
Abstract
BACKGROUND: Arterial perforation is a potentially serious complication during endovascular thrombectomy.
PURPOSE: Our aim was to describe interventional approaches after arterial perforation during endovascular thrombectomy and to determine whether reperfusion remains associated with favorable outcome despite this complication.
DATA SOURCES: Data from consecutive patients with acute stroke undergoing endovascular thrombectomy were retrospectively collected between 2015 to 2020 from a single-center cohort, and a systematic review was performed using PubMed, EMBASE, and Ovid MEDLINE up to June 2020.
STUDY SELECTION: Articles reporting functional outcome after arterial perforation during endovascular thrombectomy were selected.
DATA ANALYSIS: Functional outcomes of patients achieving successful reperfusion (TICI 2b/3) were compared with outcomes of those with unsuccessful reperfusion in our single-center cohort. We then summarized the literature review to describe interventional approaches and outcomes after arterial perforation during endovascular thrombectomy.
DATA SYNTHESIS: In our single-center cohort, 1419 patients underwent endovascular thrombectomy, among whom 32 (2.3%) had vessel perforation and were included in the analysis. The most common hemostatic strategy was watchful waiting (71% of cases). Patients with successful reperfusion had a higher proportion of favorable 90-day mRS scores (60% versus 12.5%; P = .006) and a lower mortality rate (13.3% versus 56.3%, P = .01) than patients without successful reperfusion. Thirteen articles were included in the systematic review. Successful reperfusion also appeared to be associated with better outcomes.
LIMITATIONS: Given the low number of published reports, we performed only a descriptive analysis.
CONCLUSIONS: Arterial perforation during endovascular thrombectomy is rare but is associated with high mortality rates and poor outcome. However, successful reperfusion remains correlated with favorable outcome in these patients.
ABBREVIATIONS:
- EVT
- endovascular thrombectomy
- IQR
- interquartile range
- mTICI
- modified TICI
- sICH
- symptomatic intracerebral hemorrhage
Endovascular therapy (EVT) is the standard of care for the treatment of patients with acute ischemic stroke due to large-vessel occlusion.1 Technologic advances have allowed development of new devices that have greatly improved the efficacy and safety of EVT compared with older-generation tools.2 Despite these improvements, as well as greater comfort and expertise among interventionalists across time, the procedure is still not exempt from severe complications.3,4 Arterial perforation, defined as contrast extravasation noticed during a procedural angiographic run, is one of the most serious and feared complications during EVT because it has been associated with poor functional outcomes and death.5 In large EVT trials, the rate of procedural arterial perforations varied between 0.6% and 4.9%.1
When a vessel perforation occurs, some operators might be tempted to abort the procedure, with the risk of leaving the culprit occlusion untreated. Others may decide to pursue EVT once hemostasis is achieved, risking further arterial wall damage. However, little is known regarding the best approach when facing an arterial perforation during EVT and whether reperfusion still represents a reasonable goal in the context of such a complication.5
Therefore, we aimed to describe rescue therapies, management, and clinical outcomes after intraprocedural arterial perforation during EVT, and we sought to determine whether reperfusion is still associated with favorable outcome in this setting.
MATERIALS AND METHODS
This single-center observational study retrospectively analyzed clinical and imaging data prospectively gathered from a quality-improvement database: the Montreal Neurovascular and STrokE Repository (MONSTER), maintained by a high-volume comprehensive stroke center in Montreal, Canada (Center Hospitalier de l’Université de Montréal).
Patient Population
All consecutive adult patients (18 years of age or older) treated with EVT for a large-vessel occlusion between March 1, 2015, and December 31, 2020, in whom arterial perforation occurred during EVT were included. Patients were included when an arterial perforation, defined as contrast extravasation noticed during a procedural angiographic run, was reported in radiology reports or clinical notes. Baseline demographics, stroke characteristics, and procedural details were collected, including information regarding the procedural technique, location of arterial occlusion, type of devices used (stent retriever, contact aspiration, and combined technique), number of passes, procedural duration, and the adopted rescue therapy after vessel perforation. All angiograms were reviewed by 2 interventional neuroradiologists (D.R. and B.M.). We then performed a descriptive analysis of the main steps undertaken after arterial perforation was observed.
