
Abstract
BACKGROUND AND PURPOSE: Recent reports suggest an association between dural AVFs and cerebral venous thrombosis. We aimed to investigate the specific temporal and anatomic association between the 2 conditions.
MATERIALS AND METHODS: A consecutive cohort of adult patients with dural AVFs was seen at Amsterdam University Medical Centers (2007–2020). An experienced neuroradiologist re-evaluated the presence and imaging characteristics of dural AVFs and cerebral venous thrombosis on all available imaging. The temporal (previous/concurrent/subsequent) and anatomic (same/adjacent/unrelated venous sinus or vein) association between dural AVFs and cerebral venous thrombosis was determined.
RESULTS: Among 178 patients with dural AVFs, the mean age was 58.3 (SD, 13.2) years and 85 (48%) were women. Of 55 patients (31%) with cerebral venous thrombosis, 34 (62%) were women. Four patients (7%) had cerebral venous thrombosis before the development of a dural AVF, 33 (60%) had cerebral venous thrombosis at the time of dural AVF diagnosis (concurrent), and 18 (33%) developed cerebral venous thrombosis during follow-up after conservative treatment. The incidence rate of cerebral venous thrombosis after a dural AVF was 79 per 1000 person-years (95% CI, 50–124). In 45 (82%) patients with dural AVFs and cerebral venous thrombosis, the thrombosis was located in the same venous sinus as the dural AVF, whereas in 8 (15%) patients, thrombosis occurred in a venous sinus adjacent to the dural AVF.
CONCLUSIONS: One-third of patients with a dural AVF in this study were diagnosed with cerebral venous thrombosis. In almost two-thirds of patients, cerebral venous thrombosis was diagnosed prior to or concurrent with the dural AVF. In 97% of patients, there was an anatomic association between the dural AVF and cerebral venous thrombosis. These data support the hypothesis of a bidirectional association between the 2 diseases.
ABBREVIATIONS:
- CVT
- cerebral venous thrombosis
- dAVF
- dural AVF
- IQR
- interquartile range
Dural AVFs (dAVFs) account for only 10%–15% of intracranial vascular malformations,1 with an estimated incidence rate of 0.15–0.29 cases per 100,000 person-years.2,3 In dAVFs, multiple arteriovenous shunts exist between the meningeal arteries and the intracranial venous system. The most common locations of dAVFs are the sigmoid, transverse, and cavernous sinuses. They may cause relatively benign symptoms such as tinnitus, headache, and dizziness, but in the presence of retrograde flow to the cortical venous system, dAVFs can also cause venous hypertension and/or intracranial hemorrhage, leading to a variety of neurologic symptoms.4
Cerebral venous thrombosis (CVT) is a rare neurologic condition with an incidence rate of approximately 1.32 per 100,000 person-years (95% CI, 1.06–1.61).5 CVT is most frequently seen in adults younger than 50 years of age, and women are affected 3 times more often than men.6,7 Although the clinical presentation is variable, common symptoms include headache, seizures, focal neurologic deficits, and decreased consciousness.8
It is believed that CVT and dAVF have a bidirectional association: CVT can initiate the development of a dAVF, but a dAVF can also cause CVT.1,9 It has been suggested from animal model studies that venous hypertension, through increased levels of vascular endothelial growth factor, plays a key role in the development of dAVFs.10,11 Recent clinical studies and case reports have investigated the association between dAVF and CVT.12⇓-14 In a cohort study of 69 patients with dAVF, 27 (39%) patients were diagnosed with CVT. Among patients with dAVF and CVT in this study, most of the dural sinuses affected by the CVT were directly connected to the dAVFs, indicating a possible spatial association between the 2 diseases.15 The temporal association between dAVF and CVT was not reported in this study. In contrast, another cohort study systematically screened 112 patients 6 months after acute CVT using MRA. The authors did not find any new dAVFs and, therefore, concluded that routine screening for dAVF 6 months after CVT is not recommended.16
The aim of this study was to assess the proportion of patients with dAVFs who had previous or concurrent CVT and to determine the incidence of a new CVT during follow-up in a large, consecutive cohort of patients with dAVF, regardless of treatment strategy. Additionally, we studied the anatomic association between CVT and dAVF in patients with both diagnoses.
MATERIALS AND METHODS
Data will be shared with academic researchers on reasonable request to the corresponding author.
