
Abstract
BACKGROUND AND PURPOSE: Clinical outcomes after endovascular treatment for acute basilar artery occlusions need further investigation. Our aim was to analyze predictors of a 90-day good functional outcome defined as mRS 0–2 after endovascular treatment in MR imaging–selected patients with acute basilar artery occlusions.
MATERIALS AND METHODS: We analyzed consecutive MR imaging–selected patients with acute basilar artery occlusions endovascularly treated within the first 24 hours after symptom onset. Successful and complete reperfusion was defined as modified TICI scores 2b–3 and 3, respectively. Outcome at 90 days was analyzed in univariate and multivariate analysis regarding baseline patient treatment characteristics and periprocedural outcomes.
RESULTS: One hundred ten patients were included. In 10 patients, endovascular treatment was aborted for failed proximal/distal access. Overall, successful reperfusion was achieved in 81.8% of cases (n = 90; 95% CI, 73.3%–88.6%). At 90 days, favorable outcome was 31.8%, with a mortality rate of 40.9%; the prevalence of symptomatic intracranial hemorrhage within 24 hours was 2.7%. The median time from symptom onset to groin puncture was 410 minutes (interquartile range, 280–540 minutes). In multivariable analysis, complete reperfusion (OR = 6.59; 95% CI, 2.17–20.03), lower pretreatment NIHSS (OR = 0.77; 95% CI, 0.64–0.94), the presence of posterior communicating artery collateral flow (OR = 2.87; 95% CI, 1.05–7.84), the absence of atrial fibrillation (OR = 0.18; 95% CI, 0.03–0.99), and intravenous thrombolysis administration (OR = 2.75; 95% CI, 1.04–7.04) were associated with 90-day favorable outcome.
CONCLUSIONS: In our series of MR imaging–selected patients with acute basilar artery occlusions, complete reperfusion was the strongest predictor of a good outcome. Lower pretreatment NIHSS, the presence of posterior communicating artery collateral flow, the absence of atrial fibrillation, and intravenous thrombolysis administration were associated with favorable outcome.
ABBREVIATIONS:
- ABAO
- acute basilar artery occlusion
- BSS
- brain stem score
- EVT
- endovascular treatment
- GCS
- Glasgow Coma Scale
- IQR
- interquartile range
- IVT
- intravenous thrombolysis
- mTICI
- modified TICI
- PC-ASPECTS
- posterior circulation ASPECTS
- PcomA
- posterior communicating artery
- sICH
- =symptomatic intracranial hemorrhage
Acute basilar artery occlusion (ABAO) is a devastating type of stroke, with a natural history showing a mortality rate of up to 90% and a severe residual deficit in 65% of patients without treatment.1
Although endovascular treatment (EVT) is the criterion standard therapy for patients with acute ischemic stroke in the anterior circulation and proximal arterial occlusion, results from randomized clinical trials regarding the effectiveness of EVT for ABAO are still lacking.2 Nevertheless, EVT is considered useful and routinely performed in real-world practice. Expert opinions have encouraged this practice3 to maximize the chance of reperfusion and good clinical outcome.
However, there are contradictory results on predictors of functional outcome as well as on the best reperfusion strategies (IV thrombolysis [IVT] alone, EVT, bridging therapy) in patients with ABAO. The Acute Basilar Artery Occlusion: Endovascular Interventions versus Standard Medical Treat-ment (BEST) randomized trial was stopped ahead of time because of the higher rate of crossover between treatment groups.4
Using data from our prospective registry, we aimed to investigate predictive factors of 90-day good functional outcome in a large cohort of patients with ABAO. Because of the high sensitivity in detecting posterior fossa ischemic lesions and infarct volume, MR imaging is the main selection technique for patients with acute ischemic stroke at our department, and all included subjects were MR imaging–selected.
