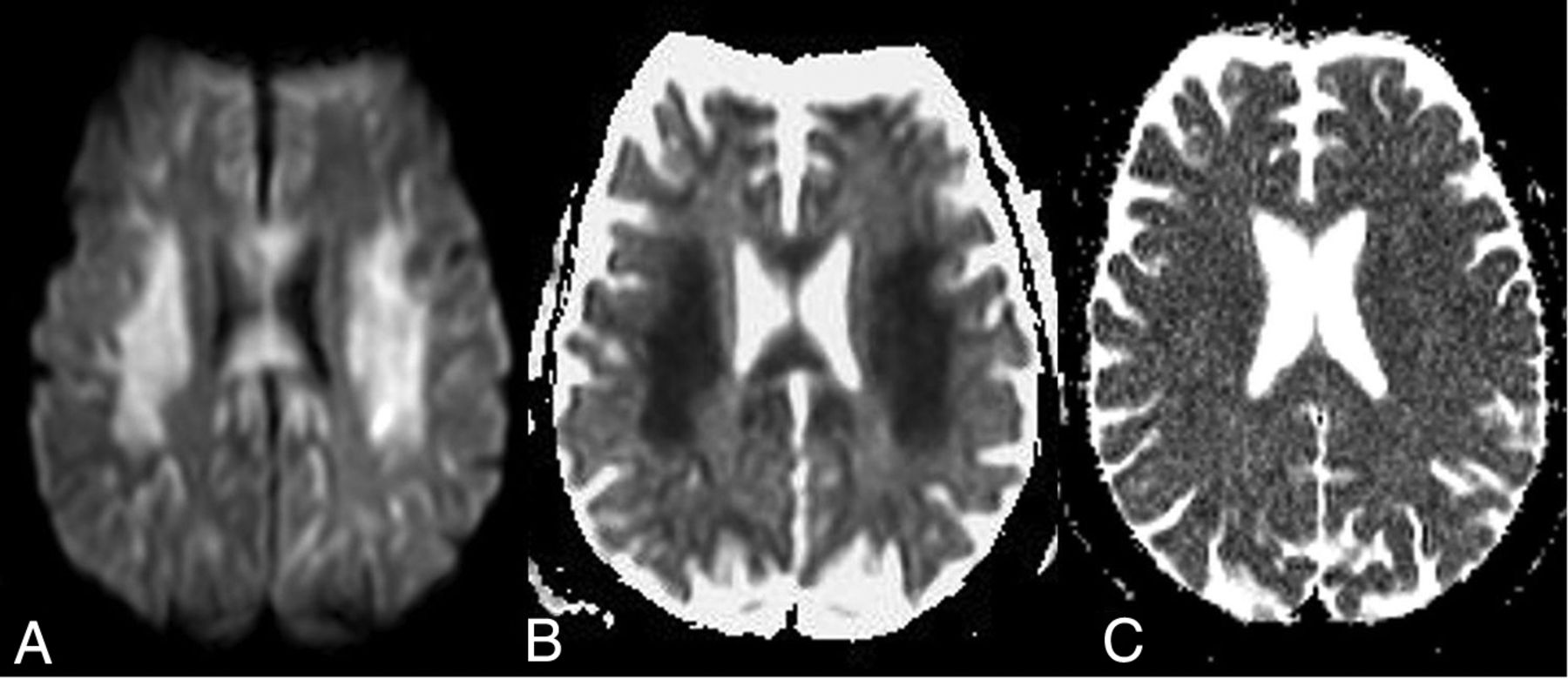
Acute toxic leukoencephalopathy in a 57-year-old man receiving 5-fluorourocil for esophageal cancer who presented with altered mental status 5 days before the initial MR imaging. On that MR imaging, there was symmetric bilateral reduced diffusion of the PVWM on DWI (A) and an ADC map (B). Nineteen days later, the symptoms and MR imaging findings had nearly resolved, as demonstrated on an ADC map (C).
- Fig 7.
