
Abstract
BACKGROUND AND PURPOSE: The acute phase of aneurysmal SAH is characterized by a plethora of impending complications with the potential to worsen patients’ outcomes. The aim of this study was to evaluate whether an elaborated CTP-based imaging protocol during the acute aneurysmal SAH phase is able to prevent delayed infarctions and contribute to a better outcome.
MATERIALS AND METHODS: In 2012, an elaborated CTP-based protocol was implemented for the management of patients with aneurysmal SAH. Retrospective analysis of patients with aneurysmal SAH treated from 2010 to 2013 was performed, comparing the patients treated before (group one, 2010–2011) with those treated after the protocol implementation (group two, 2012–2013) with regard to delayed infarctions and outcome according to the mRS at 3-months’ follow-up.
RESULTS: A total of 133 patients were enrolled, of whom 57 were included in group 1, and 76, in group 2. There were no significant differences between the groups concerning baseline characteristics. In the multivariate analysis, independent predictors of a good outcome (mRS ≤ 2) were younger age (P < .001), lower World Federation of Neurosurgical Societies grade (P < .001), absence of delayed infarction (P = .01), and management according to the CTP protocol (P = .01). Larger or multiple infarctions occurred significantly more often in group 1 compared with group 2 (88% versus 33% of all delayed infarctions, P = .03). The outcome in group 2 was significantly better compared with group 1 (P = .005).
CONCLUSIONS: The findings suggest that implementation of an elaborated CTP protocol is associated with a better outcome. An earlier initiation of further diagnostics and treatment with prevention of large territorial and/or multiple infarctions might have led to this finding.
ABBREVIATIONS:
- aSAH
- aneurysmal subarachnoid hemorrhage
- DCI
- delayed cerebral ischemia
- DIND
- delayed ischemic neurologic deficits
- ERT
- endovascular rescue therapy
- TCD
- transcranial Doppler sonography
- WFNS
- World Federation of Neurosurgical Societies
Aneurysmal SAH (aSAH) is a potentially lethal cerebrovascular disease due to primary and secondary brain function disturbances requiring elaborated treatment protocols in cerebrovascular centers with a thorough expertise in this field.1 In particular, the first 2 weeks after aneurysm rupture represent the most critical phase of aSAH, associated with impending complications with the risk of substantially worsening the functional outcome.2,3 The focus of most diagnostic and therapeutic measures in the acute phase after aSAH is preservation of sufficient cerebral perfusion with the aim of prevention of secondary brain injury. CTP has been increasingly implemented in imaging protocols for early prediction and detection of delayed cerebral ischemia (DCI) after aSAH.4⇓⇓⇓⇓-9 Nevertheless, there is a substantial heterogeneity in the CTP protocols used in different centers, not allowing general conclusions concerning the beneficial role of CTP protocols for the management of patients with aSAH in clinical practice. Despite the increased use of CTP, its actual diagnostic and prognostic value has not yet been completely determined. In 2012, an interdisciplinary imaging protocol was drawn up (neurosurgery and neuroradiology) at our institution (University Medical Center Göttingen) to facilitate a uniform management of patients with aSAH in the acute phase after ictus. Before 2012, CTP was performed only on an individual basis. The aim of this study was to investigate whether an elaborated CTP-based imaging protocol during the acute aSAH phase contributes to earlier identification of patients at risk for developing DCI and prevention of delayed infarction. Our hypothesis was that an elaborated CTP-based protocol would lead to a lower incidence of delayed infarction or to smaller infarctions and therefore would result in a better clinical outcome.
MATERIALS AND METHODS
Patient Population
This study was conducted according to the principles of the Declaration of Helsinki.10 The study (No. 16/9/20) was approved by the local Ethics Committee of University Medicine Göttingen. A patient’s consent for treatment was obtained according to the individual institutional guidelines. Due to the retrospective analysis of the data for this study, additional informed consent was deemed unnecessary.