MATERIALS AND METHODS
Inclusion Criteria and Patient Characteristics
We reviewed all patients referred to our hospital with ABAO confirmed by MR imaging and subsequently treated with EVT from January 2011 to October 2018. The inclusion criteria for EVT were the following: 1) patients with ABAO and acute stroke detected on cerebral MR imaging admitted within 24 hours from symptom onset; 2) patients with pertinent clinical deficits undergoing an evaluation by a physician (without NIHSS limits); and 3) confirmation of ABAO on angiography. Patients were considered not eligible for EVT (and received medical management) on the basis of the following exclusion criteria: 1) prestroke mRS score of more than two; 2) life expectancy of <6 months; 3) imaging evidence of cerebellar mass effect or acute hydrocephalus; and 4) bilateral extended brain stem ischemia.
Baseline characteristics, NIHSS, Glasgow Coma Scale (GCS), mothership or drip and ship strategy, and use and time of IVT were assessed by a stroke neurologist on admission. An NIHSS score of 40 was assigned to comatose patients with a GCS of 3. The local ethics committee approved the use of the patients' data for this study.
Neuroimaging Assessment
We recorded 2 scores to measure early ischemic changes on DWI in the posterior circulation: 1) the posterior circulation ASPECTS (PC-ASPECTS),5 and 2) the DWI brain stem score (BSS).6
The DWI BSS separately analyzes the medulla, pons, and midbrain, considering the right and left sides separately. One point was given for each unilateral DWI lesion at the brain stem level (medulla, pons, and midbrain) that occupied less than half of the area; and 2 points were given if the lesion occupied more than half of the area. The brain stem DWI lesion score ranged from 0 to 12. There were no limits on the PC-ASPECTS and DWI BSS scales for inclusion of patients.
The level of ABAO was determined as follows: proximal segment of the basilar artery (from the vertebral artery junction to the anterior inferior cerebellar artery), middle segment (from the anterior inferior cerebellar artery to the superior cerebellar artery), and distal segment (above the superior cerebellar artery).7 The pretreatment collateral score for the posterior circulation was collected and defined as follows: 0, no posterior communicating artery (PcomA); 1, unilateral PcomA; and 2, bilateral PcomA.8
Pretreatment imaging findings were retrospectively assessed by an experienced interventional neuroradiologist (M.M.) blinded to the clinical outcome. For each patient, imaging was retrospectively assessed by a second interventional neuroradiologist (C.D.), blinded to both the first reader's scoring and the clinical outcome. In case of discrepancy, a consensus was reached with an additional reader (I.D.).
Reperfusion Therapy
Patients received either bridging therapy (EVT combined with IVT) or EVT alone. IVT was administered within a maximum of 4.5 hours from symptom onset, according to the current guidelines.9 Conventional clinical and laboratory inclusion and exclusion criteria for IVT thrombolysis were applied. Because it has been reported that larger cerebellar infarct volume (>75%) is potentially associated with hemorrhagic transformation, IVT was not administrated in case of extensive cerebellar ischemia on DWI sequences.10
All patients were treated in a neuroangiography suite under general anesthesia or conscious sedation, after evaluation by a dedicated anesthesiologist team. An 8F (Neuron Max; Penumbra) guiding catheter was advanced into the V2 segment of the vertebral artery, usually the largest one. For stent retriever thrombectomy, a 0.021-inch microcatheter was navigated through the basilar occlusion using a 0.014-inch microwire under fluoroscopic guidance. A Solitaire FR (Medtronic) or Trevo (Stryker) device was used for EVT.
Stent retriever11 or a Direct Aspiration First-Pass Technique12 (with a SOFIA 5F or 6F [MicroVention] intermediate catheter) was used.
Successful and complete reperfusion was defined as a modified TICI (mTICI) 2b–3 and 3, respectively. In the absence of a specific definition in the posterior circulation of TICI 2b and according to our experience, we considered TICI 2b a partial perfusion with distal occlusion of a posterior cerebral artery, AICA, PICA, or superior cerebellar artery.13
We recorded periprocedural complications: embolization in an unaffected territory, arterial dissection/perforation, vasospasm, and subarachnoid hemorrhage.
Delays from stroke-onset to MR imaging, stroke-onset to IVT, stroke-onset to groin puncture, MR imaging to groin-puncture, stroke-onset to reperfusion, and groin puncture to reperfusion were recorded for all patients.
