
Abstract
SUMMARY: The incidental diagnosis of unruptured intracranial aneurysms has been increasing in the past several decades. A significant proportion represent small, low-risk, unruptured intracranial aneurysms for which there is equipoise on whether to offer treatment or conservative management. Given this uncertainty, patients may not always be comfortable with their physicians’ recommendations. Herein, we use game theory to study the interactions between physicians and patients to determine how conflict and cooperation affect the management of small, low-risk, unruptured intracranial aneurysms. We constructed a game theory model of the interaction between physicians and patients with respect to decision-making for a small, low-risk, unruptured intracranial aneurysm in an asymptomatic patient when there is perceived equipoise between whether to treat or manage conservatively. Assuming that both the physician and patient are rational and eliciting individual patient preferences is not practical, the physician should play the game based on an ex ante probability of meeting a patient with a certain type of preference. This recommendation means that the expectations of the physician regarding the patient’s preferences should guide the decision to offer treatment or conservative management as a first option for a small, asymptomatic, low-risk, unruptured intracranial aneurysm for which there is clinical equipoise.
ABBREVIATIONS:
- CM
- conservative management
- p
- probability
- T
- treatment
- UIA
- unruptured intracranial aneurysm
Roughly 2%–3% of the population has unruptured intracranial aneurysms (UIAs), amounting to approximately 6 million people in the United States.1 A recent study found a 5-fold increase in annual admissions with diagnoses of UIA during the past 2 decades, whereas the incidence of SAH has remained unchanged despite increases in the diagnosis and treatment of UIAs.2 This finding suggests that the substantial growth in the number of UIAs treated has not led to a decrease in the incidence of SAH, leading to the following question: Are most of these UIA treatments necessary and preventive?3
Studies have reported that up to 87.6% of UIAs are tiny, measuring <3–4 mm.4 On the basis of large longitudinal series, it is well-established5 that small sporadic UIAs have an overall low risk of rupture; however, in clinical practice, small aneurysms make up the majority of ruptured aneurysms.6 Increasingly, physicians may favor preventive treatment for even tiny UIAs to eliminate the risk of SAH.7 However, treatment of small UIAs is associated with a relatively high incidence of complications. Conservative management with imaging surveillance is performed to assess changes in the size and morphology that may predict a higher risk of rupture. However, the optimal frequency and duration of imaging are not defined.8 The optimal management of small, asymptomatic, low-risk UIAs is unclear,9 and uncertainty exists in the current guidelines10 and available literature, coupled with the lack of a clear understanding of the natural history of small UIAs.7 Therefore, the management of small UIAs represents a serious clinical conundrum.11
In our thought experiment, we explored the case of a small, asymptomatic, low-risk UIA for which there is equipoise as to whether to perform interventional/surgical treatment or recommend conservative management.
MATERIALS AND METHODS
We framed the patient-physician interaction in a game theory model. We developed a sequential Bayesian game model between the physician and patient to analyze the decision-making results for small UIAs when patient preferences are considered.
Model Design
In the game theory model, we have 2 players: the patient and the physician.
We defined the patients as 2 distinct types: 1) an aggressive patient who prefers to live without the risk of aneurysm rupture and, therefore, prefers the aneurysm treated by an interventional or surgical procedure, even if conservative management is recommended by the physician; and 2) a conservative patient who prefers conservative management and is satisfied with periodic imaging follow-up to assess aneurysm growth or change in morphology.
We define physicians as 2 distinct types: an aggressive and a conservative. These types of physicians differ in their willingness to treat certain small, low-risk aneurysms. On one end of the spectrum, there are more conservative physicians, who prefer to treat only aneurysms that are likely to rupture and who tend to refer many patients to imaging surveillance. On the other end of the spectrum, there are aggressive physicians, willing to treat small UIAs to minimize the possibility of rupture. The size of the UIA considered in equipoise is smaller for an aggressive physician than for a conservative physician.