A consecutive cohort of patients with aSAH treated at our department in a 4-year period was retrospectively analyzed. The inclusion criterion was complete data availability concerning the baseline characteristics, the ischemic complications, and the functional outcome. Patients treated before 2010 could not be included because of unavailability of complete data. Because the CTP protocol was implemented in 2012, group 1, in which CTP was performed on an individual basis, consisted of all patients treated between January 2010 and December 2011. Group 2, in which the CTP protocol was applied, consisted of the patients treated between January 2012 and December 2013. While management of patients with SAH using the CTP protocol was continued after December 2013, we decided to compare similar study periods to avoid data distortion during statistical analysis and eliminate possible confounders. Both groups were compared regarding the detection and management of ischemic complications as well as functional outcome.
All patients were admitted to the intensive care unit, where they were treated for at least 14 days after the bleeding. Aneurysm occlusion was performed within 48 hours after rupture by either microsurgical clipping or endovascular coiling. Patients who were admitted later were excluded. A CT scan was performed 4 hours after aneurysm treatment. Any infarction seen on that CT scan was considered treatment-associated and not related to DCI. Nimodipine was routinely administered orally or intravenously for 14 days in every patient. A neurologic assessment was performed 3 times per day (once in every shift) in all patients who were neither comatose nor sedated. Normotension and normovolemia were initially targeted in all patients. Blood flow velocities within the MCA were measured by transcranial Doppler sonography (TCD) daily for 14 days in all patients. In case of suspected DCI either clinically or radiologically, hypertension was initiated with a target systolic arterial pressure of 160–180 mm Hg. In case of refractory vasospasm with perfusion deficits, endovascular rescue therapy (ERT) was indicated, consisting of either dilation (proximal vasospasm), intra-arterial nimodipine administration (distal vasospasm), or both. The baseline characteristics were extracted from the patients’ medical records. The functional outcome at 3 months’ follow-up was documented during the follow-up examination of the patients in the neurosurgical outpatient department.
CTP Protocol
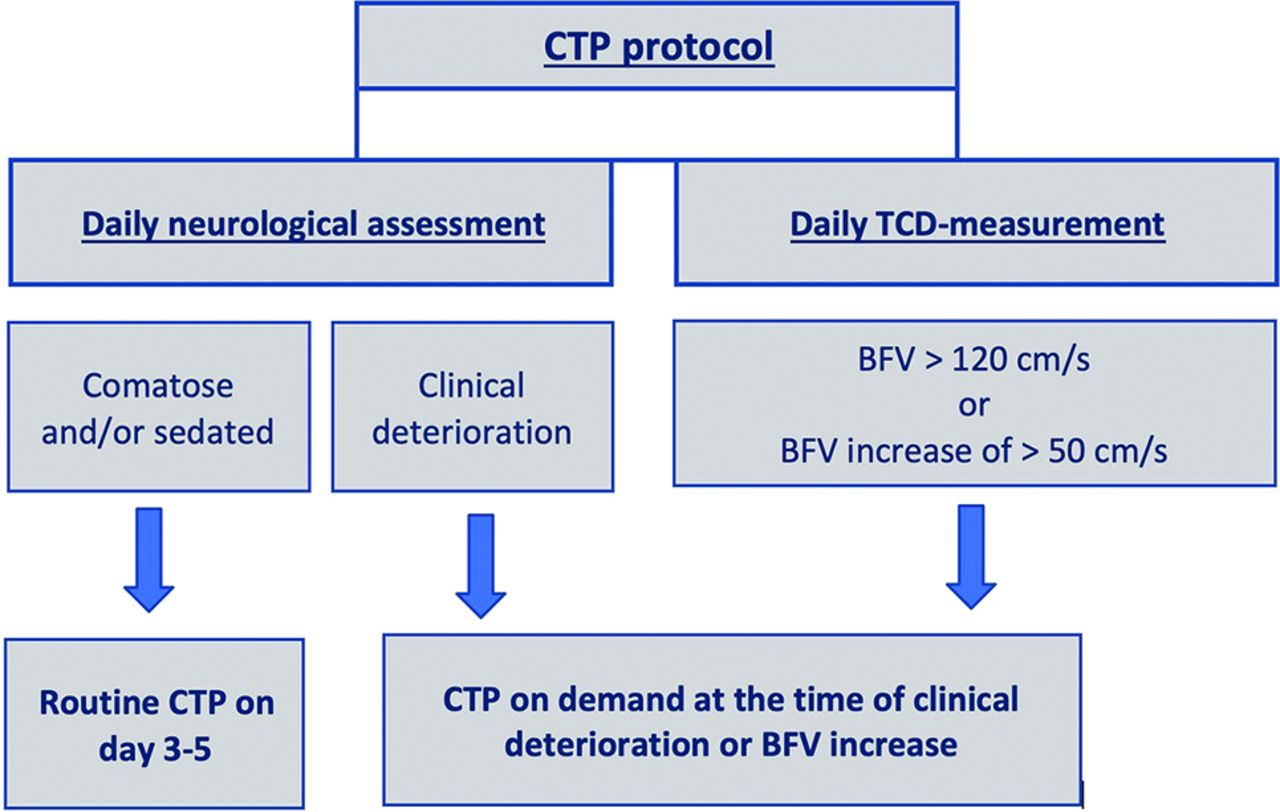
In 2012, a CTP-based imaging protocol was elaborated for the management of patients with aSAH.5 CT combined with CTA and CTP was performed routinely in all comatose/sedated patients on days 3–5 after the bleeding event. Additionally, CT, CTA, and CTP were performed in cases of delayed ischemic neurologic deficits (DIND) or TCD vasospasm and in case of an increase in the velocity acceleration of blood flow of >50 cm/s within 24 hours (Fig 1). The CTP parameters were analyzed qualitatively and quantitatively