Study Population and Study Design
We conducted a retrospective cohort study on all consecutive adult patients with a radiologically confirmed diagnosis of dAVF seen at the Amsterdam University Medical Centers (location AMC) between January 2007 and October 2020. Patients younger than 18 years of age with direct carotid-cavernous fistulas in whom baseline vascular imaging at the time of CVT or dAVF diagnosis was not available were excluded.
Ethics Approval
For this observational study, the Ethical Committee of the Amsterdam University Medical Centers waived the necessity for formal approval. In accordance with the General Data Protection Regulation, all eligible patients received an information letter about the study with the option of refusing the use of their pseudonymized care data.
Data Collection
Data on demographics, clinical signs and symptoms at the time of dAVF diagnosis, CVT risk factors, and functional outcome were obtained from the electronic medical records. Functional outcome at the last follow-up visit was retrospectively assessed using the mRS.17
An experienced interventional neuroradiologist (R.v.d.B.) re-evaluated all available brain imaging including CTA, MRA, and DSA until the last follow-up for the hemorrhage, CVT, dAVF location, Cognard classification,18 date of dAVF diagnosis, and type of dAVF treatment. With respect to dAVF diagnosis and classification and CVT diagnosis, the findings after re-evaluation were compared with the original radiology report. Treatment of the dAVF was categorized into conservative treatment, endovascular treatment (transarterial or transvenous), neurosurgical treatment, stereotactic radiosurgery, or a combination of therapies. If a patient had multiple dAVFs, each dAVF was assessed separately. In addition, all available neuroimaging was re-evaluated for the presence of previous, concurrent, or subsequent CVT, regardless of the presence of symptoms suspicious for CVT. CVT was defined as acute or subacute when a filling defect was visible in the venous sinus, cortical or superior ophthalmic vein, or as chronic when the appearance of the sinus on vascular imaging showed no flow or was irregular with residual defects in the lumen of the venous sinus or the presence of vascular channels (Fig 1).19

A 44-year-old woman presenting with pulsatile tinnitus due to a Cognard type I dAVF. Selective injection of the external carotid artery (A) shows supply from the middle meningeal artery to the dAVF. The sigmoid sinus shows irregularities due to postthrombotic changes with reopened vascular channels. The venous drainage of the brain (B) is unrestricted through the contralateral side.
Evaluation of Temporal and Anatomic Relation
For patients who were diagnosed with CVT, the location of the thrombosis and the temporal and anatomic association between CVT and dAVF were assessed. The time of the CVT diagnosis relative to the dAVF diagnosis was classified into 1 of 3 main categories: 1) imaging-proved CVT diagnosis before the dAVF diagnosis, 2) CVT diagnosis concurrent with the dAVF diagnosis without prior imaging to assess the sequence of events, and 3) CVT diagnosis after the dAVF diagnosis. The third category was further subdivided into following dAVF treatment and following conservative management of the dAVF.
The spatial anatomic association between the CVT and the dAVF was categorized as having a probable, possible, or unlikely association. These associations are defined as follows: 1) probable, if the dAVF and CVT were located in the same venous sinus or vein, 2) possible, if CVT occurred directly up- or downstream in the adjacent venous sinus or vein in spatial association with the dAVF, or 3) unlikely, if there was no anatomic association. If thrombosis was present in multiple sinuses or veins or if multiple dAVFs were present, an anatomic association was considered probable or possible if at least one of the thrombosed sinuses or veins met the applicable criteria.
Statistical Analysis
Categoric data are shown as frequencies and proportions, and non-normally distributed continuous data (defined as the Shapiro-Wilk statistic of <0.9), as medians with interquartile ranges (IQRs). The Fisher exact test was used to compare categoric variables for patients with dAVFs with and without CVT. A P value of < .05 was considered statistically significant. We calculated the incidence rate (with 95% CI) of CVT after a dAVF diagnosis per 1000 person-years. For this calculation, we included only patients with dAVFs who did not have a previous diagnosis of CVT or a concurrent CVT at the time of the dAVF diagnosis.