Outcomes
Patients were divided in 2 groups with either successful reperfusion or unsuccessful reperfusion to correlate the angiographic results with functional outcomes. Successful reperfusion was defined as a modified TICI (mTICI) ≥ 2b on the final intracranial run. Favorable functional outcome was defined as an mRS score of 0–2, as determined by a certified assessor at 90-day telephone or in-person follow-up. Proportions of hemorrhagic transformation, symptomatic intracerebral hemorrhage (sICH, defined as any hemorrhagic transformation associated with a 4-point increase in the baseline NIHSS score6), and death at 90 days were also collected. All patients had immediate brain imaging following the end of their procedure (plain CT or DynaCT [Siemens] in the angio suite) and a 24-hour follow-up CT. The 24-hour CT was used to identify hemorrhagic transformation to better distinguish true hemorrhagic transformation from contrast staining.
Systematic Review of the Literature
We also performed a systematic review to identify articles reporting on outcomes of patients with acute ischemic stroke with arterial perforation during EVT. With the help of a medical librarian having expertise in systematic reviews (B.N.), we searched the PubMed database, EMBASE database, and Ovid MEDLINE with search terms including “perforation,” “complication,” “stent retriever,” “contact aspiration,” “thrombectomy,” and “stroke” (see the Online Supplemental Data for the full search strategy). We included any study published between January 1, 2015, and June 30, 2020, specifically describing functional outcomes of patients who had arterial perforation observed during EVT. This date range was used to capture studies primarily completed in the modern EVT era. We selected only the references that met all of the following criteria: full-text articles in French or English, studies reporting 3-month clinical outcomes using the mRS score, and studies of patients with stroke undergoing EVT with a procedural arterial perforation. Using a free Web-based application,7 two reviewers (C.D., G.J.) independently screened all titles and abstracts. Full texts were obtained for any article considered relevant for the research question. Disagreements about eligibility were resolved by consensus. Data collection was completed by one author (C.D.) and reviewed by a second (G.J.). Collected data for each study included, when available, the following: baseline NIHSS score, thrombus location, ASPECTS, intravenous thrombolysis, type of anesthesia, EVT technique (stent retriever, contact aspiration, and a combined technique), mTICI score, causes of perforation, sICH, mRS score, and death at 90-day follow-up. The review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.8
Statistics
Differences between groups were tested using the χ2 test of independence or the Fisher exact test for categoric variables and the Mann-Whitney U test for continuous variables. We described the population according to reperfusion status. Reperfusion status was dichotomized as either successful reperfusion (mTICI ≥ 2b) or unsuccessful reperfusion (mTICI < 2b). The statistical level of significance was set at P < .05. Data were analyzed using SPSS (Version 26.0.0.1; IBM). Given the expected low number of previously published reports, we did not plan to perform a statistical meta-analysis of the systematic review results and only performed a descriptive analysis.
The study was approved by our local institutional ethics board for retrospective data collection and review (project No. 20.028). The data supporting the findings of this study are available on reasonable request by a qualified investigator to the corresponding author.
RESULTS
From March 1, 2015, to December 31, 2020, a total of 1419 patients underwent EVT for acute ischemic stroke in our comprehensive stroke center, among whom 32 (2.3%) experienced a vessel perforation during EVT and were included in the study. The annual proportion of EVT procedures complicated by a perforation appeared to decrease during the study period (Online Supplemental Data). Follow-up at 90 days was unavailable for 1 (3%) patient. Baseline demographics and stroke characteristics are shown in the Online Supplemental Data.
Procedural Details
We extracted data from radiology reports and review of source angiographic images, though only 29 complete angiographic studies were available for analysis.