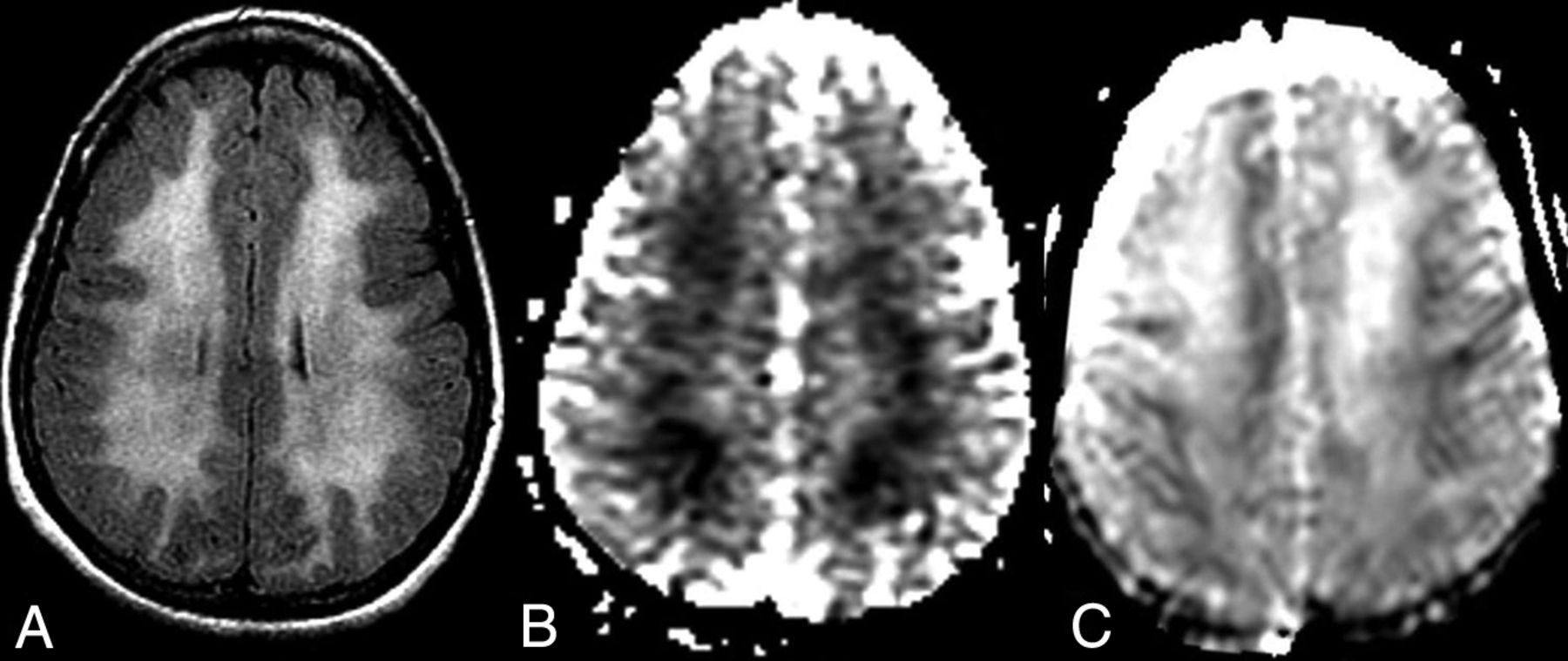
Opioid-related acute toxic encephalopathy in a 44-year-old woman with “chasing the dragon” from opioid inhalation who was found unresponsive. On FLAIR (A), there is a symmetric PVWM abnormality bilaterally, with corresponding reduced diffusion on an ADC map (B). Ten days later, the MR imaging demonstrated T2 shine through on the ADC map, with corresponding slowly improving mentation clinically (C).
- Fig 8.
CO toxicity in a confused 28-year-old man found obtunded above a garage, having elevated serum CO levels. As is typical of CO toxicity, reduced diffusion and hyperintense signal were noted within the bilateral globi pallidi on DWI (A) and FLAIR (B), respectively. One year later, atrophy of the globi pallidi was present on FLAIR (C).
- Fig 9.
Wernicke encephalopathy in a 47-year-old woman with altered mentation, who was not seen for several days, having been found unresponsive in her apartment. Reduced diffusion was noted of the mamillary bodies (arrow) and periaqueductal region (dotted arrow) on DWI (A), with thalamic abnormalities (arrows) on FLAIR (B). The symptoms and DWI findings resolved 1 week later (C).
- Fig 10.