RESULTS
Patient Selection
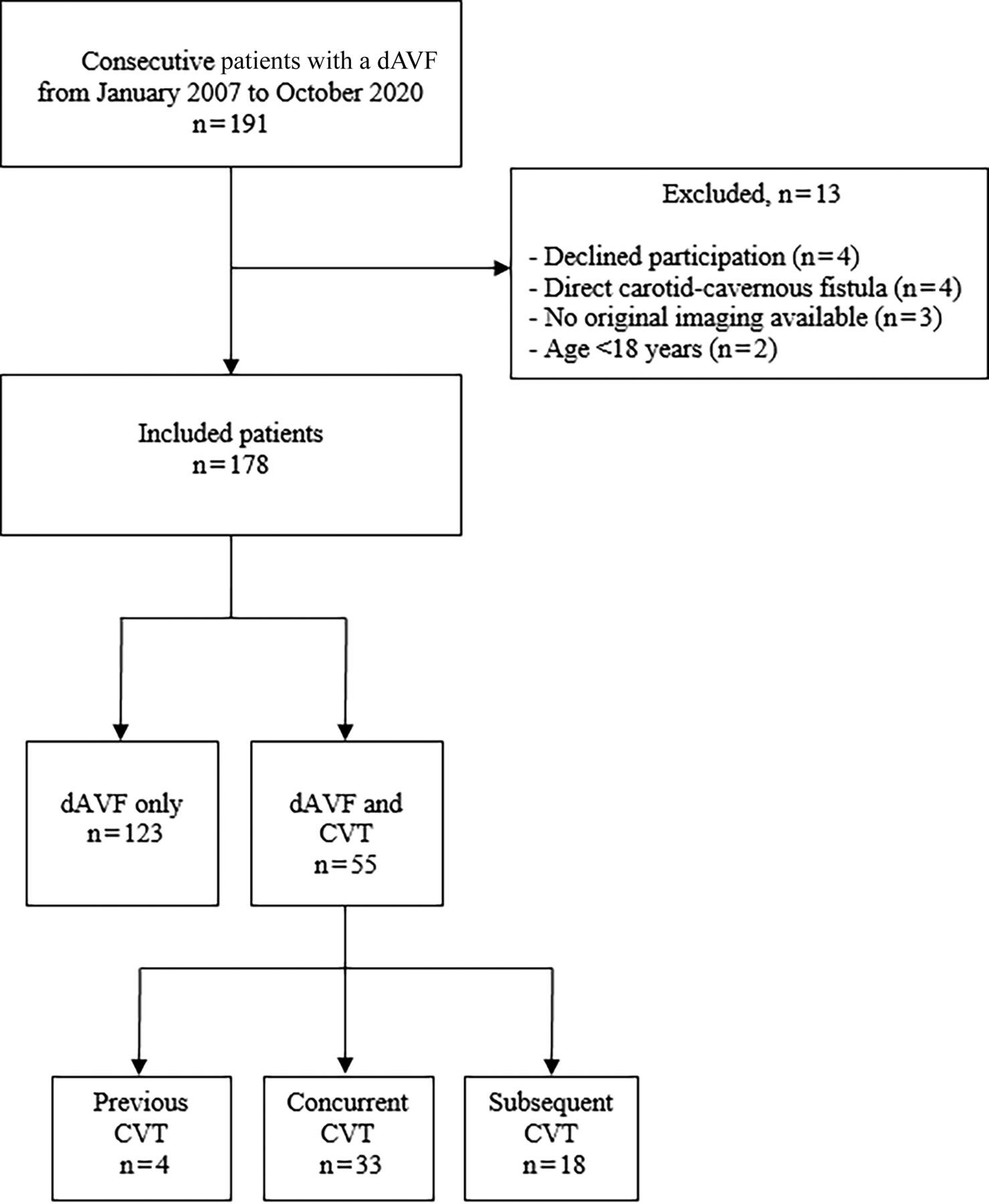
Of 191 eligible patients, a total of 178 patients were included in the study. Four patients declined participation, and 2 patients were excluded because they were younger than 18 years of age at the time of the dAVF diagnosis. Four patients were excluded because they had a direct carotid-cavernous fistula, and 3 referred patients were excluded because the initial cross-sectional imaging at the time of the dAVF diagnosis was not available for re-evaluation (Fig 2).

Flow chart showing patient cohort.
Table 1 provides an overview of the baseline patient characteristics at the time of the dAVF diagnosis. There was a female predominance in the dAVF and CVT group compared with the dAVF-only group (62% versus 42%, P = .010). The mean age was similar in both groups.