Follow-Up and Outcome
All patients underwent cerebral CT or MR imaging within the 24 hours after the procedure. Growth of the infarct core, basilar artery early re-occlusion, and hemorrhagic complications were recorded. Symptomatic intracranial hemorrhage (sICH) was defined as imaging demonstrating hemorrhage associated with an increase of ≥4 points in the NIHSS score.9
The 90-day mRS was assessed by a stroke neurologist or by a phone call with the patient, his or her relatives, or his or her general practitioner. Favorable outcome was defined by mRS ≤ 2, and poor outcome, mRS 3–6. Mortality at 90 days was also recorded.
Statistical Analysis
Continuous variables are expressed as means ± SD or medians (interquartile range, [IQR]), and categoric variables are expressed as numbers (percentage). Normality of distributions was assessed using histograms and the Shapiro-Wilk test. Rates of angiographic and clinical outcomes were estimated by calculating the exact binomial 95% confidence intervals. Baseline characteristics (patient and treatment characteristics) and periprocedural outcomes (recanalization and adverse events) were compared between patients with and without favorable outcomes at 90 days using the Student t test for Gaussian continuous variables, the Mann-Whitney U test for non-Gaussian continuous variables, and the χ2 test (or Fisher exact test when the expected cell frequency was <5) for categoric variables, as appropriate. To assess the independent predictors of favorable outcomes, we performed a first-multivariable Firth penalized-likelihood logistic regression to account for the small sample size14), including all patient and treatment characteristics with a P < .10 in univariate analyses, using a backward selection procedure with P < .10 as a selection criterion. Before developing the multivariable model, we examined the log-linearity assumption for continuous characteristics (irrespective of previous univariate analyses) using restricted cubic spline functions by comparing the models using only a linear term with models containing both the linear and cubic spline terms using a likelihood ratio test (all log-linearity assumptions were established and all continuous variables were analyzed without transformation). We also examined the absence of colinearity between the candidate predictors by calculating the variance inflation factors.15,16
To prevent collinearity between pretreatment NIHSS and pretreatment GCS (variance inflation factor >8; for all other predictors, variance inflation factors values were <2), we performed separate multivariate analyses, including either pretreatment NIHSS or pretreatment GCS. Two multivariable models were performed by including and excluding complete recanalization as a covariate. This performance was to determine the impact of the other investigated pretreatment variables, independent of the angiographic result. We examined the performance of the selected models in terms of calibration using the Hosmer-Lemeshow goodness-of-fit test and discrimination by calculating the C-statistics.14 We also derived the McFadden Pseudo R-Squared from the likelihood for the selected models and the null model (including intercept only). The results of multivariate analyses are expressed as odds ratios with 95% confidence intervals of favorable outcome. Statistical testing was performed at the 2-tailed α level of .05. Data were analyzed using the SAS software package, release 9.4 (SAS Institute).
RESULTS
Overall, 226 consecutive patients with ABAO were admitted to our hospital. One hundred seven patients treated by conservative management alone (antiplatelet/anticoagulant/IVT) and 9 patients without MR imaging performed before EVT were excluded, resulting in a total of 110 included MR imaging–selected patients who underwent EVT (On-line Fig 1). Patient and treatment characteristics are reported in On-line Table 1. The mean age was 67 ± 12 years, 60% (n = 66) were men, and the median pretreatment NIHSS score was 22 (IQR, 14–40). Thirty-four (31%) patients had proximal ABAO, 23 (21%) had middle ABAO, and 53 (48%) presented with a distal ABAO. The median door-to-puncture time was 67 minutes (IQR, 34–530 minutes). Seventy-nine patients (72%) were intubated for low GCS scores (n = 23) and for EVT (n = 56).
IVT before thrombectomy was administered in 37% (n = 41) of patients. The median time from symptom onset to groin puncture was 410 minutes (IQR, 280–540 minutes). In 10 patients, EVT was unsuccessful because of the impossibility of crossing the occlusion (n = 4) or impossible access/tortuosity (n = 4) and perforation (n = 2).