We designed the game in such a way that the physician makes the first move. We assumed that the physician starts communication with the patient to inform the patient of the UIA diagnosis and discusses the management plan with either interventional/surgical treatment or periodic follow-up as a form of conservative management. Our model does not include a “no care” option for incidentally found UIAs. We assumed that if a physician decides to advocate for aneurysm treatment, this decision is associated with additional time and effort from the physician to explain all of the treatment options, risks, and benefits. Treatment also requires the physician to schedule the patient into a busy clinical workload and entails the physician’s anxiety about treating a smaller, low-risk lesion with more uncertainty of benefit and a higher risk of complication than larger, more clearly indicated aneurysms. This scenario is weighed against the physician’s expertise and experience in successfully treating UIAs to prevent aneurysm rupture with the related morbidity and mortality. The physician has the freedom to decide how to frame the discussion of the aneurysm.
In this model, the physician does not know the exact payoff function for a given individual patient. Instead, the physician has bias about these payoff functions for each patient type (aggressive, conservative). Besides, the physician knows his or her own choice regarding the willingness to treat small, asymptomatic UIAs.
In the model, there is a unique player in the game called “Nature.” Nature can randomly choose the patient and physician type for the game. Because we model the game from the physician’s perspective and the physician knows his or her own type, we modeled the game for each type of physician separately. Let us assume that with the probability p, the patient is an