Baseline characteristics at time of dAVF diagnosis
Imaging Findings
Of the 178 included patients, 55 patients (31%) showed signs of CVT. In 11 of these 55 patients (20%), the diagnosis of CVT was made after re-evaluation of the imaging. In all 11 patients, CVT-related abnormalities were only visible on DSA.
In 33 (60%) patients with dAVF and CVT, signs of recent or past CVT (with or without partial recanalization) were visible as concurrent findings when the diagnosis of dAVF was made on imaging. Subacute or acute CVT was seen in 4 patients; all CVTs were localized to the superior ophthalmic vein in cavernous sinus dAVF locations. In addition, 29 patients showed signs of chronic thrombosis, in which the sinus was either completely occluded or partially occluded with reopened vascular channels. Only 4 patients (7%) had a confirmed history of CVT before the dAVF diagnosis (Fig 3). Finally, CVT developed secondary to the dAVF in an additional 18 patients (33%) during a median follow-up of 9 months (IQR = 5–24 months). In 11 of 18 patients, CVT occurred after dAVF treatment in the affected sinus or vein. In the other 7 patients (13%), spontaneous occlusion of the dAVF was seen during conservative management. Of these 7 dAVFs, 6 were located at the cavernous sinus region with drainage into the superior ophthalmic vein. Of the treated patients with development of thrombosis, 3 patients (3%) presented with a headache. None of these treated patients with de novo thrombosis had a history of CVT. The incidence rate of CVT after dAVF diagnosis was 79 per 1000 person-years (95% CI, 50–124).

A 19-year-old man with a history of alpha-thalassemia type 2, a carrier of sickle cell disease and ulcerative colitis, underwent imaging because of relapsing headaches. Noncontrast CT shows hyperdensity in the left transverse sinus (A). Sinus thrombosis is confirmed on CT venography (B). One week later, phase-contrast MR venography shows absent flow in the left transverse and sigmoid sinuses without signs of arterialization of the sinuses (C). Persistent thrombosis of the sinus is depicted on SWI (D). Six months later, the patient presented with a pulsatile tinnitus; repeat MR imaging shows partial reopening of the sigmoid sinus (E) but also reveals a dAVF at the left sigmoid sinus (F). One year later, dynamic contrast-enhanced MRA (G) shows restoration of sinus flow and spontaneous obliteration of the dAVF (H).
Patients with CVT more often presented with seizures at the time of dAVF diagnosis (13% versus 3%, P = .014). There was no difference in the presence of thrombotic risk factors between the 2 groups. No significant difference in the hemorrhage rate was seen between the dAVF-only group compared with dAVF and CVT groups (18/123 patients versus 4/55 patients, P = .084).
No changes in the diagnosis or grading of the dAVF were recorded between the original report and findings after re-evaluation. A total of 17 (10%) patients presented with multiple dAVFs (Online Supplemental Data). The most common dAVF locations in the dAVF and CVT group were the lateral sinus (64%) and the cavernous sinus (22%, Online Supplemental Data). In the dAVF-only group, the dAVF was most frequently located in the cortical veins (30%) and the lateral sinus (22%).
Cognard classifications and treatment of the dAVFs are outlined in Table 2. Overall, 178 patients had a total of 201 dAVFs, including 86 (48%) benign (Cognard I and IIa) and 115 (65%) aggressive (Cognard IIb and more) dAVFs. The most frequent dAVF location was the sigmoid and transverse (lateral) sinuses. Among the 59 patients with CVT, a total 73 dAVFs were seen, 37 (51%) classified as Cognard I/IIa, and 11 (15%), as Cognard >III. Among the 119 patients with dAVF-only (no CVT), a total of 128 dAVF were seen, 49 (38%) classified as Cognard I/IIa and 64 (50%) as Cognard >III. Four of 40 patients (10%) with a Cognard IIb or IIa–b classification presented with a hemorrhage; all had CVT. Three of 4 patients had a parenchymal hematoma; all 3 had concurrent CVT. The other patient presented with an SAH due to a ruptured ectatic venous pouch (Cognard IV) and developed progressive thrombosis of the draining vein after treatment. Eighteen of 75 patients (24%) with a Cognard III or more classification presented with a hemorrhage; only 1 of these 18 patients had concurrent CVT. In both groups, endovascular embolization was the most frequent treatment, followed by conservative treatment. Spontaneous occlusion of the dAVF occurred in 23 of 61 (38%) conservatively treated patients. In 7 of these patients, thrombosis of the anatomically linked draining vein or sinus was seen. A higher rate of spontaneous dAVF thrombosis was found among patients with a dAVF in the cavernous sinus (40%) compared with a dAVF in all other locations (9%).