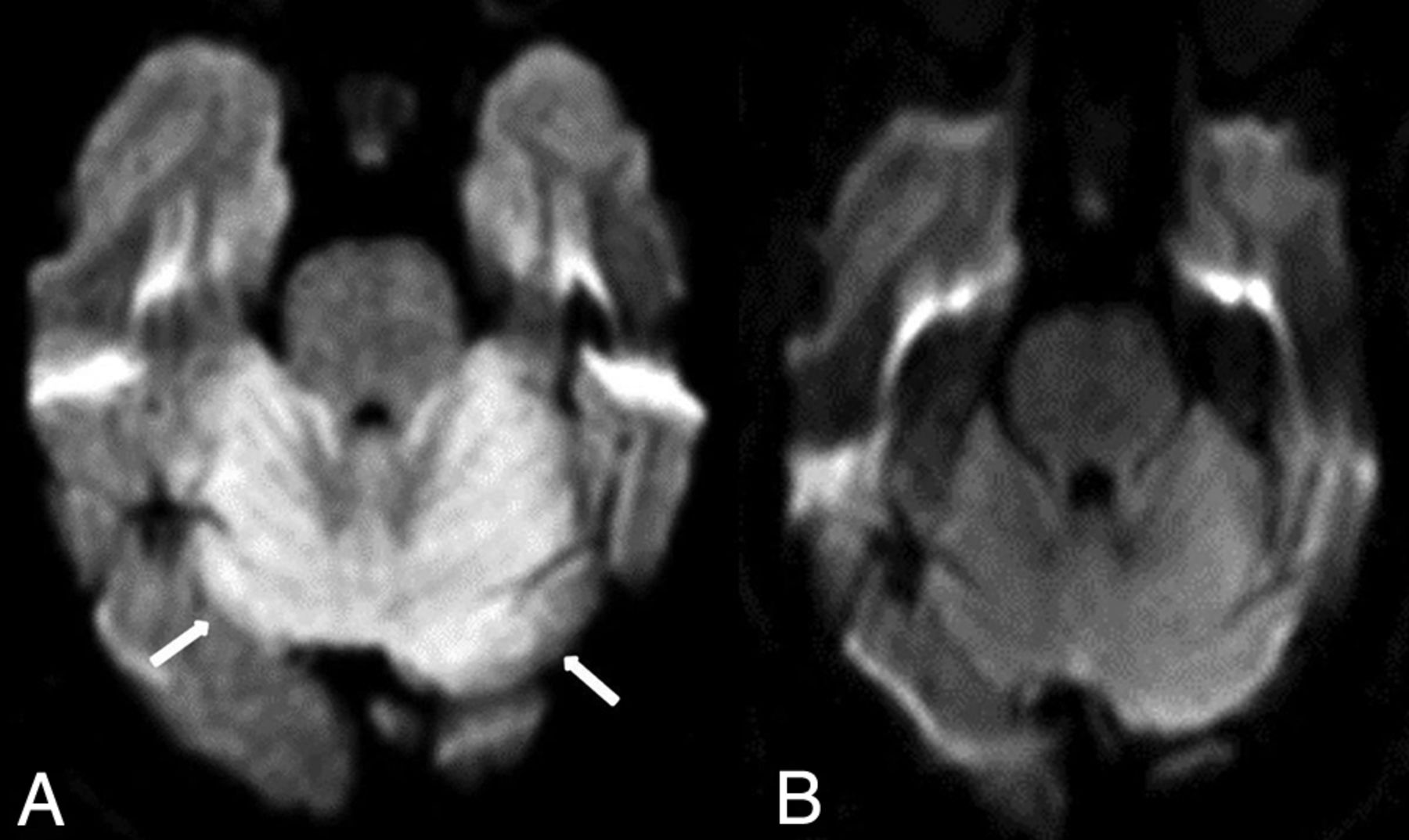
REACT syndrome in a 53-year-old woman with encephalopathy on 5-fluorouracil who had reduced diffusion within the cerebellum on diffusion-weighted MR imaging (A, arrows). This resolved 12 days later on DWI (B).
- Fig 11.
Reversible splenial lesion in a 35-year-old man on antiepileptic medications for seizures who presented with mildly altered mental status, having a lesion on DWI (A, arrow). The symptoms and DWI findings had completely resolved in 5 days (B).
- Fig 12.
Sertraline overdose in a 22-year-old man with T2 shine through in the insula (A, dotted arrows) and bilateral internal capsules on DWI (A, arrows), with high signal of the subcortical and deep temporo-parietal