Endovascular thrombectomy was performed with the patient under general anesthesia in 5 patients (15.6%) (including 2 cases with conversion to general anesthesia after arterial perforation), under conscious sedation in 12 patients (37.5%), and under local anesthesia only in the remaining 15 patients (46.9%). The median number of device passes was 1 (interquartile range [IQR], 0–1.75). Vessel perforation occurred more often with the use of a microwire (n = 14, 43.8%) than with a microcatheter (n = 9, 28.1%). The cause of vessel perforation was unknown in the remaining 9 patients (28.1%) (Online Supplemental Data.). Patients with perforation due to a microwire had numerically better 3-month outcomes than patients with microcatheter perforation (6/14 patients, 46.2%, versus 3/9 patients, 33.3%, respectively).
After review of available angiograms, we found that 16 patients had a perforation identified only on microcatheter injection (16/29; 55.2%), 13 patients (44.8%) had a perforation noticed after ICA injection, and 13 patients (44.8%) had a perforation viewed on multiple runs. Outcomes of these patients were similar regardless of how perforation was identified or the number of runs on which the perforation was viewed (Online Supplemental Data).
Most intraprocedural vessel perforations occurred at a distal location: the MCA M2 in 18 patients (56.3%) and the anterior cerebral artery in 3 patients (9.4%). The remainder occurred proximally: the MCA M1 in 7 patients (21.9%) and the ICA in 2 patients (6.3%). Among patients with proximal perforation (ICA and M1), rescue therapy was performed in 4/9 patients (intermittent balloon inflation