dAVF characteristics
Among the 55 patients with a dAVF and CVT, thrombosis was most frequently seen in the sigmoid (51%) and transverse sinuses (47%; Online Supplemental Data). Most patients with multiple CVT locations had thrombosis in both the sigmoid and transverse sinuses. Table 3 outlines the anatomic and temporal association between dAVF and CVT. Thrombosis in the venous system after treatment (Table 3) was seen after complete occlusion in 4 of 11 patients and after partial occlusion in 7 patients. In 45 (82%) patients, CVT occurred in the same venous sinus as the dAVF (probable anatomic relation). In only 2 (4%) patients was no anatomic association found. The Online Supplemental Data show the clinical presentation in patients who developed CVT during follow-up (after intervention or conservative treatment of the dAVF). Five of 11 patients (46%) who developed CVT following dAVF treatment were asymptomatic. Headache and ocular symptoms were the most common presenting symptoms of subsequent CVT in conservatively treated patients, the latter mostly related to cavernous sinus locations.
CVT characteristics among patients with dAVF and CVT diagnoses
Clinical Outcome
The median time from dAVF diagnosis until the last available follow-up was 9 months in both the dAVF and CVT (IQR = 5–24 months) and dAVF-only (IQR = 5–23 months) groups. None of the included patients had died at last follow-up, and most patients (44 [80%] versus 91 [74%] in the dAVF and CVT and dAVF-only groups, respectively) were functionally independent (mRS 0–2). Figure 4 outlines the mRS scores at last follow-up for patients with a dAVF with and without CVT with benign and aggressive dAVFs, respectively. Functional independence (mRS 0–2) was seen in 89% of the patients with a benign dAVF, compared with 69% of the patients with an aggressive dAVF. Of 22 patients with an aggressive dAVF presenting with a hemorrhage, 14 (64%) had a favorable outcome and 8 had an unfavorable outcome.

A, Last available mRS score in patients with benign dAVFs. Asterisk indicates median follow-up time 16 months (IQR 7–29). There were no patients with mRS 3, 5, or 6. Dagger indicates median follow-up time 9 months (IQR 2–21). There were no patients with mRS 5 or 6. B, Last available score mRS in patients with aggressive dAVFs. Asterisk indicates median follow-up time 8 months (IQR 5–20). There were no patients with mRS 6. Dagger indicates median follow-up time 10 months (IQR 7–27). There were no patients with mRS 6.
DISCUSSION
In this cohort study of 178 consecutive patients with dAVFs, approximately 1 in 3 patients had a previous, concurrent, or subsequent diagnosis of CVT. We found both an anatomic and temporal association between dAVF and CVT. In most patients, CVT was located in the same sinus as the dAVF, and in more than half of patients, CVT and dAVF were diagnosed concurrently.