WM on FLAIR (B, arrows). Five days later, the MR imaging findings had resolved, as noted on DWI (C) and FLAIR (D).
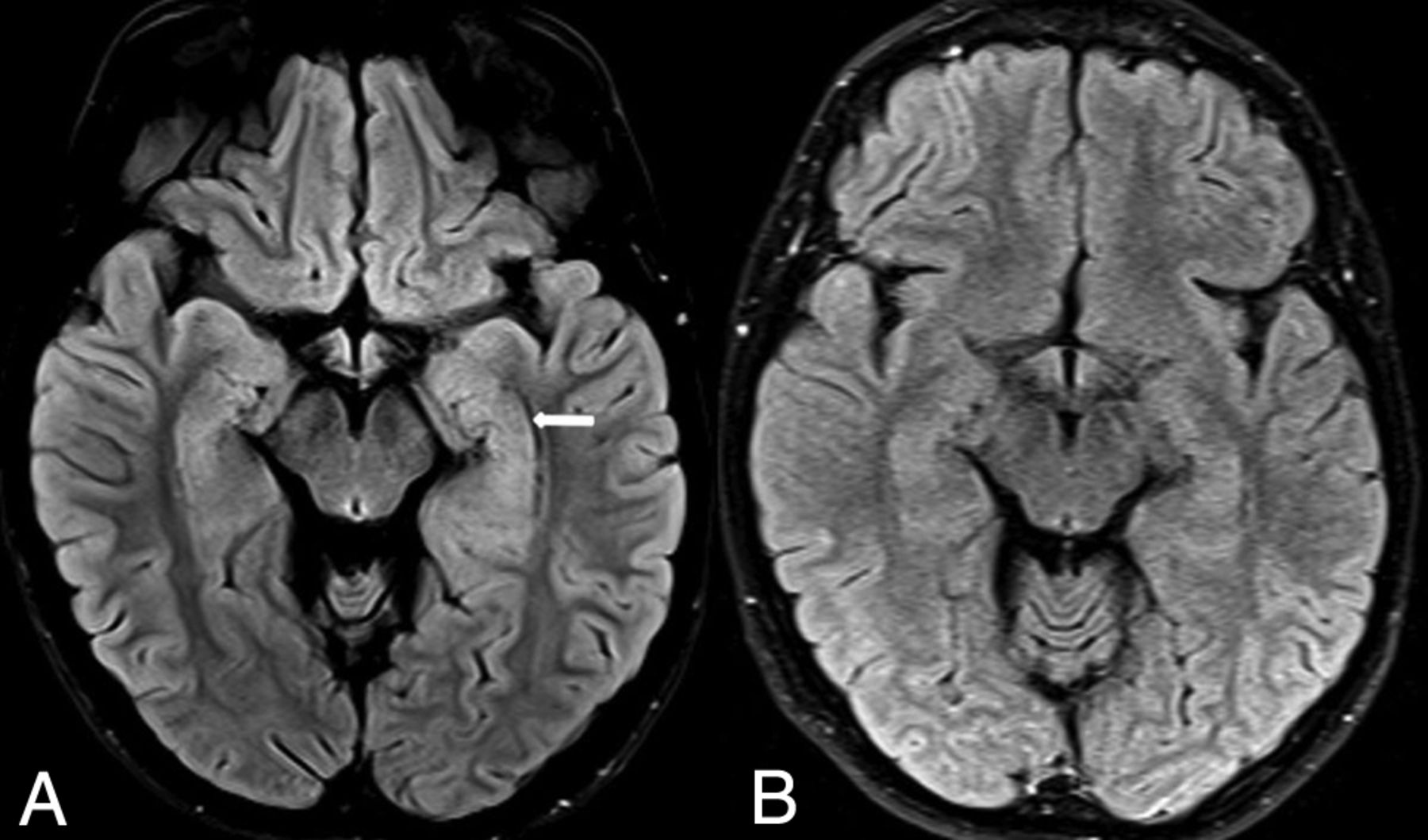
- Fig 13.
Autoimmune encephalitis in a 23-year-old man with a history of acute lymphoblastic leukemia treated with chemotherapy 2 years prior. He presented with worsening headache and speech changes. There was hyperintense signal within the left hippocampus on FLAIR (A, arrow), which did not have reduced diffusion and did not enhance on postcontrast T1WI (not shown) because the infectious work-up findings were also negative. The hippocampal abnormality resolved 1 year later on follow-up FLAIR (B).
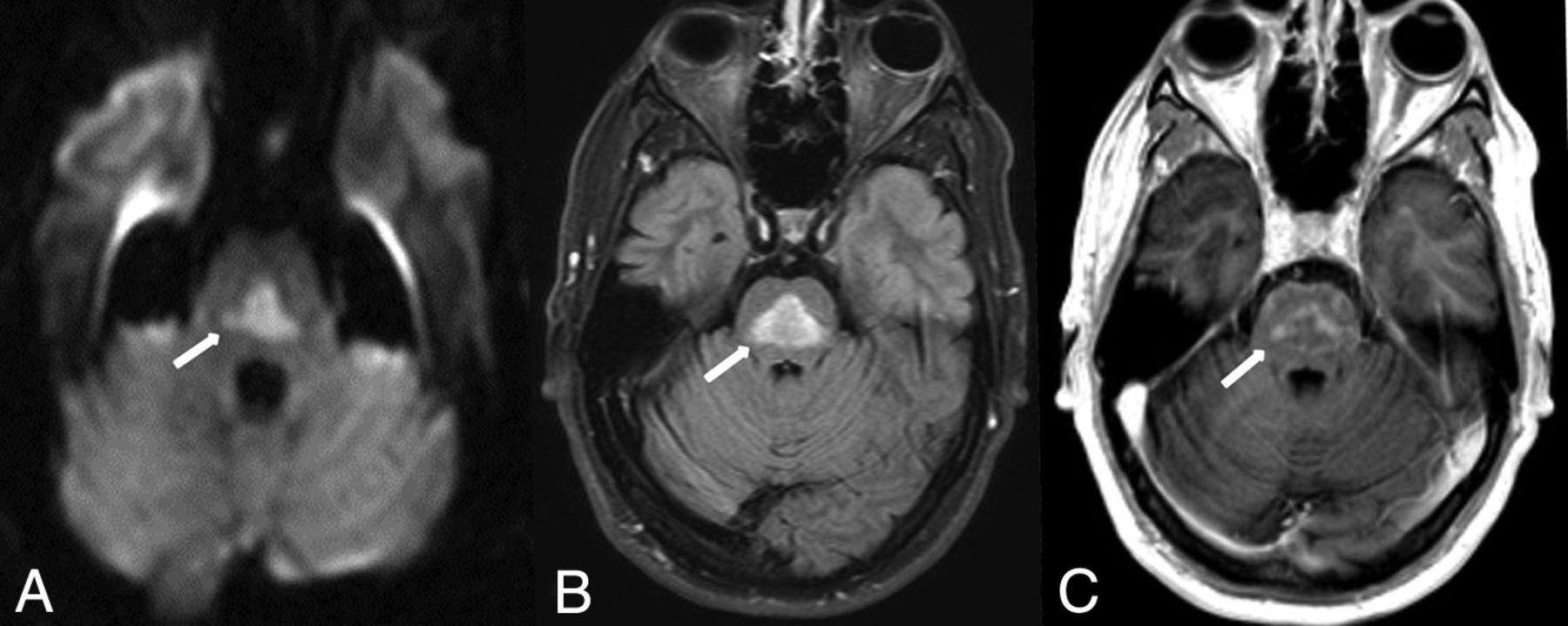
- Fig 14.