in 2 patients and parent vessel occlusion in 1 patient). In the last case, the microcatheter was left in place and cut and sewn at the groin in an attempt to seal the intracranial arterial perforation point. Contrast extravasation stopped spontaneously in the 5 remaining cases (Fig 2). Among patients with distal perforation, contrast extravasation was self-resolving in most (17/22 patients), parent vessel occlusion was performed in 4 cases, and intermittent balloon inflation was performed in the last case. “Self-resolving” is defined as contrast extravasation stopping without a specific intervention. The median number of runs before concluding that a bleed was self-resolving was 1 (IQR, 1–2).
Outcomes and Association with Reperfusion
Of 31 patients with an available 90-day mRS, 11 (34.4%) patients had favorable outcomes and 11 (34.4%) patients died (5 sICH, 3 cases of malignant edema, 2 cases of aspiration pneumonia, and 1 from multiple causes).
Reperfusion (mTICI 2b/3) was successful in 16 (50%) patients and unsuccessful in 16 (50%) others, with baseline characteristics being similar in these 2 groups (Online Supplemental Data).
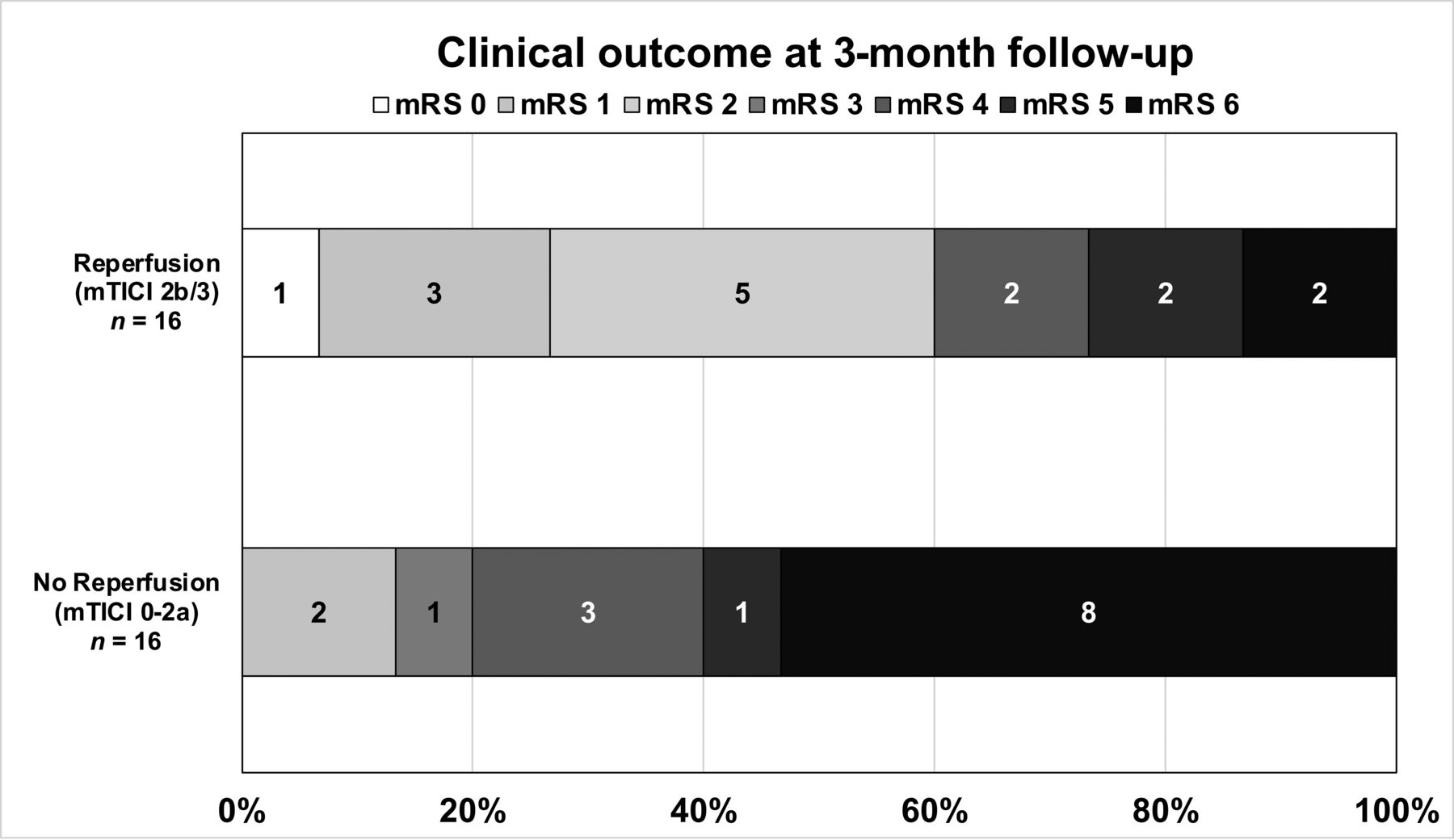
As shown in Fig 1, patients with successful reperfusion had a higher proportion of favorable functional outcomes at 90 days than patients without successful reperfusion (60% versus 12.5%, P = .006) as well significantly lower mortality rates (13.3% versus 56.3%, P = .01) (Table).

The mRS score distribution at 90 days for patients with successful reperfusion (TICI 2b/3) and no reperfusion (TICI 0-2a), despite vessel perforation during endovascular thrombectomy.