Of the 100 patients receiving at least 1 device pass, the first-line treatment strategy was stent retriever in 30%, contact aspiration in 23.6%, and a combined stent retriever and contact aspiration strategy in the remaining 37.3%.
Angiographic and Clinical Outcomes
Main outcomes are summarized in Table 1. Successful reperfusion (mTICI 2b–3) was achieved in 81.8% (n = 90; 95% CI, 73.3%–88.6%) with a median number of passes of 1 (IQR, 1–2), and a median time of 45 minutes (IQR, 22–70 minutes) from groin puncture. Reperfusion was complete (mTICI 3) in 60.9% of patients (n = 67; 95% CI, 51.1%–70.1%). Overall, procedural complications occurred in 18.2% (n = 20; 95% CI, 11.4%–26.7%) of patients. These included 13 (11.8%) vertebral dissections, 5 distals embolisations (4, 6%) angiographic distal embolizations, and 2 (1.8%) vasospasms. Intracranial hemorrhagic complications within 24 hours occurred in 11.8% (n = 13; 95% CI, 6.4%–19.4%) of patients, with 3 (2.7%) symptomatic events. At 90 days, 35 patients (31.8%; 95% CI, 23.2%–41.4%) achieved good outcome (mRS 0–2), 75 (68.1%; 95% CI, 59%–76%) had a poor outcome (mRS 3–6), and among those, 45 subjects (40.9%; 95% CI, 31.6%–50.7%) died. Overall, 64 patients had post-EVT MR imaging. Of these, 51 (79.7%) had successful recanalization (TICI 2b-3), while 13 (20.3%) were TICI 0–2a. Among those having a successful recanalization, 28 (55%) presented with an infarct growth. Functional independence at 3 months was lower (30% versus 70%) in the group with infarct growth compared with the group without infarct growth (details in the On-line Fig 2).
Angiographic and clinical outcomesa
Predictors of Favorable Outcome at 90 Days
In univariate analyses, lower pretreatment NIHSS and GCS scores, lower DWI BSS values and PC-ASPECTS, the presence of PcomA collateral flow, the absence of thalamus involvement, IVT before EVT, the absence of atrial fibrillation, onset-to-groin puncture time, no admission to the intensive care unit, and mothership–treated strategy were associated with a good outcome (P value < .10, On-line Table 2) and were included in the multivariable analyses. Due to the strong collinearity between 2 variables, 2 separate multivariate analyses were performed, including either pretreatment NIHSS (Table 2) or GCS (On-line Table 3).
Independent predictors of favorable outcomea
Multivariable Model Including NIHSS
We tested 2 models: 1) excluding complete recanalization (mTICI 3), and 2) including complete recanalization as an independent candidate predictor. In the first model, lower pretreatment NIHSS (P = .007), the presence of PcomA collateral flow (P = .039), IVT administration (P = .04), and absence of atrial fibrillation (P = .049) were significantly associated with the likelihood of good outcome (Table 2). Association with onset-to-groin puncture and pretreatment DWI BSS was on the borderline of significance.
In model 2, including mTICI 3 recanalization, lower pretreatment NIHSS (P = .03), the presence of PcomA collateral flow (P = .02), and complete reperfusion (P < .001) were significantly associated the good outcome.
Both multivariate models had good discrimination (C = 0.803 for the first and C = 0.816 for the second model) with no deviation in calibration as indicated by the Hosmer-Lemeshow goodness-of-fit test (P = .85 for the first and P = .74 for the second model).
Multivariable Model Including GCS
Similar results were found when the pretreatment GCS was considered as a candidate variable rather than the pretreatment NIHSS (On-line Table 3).
DISCUSSION
Our study, analyzing 110 MR imaging–selected patients with ABAO, highlighted complete reperfusion after EVT as the strongest predictor of 90-day good functional outcome. Moreover, a lower pretreatment NIHSS score, the absence of atrial fibrillation, PcomA collateral flow, and IVT (bridging therapy) were predictors of functional independence. Although GCS was also strongly associated with a good neurologic outcome, the NIHSS score was considered more accurate in the evaluation of the pretreatment clinical status.