Pontine-type ODS in a 45-year-old man who presented with acute confusion due to a correction of the serum sodium (Na+) level from 101 mEq/L during 1 day. There was characteristic pontine reduced diffusion on DWI (A, arrow) and FLAIR (B, arrow). Postcontrast T1WI demonstrated mild enhancement, consistent with the subacute phase of ODS (C, arrow).
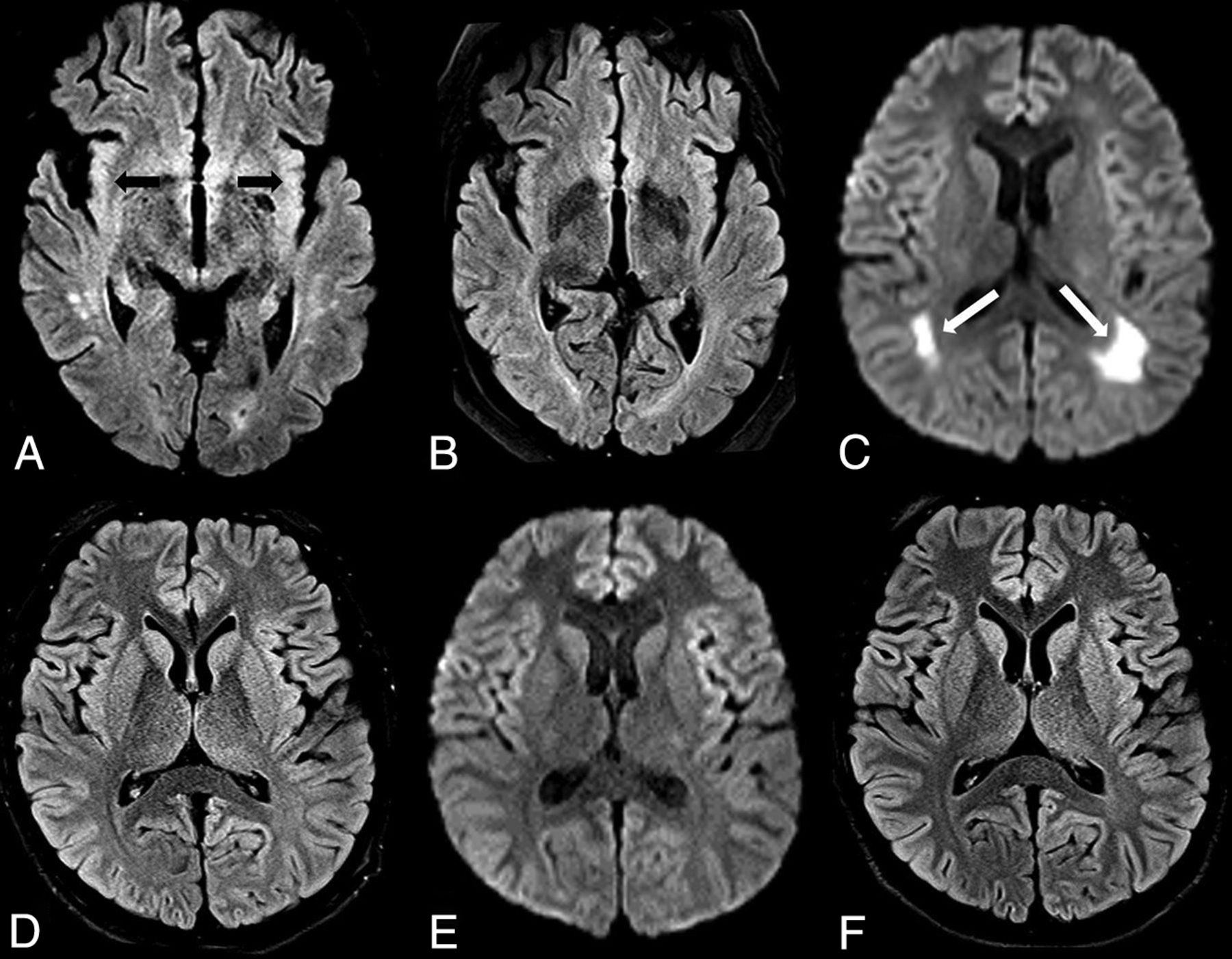
- Fig 15.