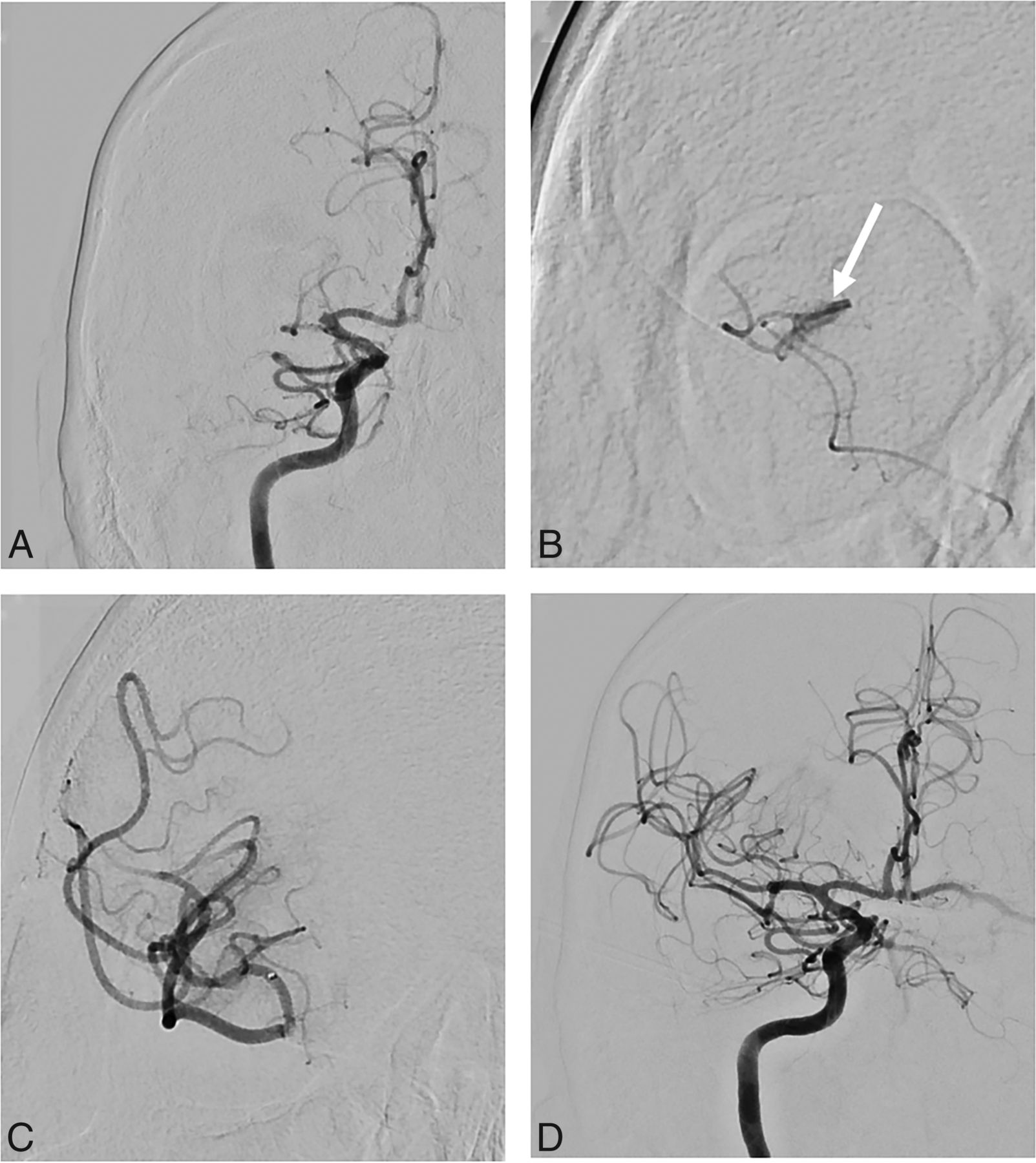
Illustrative case. A 69-year-old man with a proximal right MCA occlusion (A). B, After catheterization of M1, contrast extravasation (white arrow) was identified on microcatheter injection. C, After 10 minutes, contrast extravasation stopped spontaneously. D, Thrombectomy was pursued without further complications, and successful reperfusion was achieved. The patient had a favorable outcome at 3 months (mRS 1).
Outcomes of patients with procedural perforation with successful reperfusion (mTICI ≥ 2b/3) and with unsuccessful reperfusion (mTICI < 2b/3)a
Among patients with successful reperfusion, vessel perforation occurred before achieving reperfusion in 13 cases (13/16, 81.3%) and after achieving reperfusion in 3 cases (18.7%). In these last 3 cases, a secondary medium vessel occlusion (A2 and M3) was targeted and recanalized, despite a reperfusion status of ≥TICI 2b.
Among patients with unsuccessful reperfusion, the procedure was aborted after vessel perforation in 5 patients, while in the remaining 11 cases, the procedure was stopped because of failure to achieve successful recanalization. Among these patients, 9 had unsuccessful thrombectomy despite several passes and 2 patients had persistent distal emboli.