Several studies have proposed potential mechanisms to explain the association between dAVF and CVT. First, CVT may cause a dAVF due to the angiogenetic activity induced by decreased cerebral perfusion secondary to venous hypertension or by enlarging pre-existing arteriovenous shunts due to elevated venous pressure.9,10 This mechanism has been demonstrated in several animal model studies.10,11,20,21 It can be postulated that the extent of the thrombosis determines the behavior of the dAVF: A more severe thrombosis increases the risk of corticovenous reflux when sinus outflow is no longer available. On the other hand, a dAVF may also precede CVT, especially when the dAVF shows spontaneous occlusion. This sequence of events was confirmed in this study in conservatively managed patients. The proposed mechanism is that venous hypertension and venous stasis caused by dAVFs may cause secondary thrombosis.1 A second possible mechanism is that during the development of a dAVF, the sinus wall thickens, possibly causing stenosis and eventually inducing CVT.22
Previous studies have found venous thrombotic risk factors to be associated with dAVF development.23⇓⇓-26 This finding is inconsistent with our finding that there were no major differences in the occurrence of risk factors for the development of thrombosis in the dAVF-only group compared with the dAVF and CVT group. Our findings are limited because we did not routinely test for inherited or acquired thrombophilia such as Factor V Leiden or elevated homocysteine levels, but these are well-known risk factors.23
In our study, 21% of all patients with dAVFs had previous or concurrent CVT. The incidence rate of CVT during follow-up was 7900 per 100,000 person-years (95% CI, 5000–12,400) in our study versus 1.32 per 100,000 person-years (95% CI, 1.06–1.61) in the general population.5 With a low incidence of dAVF in the population of 0.15–0.29 cases per 100,000 person-years,2,3 besides management of the dAVF, patient care should also focus on CVT risk factors. Thus, the association between dAVF and CVT is more pronounced in patients primarily presenting with a dAVF than in patients presenting initially with CVT. The finding that CVT both precedes and is seen during follow-up of dAVF supports the hypothesis of a bidirectional association between the 2 diseases, and clinicians should be vigilant for CVT among patients with dAVFs. This advice is especially important when the dAVF-affected sinus is occluded for treatment purposes because future contralateral sinus thrombosis can then be a clinically devastating event. Moreover, our data show that the diagnosis of CVT is easily missed on CT and/or MR imaging. Especially in this population at risk for CVT, it is important to look for changes in the venous system on DSA that might indicate previous thrombosis. A clinical clue to CVT in patients with a dAVF is when they present with or have a history of seizures.27
Our finding that CVT was most often located in the same or adjacent venous sinus as the dAVF is in line with a previous cohort study of 69 patients with dAVFs.15 The proportion of patients with dAVFs who had CVT was also similar in our cohort compared with previous cohort studies.15,28 In contrast, the proportion of patients with CVT who had a previous or concurrent dAVF is reported to be only around 1.6%–2.4%.14,29 On the contrary, from another prospective study, no patients with CVT developed a dAVF during follow-up when screened after 6 months.16 We propose that the temporal association between dAVF and CVT might at least be partially location-dependent with a preference for the sigmoid and transverse sinuses and also the cavernous sinus. Progressive occlusion of a dAVF with thrombosis of the venous outlet was more often seen in patients with dAVFs in the cavernous sinus region compared with dAVFs in other locations in our study. This finding might be related to the anatomic disposition of the superior ophthalmic vein, which serves as a major drainage route in most of these dAVFs and has to pass the orbital septum. Because of narrowing of the vein at the orbital septal junction, it can be hypothesized that the focal venous outflow restriction promotes the thrombotic process.
At the last follow-up assessment, most patients in our study had an mRS score of 0–2. In a previous study of 40 patients with dAVFs (including 13 patients with carotid-cavernous fistulas), an mRS score of 0–2 was found in 91% of patients after a mean follow-up of 6.2 years (range, 0.7–14.8 years, with 20% lost to follow-up).30 Although the reason for this difference in functional outcome between our study and the previous study is not entirely clear, our results seem to indicate the important burden of residual symptoms among patients with dAVFs. Further research to better identify optimal treatment strategies for individual patients with dAVF is thus warranted.
To our knowledge, this is the first study to investigate both the anatomic and temporal association between dAVF and CVT in a large cohort of consecutive patients with dAVFs. In all patients, brain imaging was re-evaluated by an experienced interventional neuroradiologist for this study to increase the reliability and validity of image interpretation. Several limitations warrant comment, however. First, due to the retrospective study design, data on several CVT risk factors (such as oral contraceptive use) were missing in a considerable proportion of patients. Second, patients with a benign dAVF and relatively benign symptoms (eg, tinnitus) who did not require treatment were usually discharged from follow-up. This limited follow-up time for some patients may have both biased our estimate of the incidence rate of CVT during follow-up and limited our functional-outcome assessment. Third, most patients with dAVFs underwent routine follow-up imaging, which increased the chance of incidentally finding asymptomatic CVT. This is supported by our finding that nearly half (44%) of the patients who developed CVT during follow-up had asymptomatic CVT.
CONCLUSIONS
CVT occurred in 31% of patients with dAVFs either initially or during follow-up. In 82% of cases, there was an anatomic relation between the dAVF and CVT. These data support the hypothesis of a bidirectional association between the 2 diseases.
Footnotes
L. Kuiper and M.S. van Kammen contributed equally to this work.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received March 28, 2022.
- Accepted after revision July 19, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}