using cutoff values that have been previously published elsewhere.6 Whole-brain volume CTP data were generated on a 128-section multidetector CT scanner (Definition AS+; Siemens). The acquisition of images was initiated 4 seconds after a bolus of contrast medium, iopamidol (Imeron 400; Bracco) was injected (36 mL of contrast medium with a flow rate of 6 mL/s followed by 36 mL of saline solution with a flow rate of 6 mL/s). For CTP, we used the following parameters: tube settings = 80 kV; 200 effective mAs; rotation time = 0.6 seconds; maximum pitch = 0.5; collimation = 32 × 1.2 mm; scan time = 45.0 seconds; scan length = 84 mm; volume CT dose index = 218.99 mGy; dose-length product = 2505 mGy × cm; effective dose = 5.3 mSv.

Flow chart of the CTP protocol. BFV indicates blood flow velocity.
CTP was used to detect “tissue at risk,” to diagnose hemodynamically relevant vasospasm, and to initiate treatment (ie, induced hypertension). In case of refractory hemodynamically relevant severe vasospasm, ERT was additionally performed.
Definition of Primary End Points
TCD vasospasm was defined as an increase in blood flow velocity of >120 cm/s. DIND were defined as new focal or global neurologic deterioration in unsedated or comatose patients if other possible causes could be excluded. Delayed infarction was defined as newly diagnosed infarction on CT after excluding treatment-associated infarction. The incidence of delayed infarction as well as the extent of infarction (small infarctions versus large territorial and/or multiple infarctions) was evaluated. The functional outcome was assessed according to the mRS 3 months after ictus. Good outcome was considered mRS ≤ 2. The effective radiation exposure was calculated by summing the radiation doses of every examination performed with ionizing radiation and was converted to millisieverts. The effective dose for the DSA was calculated by applying the following equation: Effective Dose (mSv) = DAP (dose-area product) (mGy × cm2) × Conversion Factor (mSv/mGy × cm2). We applied a commonly used conversion factor for DSA of 0.087 mSv (Gy × cm2)-1: https://www.iaea.org/resources/rpop/health-professionals/interventional-procedures/radiation-doses-in-interventional-fluoroscopy#5. The effective dose of CTP can differ depending on the scanner parameters. Thus, we calculated the effective dose of CTP on the scanner at our department of neuroradiology by means of the CT Expo software (http://sascrad.com/information/downloads/).11
Statistical Analysis
The statistical analyses were performed by means of GraphPad Prism software (Version 8; GraphPad Software). The normality of the data was evaluated using data-distribution tests. Nonparametric tests (Mann-Whitney U test) were applied for the analysis of non-normally distributed data, and a t test was used for normally distributed data. For the presentation of baseline data, descriptive statistics and frequency distribution analysis were performed. Multivariate linear regression analysis was performed to identify independent predictors.