aggressive type, and with the probability 1−p, the patient is a conservative type. We make the common prior assumption that the probability distribution p is known to all players. In fact, the physician has a belief about the value of p, making this game one with imperfect information. Thus, while the physician is unsure about the type of patient presented for care, the patient has perfect information regarding his or her own risk type.
Next, we will explore the payoff matrices for both physician and patient types to investigate whether there is a pure strategy for the physician. By definition, pure strategy determines all players’ moves throughout the game.
Payoffs for Patient and Physician
The aggressive patient prefers to avoid living with the rupture risk of an UIA and will agree to treatment if offered by the physician. In the case of an aggressive physician, both the patient and the physician prefer treatment, and both get maximum payoff. The conservative physician would like to avoid offering conservative management for the aggressive patient, knowing that the patient would want treatment and be unhappy with an untreated UIA. This scenario could lead to an unsatisfied patient, while at the same time, the physician misses the opportunity to have occupational satisfaction in performing the treatment procedure.
The conservative patient will prefer to continue living with the UIA and undergo periodic imaging follow-up and will not agree to interventional treatment if offered by the physician. In case of a conservative physician, both the patient and physician prefer conservative management, and both get the maximum payoff. The aggressive physician would like to avoid wasting time and effort explaining the risks, benefits, and alternatives of treatment to the conservative patient because the patient would be unlikely