Influence of Complete Reperfusion on Favorable Outcomes
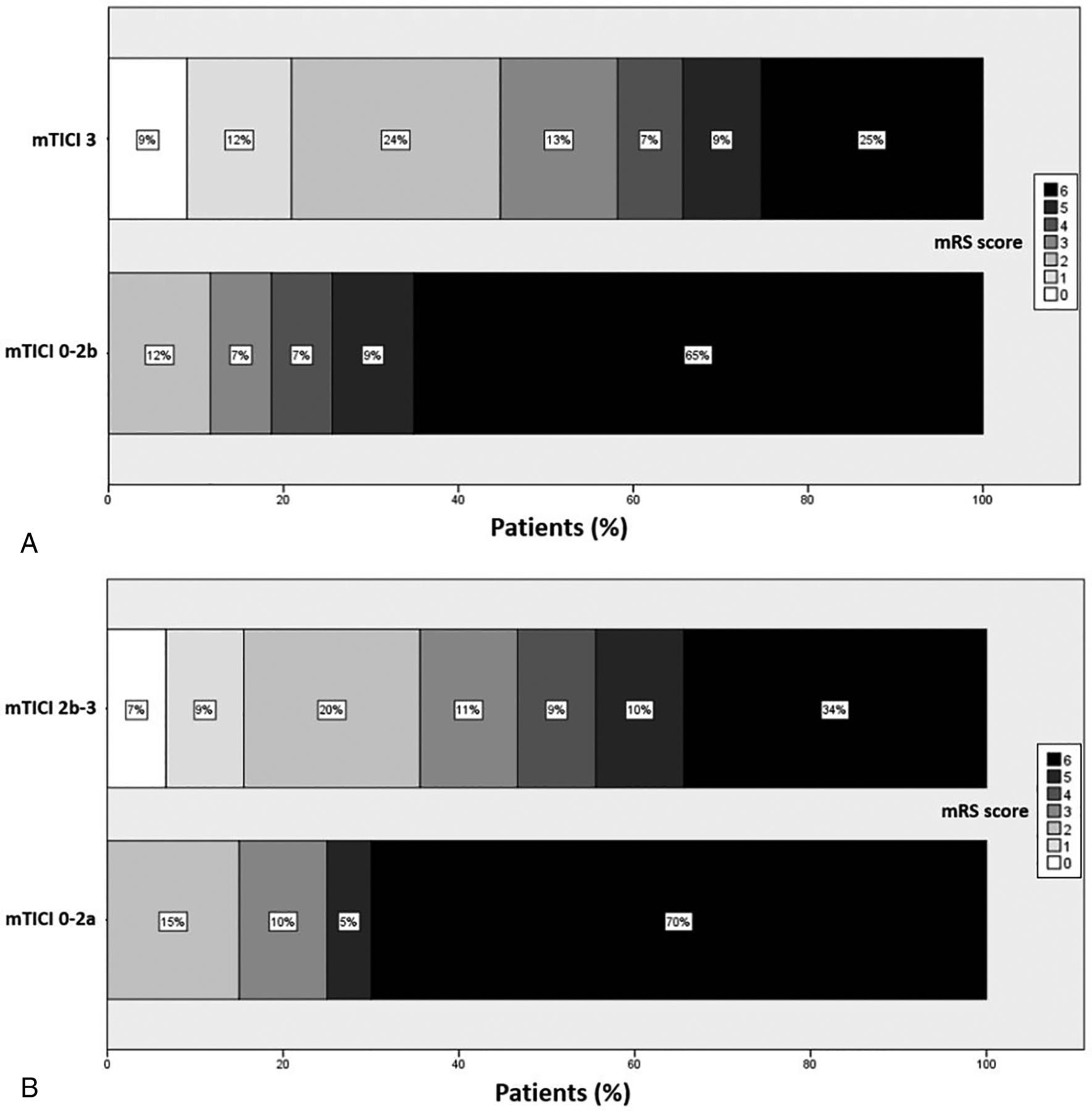
Our rate of successful reperfusion (mTICI 2b–3, 81.8%) was in the range of those reported in other series showing a rate between 79% and 96%.17⇓⇓⇓-21 Patients with mTICI 3 reperfusion had a better mRS at 90 days than patients with mTICI 2b (44.8% among mTICI 3 versus 8.7% among patients with mTICI 2b). On-line Figure 3 shows as complete recanalization (mTICI 3) increased the rate of good functional outcome compared with mTICI 0-2b. In addition, there was a shift to higher rates of independence in the group with successful reperfusion compared with unsuccessful recanalization. Furthermore, in a multivariate analysis, complete reperfusion (obtained in 60.9% of patients) was the strongest predictor of a 90-day favorable outcome. This result is in accordance with what was reported in previous published series of mechanical thrombectomy for posterior circulation acute ischemic stroke.20,22⇓-24 This point probably underlines the importance of achieving complete reperfusion in the posterior circulation, likely due to the extremely functional anatomic region involved.