Patients with self-resolving bleeding did not have a greater proportion of favorable outcomes than patients needing hemostatic intervention (14/23 patients [60.9%] versus 6/9 patients [66.7%]).
Intracerebral Hemorrhage
The median delay between the groin puncture and control imaging was 18 hours (IQR, 13–24 hours). One patient died within 24 hours before any follow-up imaging was performed. All patients had an SAH on their 24-hour CT. Intraparenchymal hemorrhage of any type occurred in 14 patients (37.5%), of whom 6 (18.8%) had sICH (Table). Among patients with sICH, 4 patients had a distal perforation (distal M2, M3, or A2) and 2 patients had a proximal perforation (M1 segment).
Systematic Review
The initial literature search yielded 6052 articles. After all titles and abstracts were screened by C.D. and G.J., 5969 articles were considered irrelevant. Of the remaining 83 articles, 70 were excluded for incorrect outcome assessments, wrong population, wrong study design, and wrong publication type (abstract only, language other than French or English), leaving a total of 13 studies eligible for analysis (n = 37 patients; Online Supplemental Data: PRISMA diagram). Eight studies were cohort studies, and 5 were case reports (Online Supplemental Data). The median baseline NIHSS score was 14.5 (IQR, 11.75–19). A stent retriever was used in most cases (28/37 cases); contact aspiration, in 13/37 cases; and combined therapy, in 1 case. Nine patients had multiples passes using different techniques. Vessel perforation occurred more often in distal branches (16/37 cases; 43%), while 14 patients (38%) had proximal vessel perforation, and the exact location was not detailed in the remainder.
In most cases (23/37, 62%), the cause of vessel perforation was not described. For those in whom the cause was mentioned, 9 patients (24%) had vessel perforation due to a microwire; 4 patients (11%), due to a microcatheter; and 1 patient (0.03%), due to a strong contrast injection. Different hemostatic strategies were described for 26 patients: 1) procedural abandonment without any additional maneuver despite a persistent intracranial occlusion (7 cases); 2) inflation of an intracranial balloon (8 cases); 3) parent vessel occlusion using coils or glue (6 cases); or 4) watchful waiting (no intervention performed because of spontaneous regression of bleeding) in 2 cases. In 1 case, despite inflation of an intracranial balloon catheter, bleeding persisted, and therapeutic occlusion using coils was performed.
In all studies included in this literature review, the functional outcome at 3 months was available for 35 of 37 patients. The outcomes were poor (median mRS, 6 [IQR, 2.5–6]): Only 9 patients (9/35, 26%) had a favorable outcome (mRS, 0–2) at 3 months, and mortality was high (20/35 cases, 57%). Both reperfusion status and outcome at 3 months were available for 34 patients. Although formal statistical analysis was not possible due to an overall paucity of data in the published reports, the median mRS appeared slightly better in patients with successful reperfusion (median mRS, 5; IQR, 2–6, versus 6; IQR, 4–6) as did mortality, which was numerically lower in these patients (7/14, 50%, versus 13/20, 65%).
DISCUSSION
Our findings demonstrate that vessel perforation in the context of EVT for acute stroke is infrequent but may result in a high rate of mortality and poor functional outcome. In our series, the proportion of patients having this complication was similar to that reported in recent EVT randomized trials (0.6%–4%), registries,1,4 and a previous cohort study by Mokin et al5 (1%). However, our results suggest that patients might, nevertheless, do better despite perforation if successful reperfusion is achieved.