RESULTS
A total of 133 patients were enrolled in the study, of whom 57 patients were included in group 1 and 76 patients in group 2. The mean age of the patients was 53.9 (SD, 18.8) years (range, 21–86 years); 68.4% (91/133) of all included patients were women. A good World Federation of Neurosurgical Societies (WFNS) grade (I–III) was found in 52.6% (70/133), and a good Fisher grade (1–2), in 11.3% (15/133) of the patient population. The baseline characteristics of both patient groups are summarized in Table 1, showing no significant differences between the patient populations.
Baseline characteristics in both patient groups
Imaging Findings
Several differences could be detected between the groups with regard to the radiologic examinations performed. Expectedly, CTP was significantly more frequently performed in group 2 compared with group 1 (mean number of CTPs in group 2 = 1.3 [SD, 1.2], ranging from 0 to 5 compared with 0.5 [SD, 0.9], ranging from 0 to 4 in group 1; Mann-Whitney U test, P < .001). CTA was also more frequently performed in group 2 compared with group 1 (mean number of CTAs = 1.9 [SD, 1.1], ranging from 0 to 5 in group 2 compared with 1.1 [SD, 0.8], ranging from 0–3 in group 1; Mann-Whitney U test; P < .001). The first CTP was, on average, performed on day 8 after bleeding (mean, 8.2 [SD, 3.5] days, ranging from 2 to 14 days) in group 1 and on day 4 (mean, 4.1 [SD, 2.3] days, ranging from 3 to 12 days) in group 2. Diagnostic DSA was, however, more frequently performed in group 1 than in group 2 (mean number of DSAs in group 1 = 1.2 [SD, 0.7], ranging from 0 to 3 compared with 0.8 [SD, 0.6], ranging from 0 to 2 in group 2; Mann-Whitney U test, P = .0005). Most interesting, nonenhanced CT scans were also significantly more frequently performed in group 1 compared with group 2 (mean number of CT scans = 5.5 [SD, 3.7], ranging from 1 to 25 in group 1 compared with 4.4 [SD, 1.9] ranging from 2 to 10 in group 2; Mann-Whitney U test, P = .03). Despite these differences, we found no significant difference in the mean cumulative radiation exposure (25.5 [SD, 14.3] mSv in group 1 versus 25.8 [SD, 19.2] mSv in group 2; Mann-Whitney U test, P = .92) between the 2 groups. The mean calculated effective dose for DSA in our study was 7.8 (SD, 2.4) mSv. The calculated effective dose for CTP in our study was 5.3 mSv.
Primary End Points
TCD vasospasm was detected in 58% (33/57) in group 1 and in 51% (39/76) in group 2 (Fisher exact test, P = .46). DIND developed in 8.8% (5/57) of the patients in group 1 compared with 19.7% (15/76) of the patients in group 2 (Fisher exact test, P = .09). The incidence of ischemic complications is shown in Fig 2. Induced hypertension was performed in 50.9% of the patients in group 1 and in 51.3% of the patients in group 2. ERT for the treatment of refractory, severe vasospasm was significantly more often performed in group 2 (ERT in group 2 in 15.8% [12/76 patients] and in 8.8% [5/57 patients] in group 1; Mann-Whitney U test, P = .004). In group 1, four patients underwent angioplasty alone and 1 patient had a combination of angioplasty and nimodipine. In group 2, five patients had angioplasty, 3 patients received intra-arterial nimodipine alone, and 4 patients had both. In those with DIND, only 1 of the 5 patients underwent ERT in group 1, which improved after ERT. In group 2, six patients with DIND underwent ERT, of whom 5 patients improved after ERT and 1 patient had permanent deficits despite ERT. Delayed infarction was detected in 19.3% (11/57) in group 1 and in 15.8% (12/76) in group 2 (Fisher exact test, P = .64).

Incidence of vasospasm and ischemic complications in both groups, showing no significant difference for either DIND or delayed infarction.