Functional outcomes at 90 days according to the mRS score. Distribution of 90-day mRS scores in patients with complete (mTICI 3) versus mTICI 0–2b reperfusion (A) and success of reperfusion (mTICI 2b–3) versus mTICI 0-2a (B). Scores range from 0 to 6, with higher scores indicating greater disability.
Not surprisingly, failure to achieve reperfusion has been reported as a strong predictor of mortality.17 These results are important because they outline the efficacy of EVT in ABAO and the impact on the clinical outcome.
Clinical Predictors of Outcome
In our series, the rate of favorable outcome was slightly lower (31.8%) compared with other reports (42%–54%),4,17,19,25⇓⇓-28 with higher rates of mortality (40.9% versus 12%–35%)4,19,25⇓⇓⇓-29 and poor outcome (mRS 3–5, 27%). These results suggest that among patients with posterior circulation ischemic stroke, if reperfusion appears to be an important factor in functional independence, other variables potentially influence the final neurologic status. It has been suggested that occlusion of small perforating arteries in thromboembolic ABAO may persist even after clot removal and recanalization of the basilar artery, leading to irreversible brain stem ischemic lesions.20
In addition, compared with the literature, our patient group was older (mean age, 66.9 versus 58–64 years),26,29,30 with higher initial stroke severity (mean baseline NIHSS score of 22 versus 13–17).11,21,25,29 Furthermore, >70% of patients (80 comatose patients) required admission to the intensive care unit for mechanical ventilation.
Younger age has been demonstrated to be associated with favorable outcomes.25 On the other hand, 60 years of age and older was an independent predictor of mortality.17 A higher GCS score and a lower baseline NIHSS are known to be predictors of good outcome in patients with ABAO.25,26,28,31 Most interesting, it has been shown that despite recanalization, patients with ABAO with a baseline NIHSS of ≥13 have poorer outcomes compared with those with a mild-to-moderate deficit.17 In our series, the median NIHSS score among patients achieving a poor outcome was 40, and the median GCS was 3. Accordingly, we can reasonably state that patients with very severe disease at admission have a quite low probability of achieving a good neurologic outcome even if treated with the best medical management and with the most advanced interventional techniques.
Delay of Reperfusion Therapy
Our regional network organization 31 may explain our longer median time from onset to groin puncture and imaging to puncture time (410 minutes versus 242–405 minutes and 99 minutes versus 50–60 minutes) compared with previous findings.17,25,26,32
Hospitals in our region (>2,700,000 habitants with an area of 27,376 km2) are not geographically close together, so most of those with the drip and ship paradigm (representing 71.6% of subjects) underwent a re-evaluation MR imaging on arrival at our comprehensive stroke center, which might increase the onset-to-groin puncture time and imaging-to-puncture time.
In addition, 72% of patients (79 subjects) needed to be intubated for their low GCS (n = 23) and for EVT (n = 56). All these factors contributed to an increase in the median time from onset to groin puncture and imaging to groin puncture.