Two different appearances of uremic encephalopathy. A and B, A 54-year-old man with chronic kidney disease, altered mental status, and an acute rise in the blood urea nitrogen level (range, 45–114 mg/dL during the 10 days prior). Reduced diffusion was present within the bilateral insular cortices, as shown on FLAIR (A, arrows). By 40 days later, the insular abnormalities had resolved on FLAIR (B). C–E, A different 18-year-old male patient (previously healthy) with altered mental status from more severe uremic encephalopathy. The patient was later found to be in end-stage acute renal failure (blood urea nitrogen level range, 90-114 mg/dL during the 2 days before MR imaging). The initial MR imaging demonstrated reduced diffusion on DWI (C, arrows) within the posterior PVWM, but without abnormality on FLAIR (D). One month later, the symptoms and DWI MR imaging findings (E) had resolved, without abnormalities on FLAIR (F).
- Fig 16.
AHE in a 34-year-old woman with acute liver failure from acetaminophen overdose, having severe serum ammonia level elevation (206 μg/dL), with characteristic insular (dotted arrows) and thalamic involvement (arrows) on FLAIR (A) and T2WI (B). By 3 weeks later, the signal abnormalities and symptoms had resolved, but there was mild resultant insular atrophy (C).
- Fig 17.
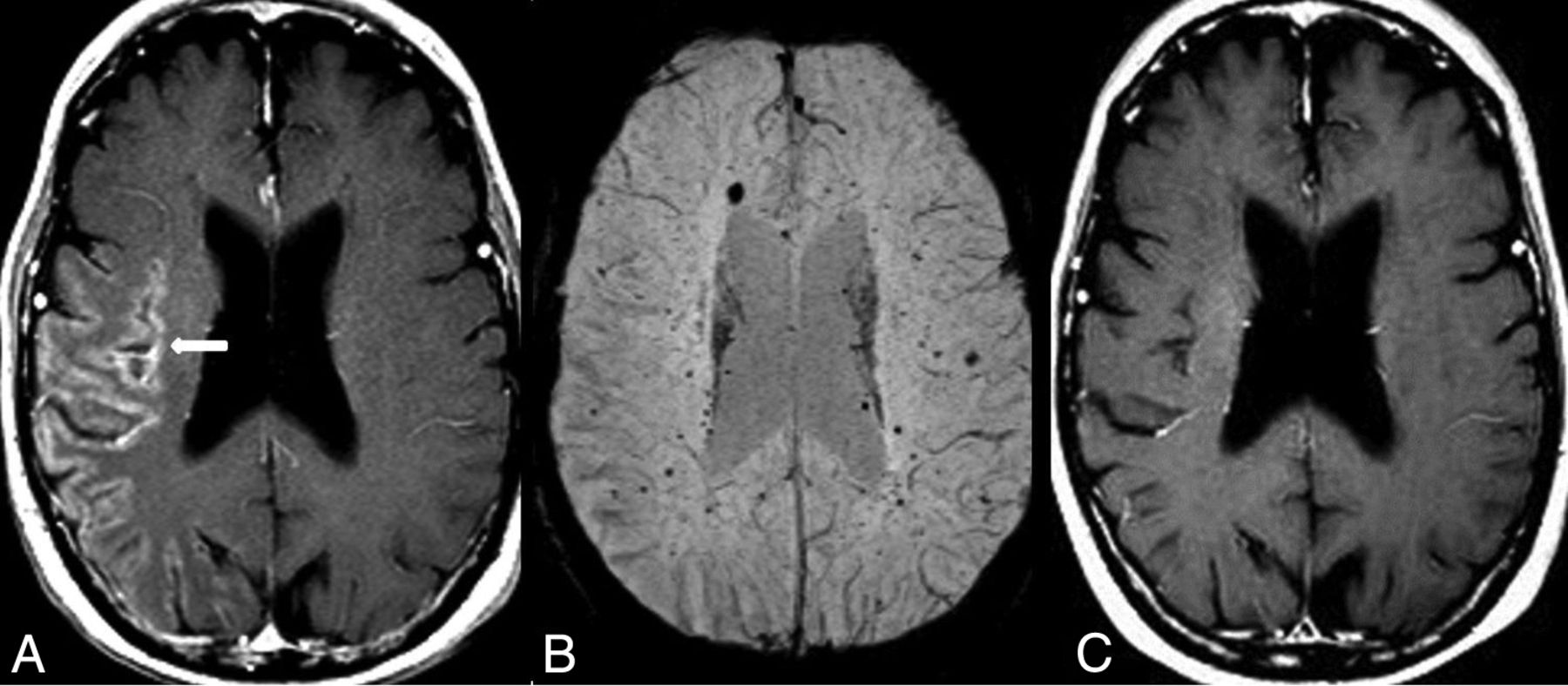
SMART syndrome in a 56-year-old man with acute headaches and confusion, who had a history of radiation therapy >40 years ago for a pineal tumor. Unilateral, gyriform temporo-occipital enhancement was noted on postcontrast T1WI (A), with numerous microhemorrhages on SWI (B). The symptoms resolved 4 days later, along with resolution of the abnormal enhancement on postcontrast T1WI (C).