Considering the extent of infarction, large territorial and/or multiple infarctions were statistically significantly more frequently detected in group 1 (88.8% of all delayed infarctions) compared with group 2 (33.3% of all delayed infarctions, Fisher exact test, P = .03) (Fig 3). In group two, 58% of patients undergoing ERT had no infarction and 42% developed delayed infarction despite ERT, of whom only 1 patient had multiple territorial infarctions. In group one, 60% of the patients undergoing ERT developed multiple and/or territorial delayed infarction and 40% had no infarction. The functional outcome of the patients in group 2 (median mRS at 3 months = 1, interquartile range = 0–3.8) was statistically significantly better compared with the patients in group 1 (median mRS at 3 months = 3, interquartile range = 0–6; Mann-Whitney U test, P = .005) (Fig 4). In the multivariate analysis, independent predictors of good functional outcome were younger age (P < .001), lower WFNS grade (P < .001), the absence of delayed infarction (P < .001), and treatment according to the CTP protocol (P < .001). The results of the multivariate analysis are summarized in Table 2. A lower WFNS grade (P = .01) and treatment according to the CTP protocol (P = .03) were the only independent predictors of large territorial and/or multiple infarctions in a multivariate analysis, including well-known predictors in the analysis such as Fisher grading, WFNS grading, DIND, ERT, and CTP protocol (Table 3).

Examples of large territorial and multiple infarctions (A and B) and smaller infarctions affecting only a part of a vessel territory (C and D).

Comparison of functional outcome (mRS at 3 months’ follow-up) showing significantly better functional outcome in group 2 compared with group 1 (Mann-Whitney U test, P = .0005).
Multivariate analysis for prediction of functional outcome at 3 months’ follow-up
Multivariate analysis for prediction of delayed, large territorial and/or multiple infarctions
DISCUSSION
The case fatality of aSAH has decreased by 17% during the past 3 decades, and the functional outcome of the survivors of aSAH is continuously improving due to advances in diagnostics and treatment of impending complications after the bleeding.3,12 Because aSAH affects younger patients compared with other stroke types, the aspired goal is to increase the proportion of patients reaching full functional recovery with no or minimal long-term disability. Pursuing the goal of early DCI prediction and detection, which, if left untreated, results in infarctions and long-term disability, we implemented, in 2012, an elaborated CTP-based protocol in addition to the institutional standards for aSAH management.5,13 In the present study, we have evaluated the impact of that CTP-based protocol on functional outcome, comparing 2-year treatment periods before and after the adoption of the protocol. We have chosen the same 2-year interval before and after the protocol implementation to reduce bias introduced by a longer study period (eg, technical advancements in ERT, experience of the neuroradiologist and neurosurgeon), thereby accepting lower patient numbers. The data consistency could be confirmed by comparing the baseline characteristics and excluding significant differences between the 2 patient groups.
Ischemic Complications and Functional Outcome with and without CTP Protocol
The proportion of patients reaching a better outcome was significantly higher in the patient group treated according to the predefined protocol. Several previously published studies reported on the early prediction of functional outcome after aSAH by CTP, which allowed the possibility of influencing the outcome by initiating further measures for preventing permanent neurologic disability.14-16 Delayed infarction is one of the strongest contributors to permanent disability after aSAH, which was earlier shown to be predictable by early CTP.17⇓⇓-21 Although the incidence of delayed infarction in our study was higher in the patient group treated without a predefined protocol, the difference was not statistically significant. However, the proportion of large, territorial, and/or multiple infarctions was significantly higher among the patients treated before the protocol implementation, possibly explaining the worse outcome in this patient group. Additionally, ERTs were significantly more frequently indicated after the protocol adoption. A more reliable identification of patients requiring ERT might be the reason for preventing large territorial and/or multiple infarctions in the patient group treated according to the predefined CTP protocol and, hence, might have contributed to a better outcome in this treatment group.