to agree to treatment and the patient may lose trust in the physician whom they believe is offering unnecessary care. This scenario could lead to an unsatisfied patient, while at the same time the physician misses the opportunity to use his or her time more efficiently with some other patient.
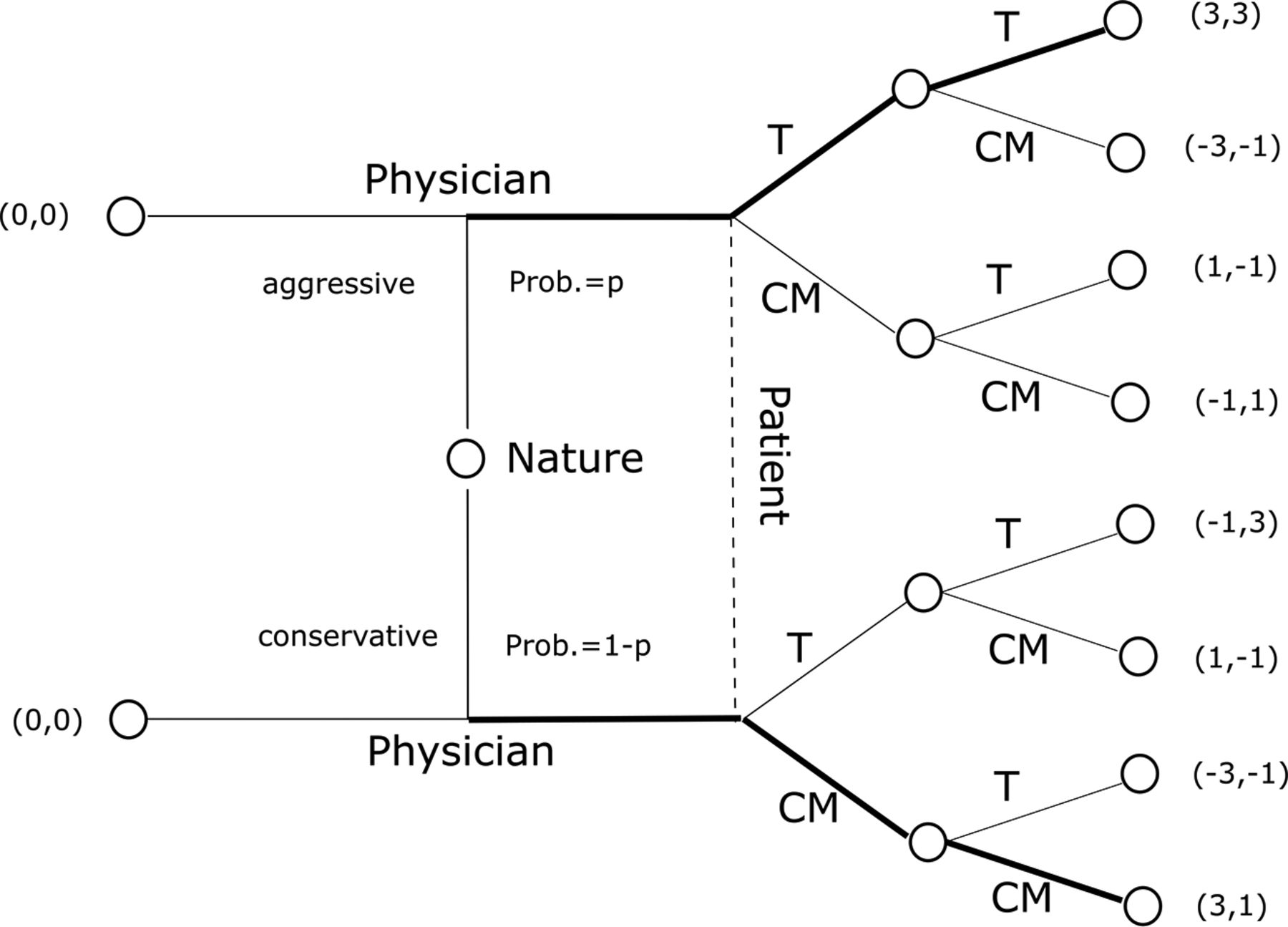
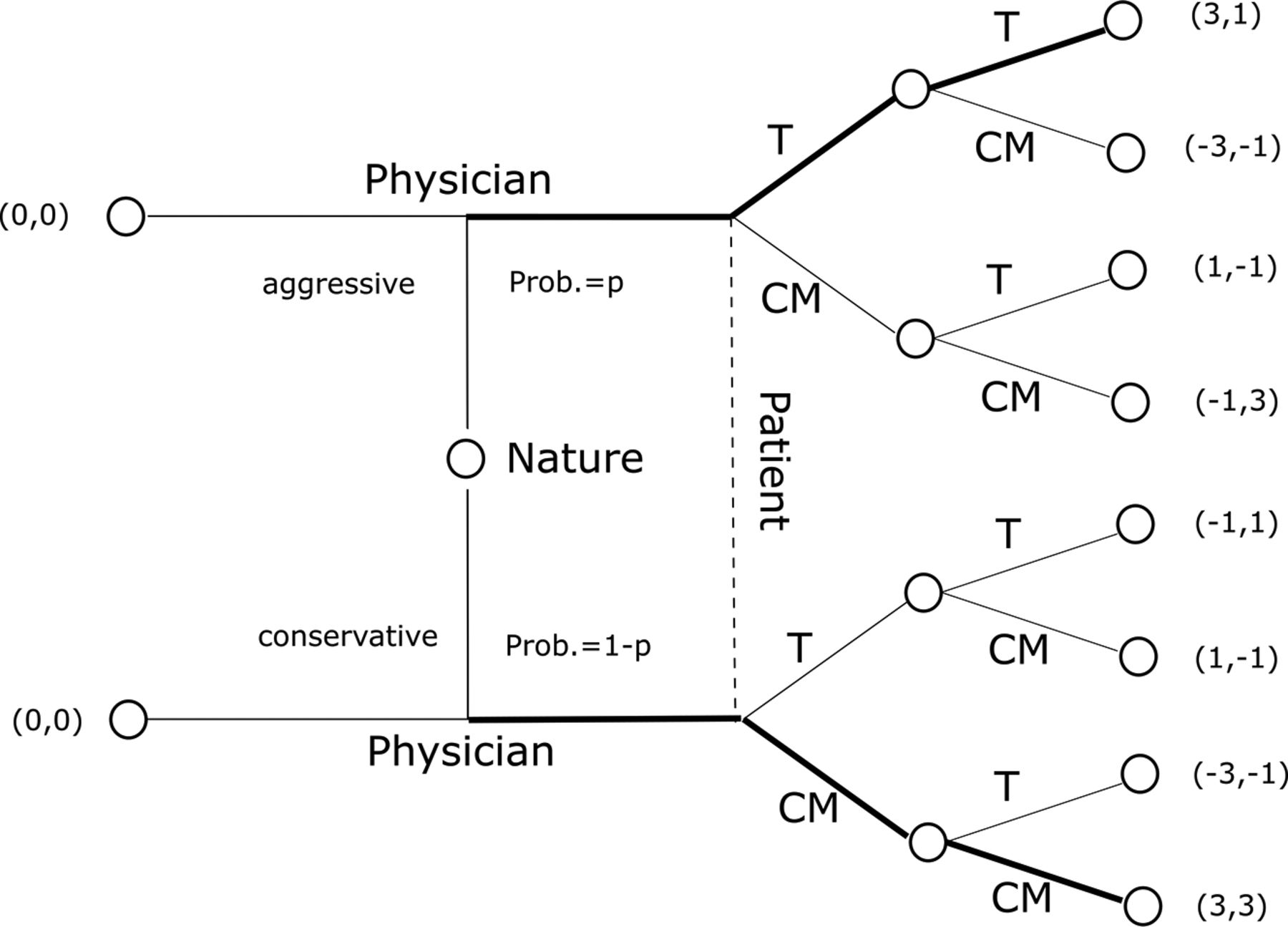
Therefore, for each player, there are 2 options: treatment (T) or conservative management (CM). For both types of physicians, for an aggressive patient, the dominant strategy is T, while for a conservative patient, the dominant strategy is CM. A physician will follow the patient’s decision to avoid conflict. Thus, we assume the following scoring system for the game: a patient will get 2 points for his or her preference and deduct 2 points for the nonpreferred option. The patient will add 1 point if there is no conflict with the physician and deduct 1 point if there is a conflict with the physician. The physician will add 1 point for no conflict with the patient and deduct 1 point if there is a conflict with the patient. In addition, an aggressive physician will add 2 points if treatment is selected by both the patient and the physician. A conservative physician will add 2 points if conservative management is selected by both parties. Hence, the Bayesian Normal Form representation of the game is shown in Fig 1 (aggressive physician) and Fig 2 (conservative physician).

Bayesian Normal Form representation (aggressive physician). Prob. indicates probability.

Bayesian Normal Form representation (conservative physician). Prob. indicates probability.
On the basis of the Bayesian Normal Form representation, we developed the payoff matrices for both types of physicians, as shown in Table 1 (aggressive physician) and Table 2 (conservative physician).