Vessel perforation is arguably one of the most serious and feared complications during EVT and is associated with high rates of mortality.3⇓-5,9,10 The risk of vessel perforation is increased during ‘‘blind maneuvering’’ while trying to gain access to occluded intracranial vessels with a microwire or microcatheter11⇓⇓⇓⇓⇓-17 and while withdrawing a stent retriever.5,18,19
Vessel perforation tends to involve more distal vessel segments: 65% of cases in our study and 61% in our literature review. This finding is particularly relevant because the field is moving toward more aggressive recanalization of distal vessel occlusions,20 with upcoming trials evaluating the role of EVT in such patients (NCT05029414). However, the clinical impact of distal perforation might be less severe than that of proximal perforation (ICA or M1). In our cohort, rescue therapy was performed more often in patients with proximal perforation, but outcomes were similar regardless of perforation site.
It is usually thought that intraprocedural vessel perforation requires immediate action to achieve hemostatic control, such as blood pressure reduction and/or the interruption or reversal of any ongoing thrombolytic agent or blood thinners,10 temporary intracranial balloon occlusion,5,16 or parent vessel occlusion by injection of either liquid embolic agents16,21 or detachable coils.10,22 These maneuvers were used in most patients found in our systematic review, other than cases in which the procedure was simply aborted prematurely. However, in our cohort, most cases of contrast extravasation resolved spontaneously (71.9%) after the device or microcatheter was withdrawn. In some cases, the offending thrombus itself may provide effective hemostasis when a perforation occurs in the vasculature distal to the occlusion. On the other hand, parent vessel occlusion may potentially result in major stroke with severe disability and could increase the risk of poor clinical outcome and mortality.3,22,23
In our series, as well as in previously published reports, procedural perforations during EVT were associated with overall high mortality rates and low rates of good clinical outcome.5,24 Compared with outcomes found in the major EVT trials1 and in most large EVT registries,25 functional outcomes of patients with vessel perforation remain relatively poor. However, such poor clinical outcomes might be due to the absence of reperfusion26 rather than cerebral hemorrhage. The decision to resume or abort EVT should be based on stroke severity, hemostatic control, technical difficulty, and the safety of pursuing thrombectomy, while always being aware that successful reperfusion appears to be associated with better outcomes and lower mortality in this population.5,27
There are several suspected risk factors for vessel perforation, notably a distal occlusion, the presence of arterial tortuosity, and intracranial atherosclerosis.18 Moreover, some clot types can be more difficult to cross with a microcatheter and microwire, thus increasing the risk of traumatic vessel injury and perforation.5,23 Contact aspiration does not always require crossing the clot with a microcatheter and might intuitively seem safer than stent retrievers in this regard. However, a randomized trial comparing both techniques did not show a significant difference in vessel perforation.28 Some authors have suggested that crossing the clot with a wireless microcatheter may reduce the risk of vessel perforation.29
In our cohort, functional outcome and mortality at 3 months were better than in the literature review. Most studies reporting procedural complications, including vessel perforation, described only severe cases with poor outcomes. Conversely, in our study, we reported all cases of perforation, which could be more representative of real life than smaller series or case reports. Since the widespread adoption of EVT following the major randomized trials,1 the tools and techniques available have continuously improved,2 and in our center, the rate of vessel perforation decreased from 3% in 2015 to 1.6% in 2020.
Despite being a larger cohort than those in previously published reports, our study has several limitations, including its single-center, retrospective design, a relatively small sample size, and the heterogeneity in the management of complications. This last limitation reflects the known variety of practices among neurointerventionalists and stroke physicians regarding the management of vessel perforation during EVT.3,5 Because this complication is, fortunately, rare, the limited number of cases precluded the use of statistical analysis to reliably determine which clinical or technical variables were associated with favorable outcome. We did not assign degrees of severity to the perforations, given the lack of a standardized angiographic definition and because procedural imaging of the perforation varied widely among cases. Finally, the 90-day mRS was assessed by raters who were not necessarily blinded to perforation status, and although performed by certified assessors, the mRS is known to have only fair-to-moderate interobserver reliability.30
CONCLUSIONS
Procedural vessel perforation during EVT is a rare-but-serious complication, associated with high mortality and poor clinical outcome. However, successful reperfusion remains correlated with favorable outcome in these patients and can be pursued when technically safe and feasible.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received February 17, 2022.
- Accepted after revision July 17, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}