The Basilar Artery International Cooperation Study (BASICS) demonstrated that the probability of poor outcome was significantly increased when recanalization therapy was started after 6 hours.33 However, data in the literature are contradictory, with series showing a not significant correlation between patients treated before and after 6 hours.26 In our study, onset-to-groin puncture was not independently associated with 90-day mRS 0–2 at multivariable analysis. These data support the hypothesis that functional prognosis might be governed by other factors such as baseline neurologic presentation, collateral flow, and initial ischemia.27
Influence of Atrial Fibrillation
Different from what was reported before, in our cohort, the absence of atrial fibrillation was associated with a favorable outcome. Atrial fibrillation, associated with fresh thrombus and less atherosclerotic vessel damage, was an independent predictor of successful reperfusion in previous series.34 In addition, it has been reported that cardiac embolism is more frequently related to distal basilar artery occlusion, which is generally associated with higher rates of successful recanalization after EVT.35,36
PcomA Collateral Flow
The positive impact of collateral blood flow on clinical outcomes has been previously demonstrated.19,21,28,37 Scores used to determine collateral flow are heterogeneous, and there is not a consensus for the posterior circulation. Here, the presence of collateral flow in the PcomA was defined using an easy-to-use, validated scale assessed on baseline MR imaging8 and was associated with a 90-day favorable outcome. Moreover, other authors reported that better collateral supply significantly increases recanalization rates,19 providing blood flow to the penumbral tissue and decreasing the final infarct core.38 It is conceivable that the presence of a PcomA artery should be checked during the pretreatment imaging and patient selection, considering that subjects with PcomA collateral flows are more likely to benefit from mechanical thrombectomy and have a higher chance of recovery. In addition, the presence of a PcomA artery impacted the outcome independent of complete reperfusion, indicating the importance of the collateral blood flow in patients with ABAO.
Impact of Bridging Therapy
In our cohort, the use of IVT (37.3% of patients) increased the 90-day favorable outcome, without higher hemorrhagic risk. Similarly, Gory et al17 reported higher mortality rates among patients with ABAO not receiving IVT. These findings may support the use of IVT in ABAO, underlining its role in reperfusion strategy. In our study, the sICH rate was quite low (2.7%) compared with that reported in other series (0 to 11.8%).17⇓-19,25⇓⇓-28 In agreement with recent series,39 it is likely that the low rate of sICH is partly explained by the MR imaging–based patient selection, with no administration of IVT for patients with large stroke volumes.
Limitations
Our study has limitations. First, it is a monocentric retrospective, nonrandomized observational registry study. Our sample size remains limited to assess the predictors of favorable outcome, despite being the largest EVT study of MR imaging–selected patients with ABAO. First, we could not exclude several predictors not being identified due to lack of adequate statistical power. Although there is no single sample calculation, we performed an a posteriori power calculation by calculating the smallest effect size (expressed as an odds ratio) that our sample size (35 patients with favorable outcome and 75 patients without it) allows to detect a 5% significance level (2-sided) with a 80% power. On the basis of our study sample, we could detect odds ratios of 4.24 and 3.38, assuming an exposure prevalence of 10% and 50% in patients without favorable outcome. In addition, we could not exclude a risk of overfitting in multivariate analysis. For these reasons, the present findings should be confirmed in further larger studies or in the ongoing randomized controlled trials.40
CONCLUSIONS
This study emphasizes the impact of complete successful reperfusion in patients with ABAO, which appeared the strongest predictor of a 90-day favorable outcome. The presence of PcomA collateral flow, lower pretreatment NIHSS scores, the absence of atrial fibrillation, and IV thrombolysis administration was also associated with favorable outcomes. Nevertheless, further randomized controlled trials are warranted to assess the patient-related factors determining clinical outcome.
Footnotes
Disclosures: Julien Labreuche—RELATED: Fees for participation in review activities such as data monitoring boards, statistical analysis, endpoint committees, and the like. Alain Bonafe—UNRELATED: Consultancy: Medtronic, Stryker, MicroVention. Pierre Henri Lefevre—UNRELATED: Payment for development of educational presentations: Medtronic, Stryker.
References
- Received February 3, 2020.
- Accepted after revision June 7, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}