- Fig 18.
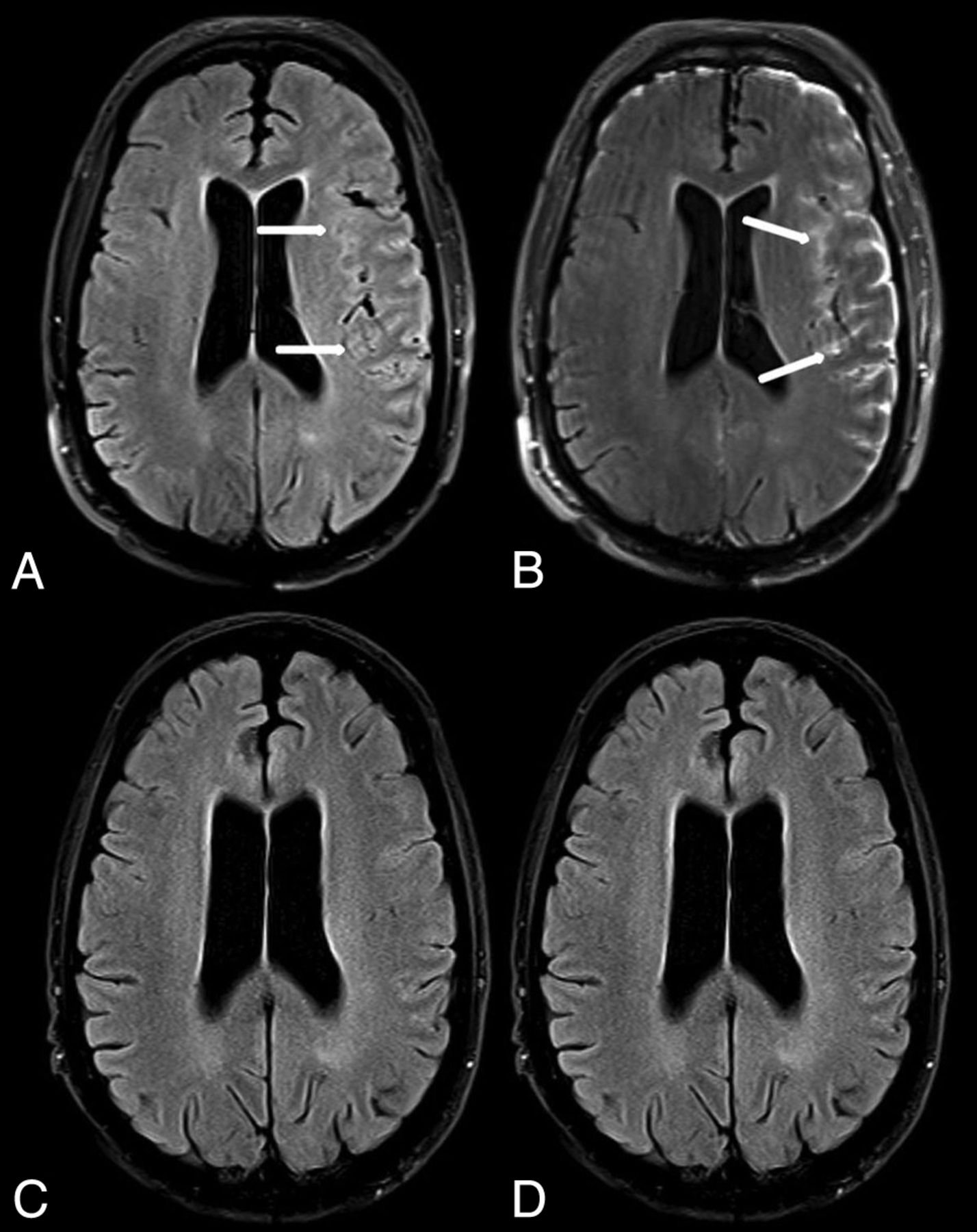
Leptomeningeal carcinomatosis in a 60-year-old man with an acute presentation of altered mental status and seizure. The initial MR imaging demonstrated leptomeningeal hyperintense signal and enhancement on pre- (A, arrows) and postcontrast FLAIR (B, arrows), diagnosed as metastatic melanoma later via direct biopsy. The imaging findings were completely resolved 3 months later, as demonstrated on pre- (C) and postcontrast FLAIR (D).
- Fig 19.