Similar results were recently published by Omoto et al,22 who reported that CTP routinely performed between days 5 and 9 after ictus was an effective measure for indicating ERT. However, the number of patients receiving ERT in our study was too small to allow conclusions concerning its effectiveness. Furthermore, the role of ERT has not yet been ultimately defined, and indication criteria are yet to be established. Expectedly, we found different practices when indicating further radiologic examinations by comparing both treatment groups. While CTP and CTA were more frequently scheduled after the CTP protocol implementation, the number of diagnostic DSA and CT scans significantly decreased, indicating a more targeted indication for DSA in patients who might require ERT as well. When we took into account the invasiveness of DSA and the mostly higher radiation exposure associated with DSA compared with CTP, this approach seems to be more targeted to the management of patients with aSAH by acquiring direct information about the cerebral perfusion and not only cerebral vasospasm. Although DSA remains the criterion standard, the combination of CTA and CTP has been shown to be a valid noninvasive alternative to DSA for the diagnosis of vasospasm.23-25
The differences in the use of radiologic examinations, however, might also be the reason why the calculated cumulative radiation exposure did not significantly differ between treatment groups, despite the increased use of CTP. CTP is associated with relevant radiation exposure, which has to be considered while elaborating CTP-based treatment protocols. Effective radiation doses ranging from 3.8 to 22.1 mSv have been calculated for CTP, varying depending on the tube voltage.26 A meticulous risk-stratification of patients is necessary to allow a more targeted indication for performing CTP.27 While the value of TCD for detection of cerebral vasospasm is well-established, its role in diagnosing symptomatic vasospasm is rather controversial.28,29 TCD alone (blood flow velocity > 120 cm/s) has a low sensitivity of only 63% for identifying patients at risk for developing DCI.29 Therefore, a combination including additional imaging such as CTP is useful to facilitate a more reliable identification of patients at risk for DCI.5 A clinical evaluation and TCD were used to better identify patients at risk for DCI in whom CTP was indicated, and routine CTP was performed only in comatose and/or sedated patients. Ditz et al21 followed a similar approach, analyzing CTPs performed in unconscious patients with aSAH and found that CTP could identify DCI-related hypoperfusion but could not prevent all delayed infarctions in this population. The CTP protocol could not prevent all delayed infarctions in our study but was associated with smaller infarctions compared with the patient population treated before the protocol adoption. The findings of our study support the concept of elaborating imaging protocols in patients with aSAH, providing direct information about cerebral perfusion and allowing a more targeted treatment-planning, which ideally might result in a better outcome. Further evaluation of CTP protocols with regard to the indication for further diagnostics and treatment is needed, applying a prospective study design to better use the information about cerebral perfusion gathered by CTP.
Limitations of the Study
A limitation of the study is the retrospective nature, with the resulting shortcomings leading to the small number of included patients because of incomplete data availability before 2010. Due to the retrospective data acquisition, we cannot exclude individual decision-making for performing ERT in some patients. The effectiveness of ERT is considered a confounder because the indication for ERT was consistently based on the CTP findings in group 2, whereas the decision to perform ERT in group 1 was made individually and CTP was only performed sporadically. The improvement of ERT techniques across time might have impacted the functional outcome as well. Cognitive impairment was not considered during the evaluation of patients’ outcomes, another limitation of the study.
CONCLUSIONS
The findings of the study suggest that implementation of an elaborated CTP protocol is associated with a better outcome. An earlier identification of patients with impending DCI and early initiation of further diagnosis and treatment, with prevention of large territorial and/or multiple infarctions, might have led to this finding. An elaborated CTP protocol might be a suitable measure for a more reliable ERT indication, which has to be addressed in a prospective study.
Footnotes
Disclosures: Veit Rohde—UNRELATED: Other: Advisory board for BBraun Ausculap, Tuttlingen, Germany, until 2018, Comments: payment of travel expenses. Expert Testimony: Deutsche Forschungsgesellschaft (DFG), ongoing, Comments: no payment; Payment for Lectures Including Service on Speakers Bureaus: Ulrich, Ulm, Germany, until 2018, Comments: €500. Dorothee Mielke—UNRELATED: Board Membership: Advisory Board Member for Medtronic; Consultancy: review doctoral thesis/professor at the Universities of Oslo and Geneva.
References
- Received March 25, 2021.
- Accepted after revision July 3, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Bedside three-dimensional acoustic angiography and perfusion imaging for early detection of delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage: A Feasibility study
- The Complementary Role of CT Perfusion and Transcranial Doppler in the Assessment of Delayed Cerebral Ischemia after Aneurysmal SAH