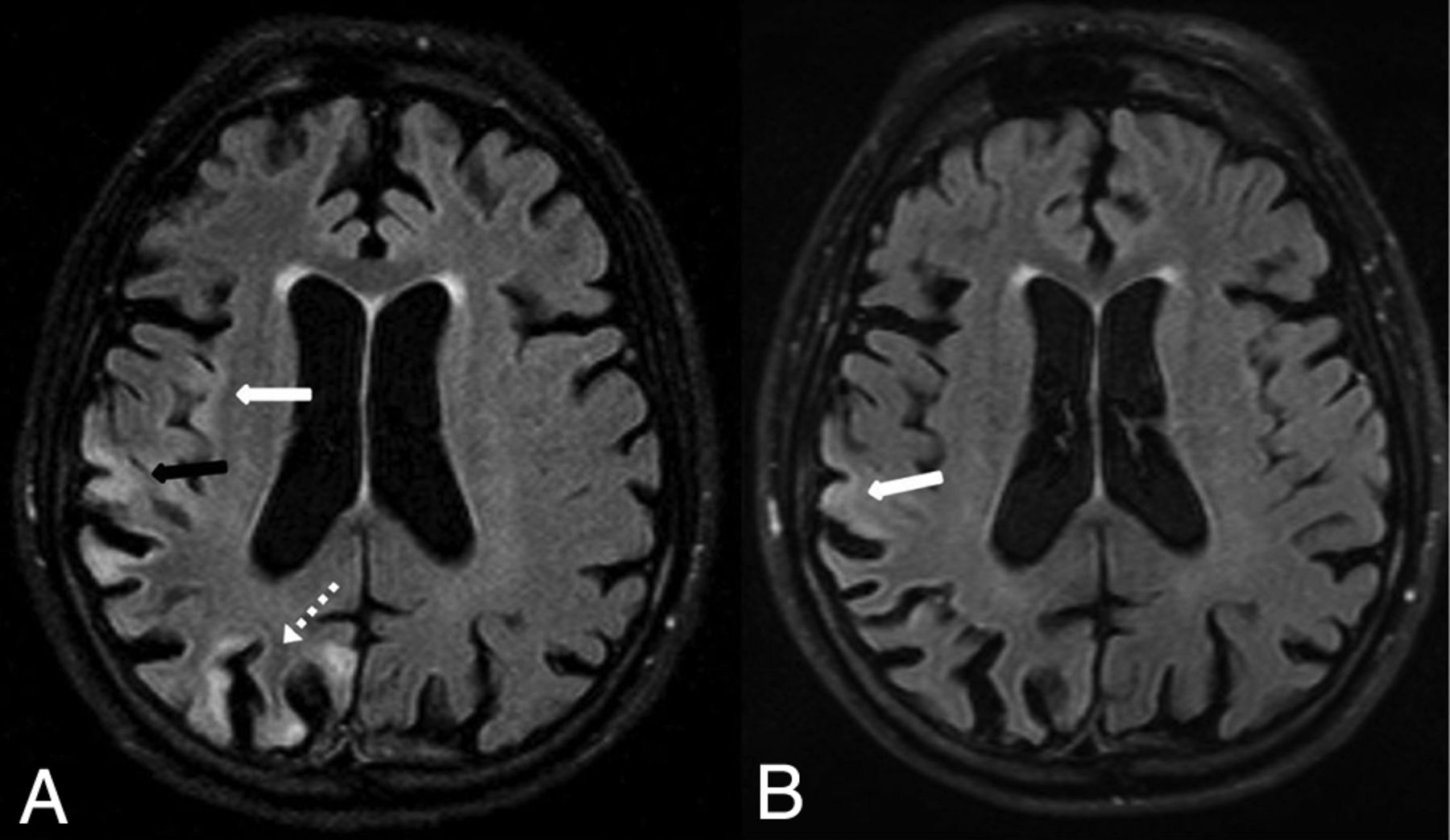
Status epilepticus in a 58-year-old man with reduced diffusion (not shown) and high signal on FLAIR (A) within the right parietal (A, black arrow), occipital (A, dotted arrow), and insular cortices (A, white arrow). By 12 days later, the findings were mostly resolved except for mild residual hyperintensity within the right parietal cortex, as demonstrated on follow-up FLAIR (B, arrow).



















Tables
Etiologies of potentially reversible acute encephalopathy syndromes
Etiologies Vascular (RCVS, TGA, TMA/DIC) Infection (encephalitis, meningitis) Toxic (PRES, ATL, CO, ARE), medication-induced (RSL, REACT, serotonin) Autoimmune encephalitis Metabolic (ODS, uremic encephalopathy, AHE) Idiopathic/inflammatory (SMART syndrome) Neoplasm (leptomeningeal carcinomatosis) Seizure Note:—TGA indicates transient global amnesia; DIC, disseminated intravascular coagulation; ARE, alcohol-related encephalopathy.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.