Combined payoff matrix for both types of patients (aggressive physician)
Combined payoff matrix for both types of patients (conservative physician)
Results
Given the above, the aggressive physician faces the following dilemma: If the aggressive physician chooses T, the payoff will be p × (3) + (1−p) × (−1) = 4p−1. If the aggressive physician chooses CM, the payoff will be p × (−1) + (1−p) × (1) = 1−2p. Thus, if 4p−1 > 1−2p, then p > 1/3, the aggressive physician will choose T. If p < 1/3, the aggressive physician will choose CM. The aggressive physician will flip a coin to decide the choice if p = 1/3.
Similarly, the conservative physician faces the following dilemma: If the conservative physician chooses T, the payoff will be p × (1) + (1−p) × (−1) = 2p−1. If the conservative physician chooses CM, the payoff will be p ×(−1) + (1−p) × (3) = 3−4p. Thus, if 2p−1 > 3−4p, then p > 2/3, the conservative physician will choose T. If p < 2/3, the conservative physician will choose CM. The conservative physician will flip a coin to decide the choice if p = 2/3.
Thus, whether the patient is offered first treatment or conservative management depends on both the physician type and the physician’s belief of the probability that the patient is an aggressive type.
In our Bayesian game, we have a pure strategy for each type of patient, but the physician does not have a pure strategy because the physician does not know the type of patient presenting for care. Therefore, the physician must play a mixed strategy, using his or her belief about the patient type based on the probability of facing each type of patient.
The optimal mixed strategy in this game is a perfect Bayesian Nash equilibrium, in which each player maximizes the payoffs given his or her belief about the state of Nature and the strategies played by other players. Assuming that both the physician and patient are rational and eliciting individual patient preferences is not practical, it makes sense for the physician to play the game according to the perfect Bayesian Nash equilibrium. The physician will choose the strategy on the basis of the probability of meeting an aggressive patient. The practical implication of this result is that a physician is interested in knowing ex ante the proportion of aggressive and conservative patients in the population that he or she is serving. The difference between an aggressive and conservative physician would be in the threshold value of the p that they would use to determine whether to offer treatment or conservative management as a first option.
DISCUSSION
For incidentally detected UIAs, physicians need to consider multiple factors when considering treatment, such as patient preferences, including the anxiety of the patient or the patient’s family, the right not to know or patient autonomy, the age of the patient, the complexity of the aneurysm, the risk of aneurysm rupture, and so forth.12 The diagnosis of a UIA can be a source of stress to the patient. Therefore, the optimal care for patients with a UIA should take patient preferences into account. In clinical practice, it may be time-consuming for a physician to allocate time to elicit individual patient preferences. Our model suggests that a more efficient approach would be to ascertain the patient preferences in the target population the physician is serving to know how many are aggressive-versus-conservative types. Knowing this and knowing his or her own personal preference toward being more aggressive or more conservative with treatment, the physician can choose the more appropriate strategy on which treatment option to offer first every time the physician encounters the situation of equipoise with a small, asymptomatic UIA.
UIAs can be associated with a not-negligible risk of treatment-related complications with associated morbidity and mortality, as well as the risk of recurrence and rupture despite treatment.13 Furthermore, it has been reported that for low-risk aneurysms, the benefits of treatment are marginal or even negative, being about 1 life-year for a 20-year-old patient, falling to 0 life-years for a 60-years-old patient, and becoming marginally negative for older patients.14
Risk-stratification models provide information for physicians on how to use optimal clinical strategies under conditions of uncertainty in the context of a true patient diagnosis.15 Unfortunately, they do not take into account patient preference. Recently, researchers have been calling for greater patient involvement in decision-making, after receiving precise and detailed information regarding his or her individual aneurysm risk, as well as the potential risks of treatment.16 Our model demonstrates how patients and physicians could interreact to achieve optimal outcomes when approaching small UIAs when clinical equipoise is present.
One limitation of our model is that there may be many more patient types than just aggressive and conservative. For example, a third type of patient might exist who is undecided about whether to be treated or followed up and for whom detailed information about the benefits and risks of both management options would be most valuable. Nevertheless, this patient type does not fundamentally change the model because the main insight from the model is that the physician should start discussions with the patient with the strategy preferred by the most prevalent patient type. If the most prevalent patient type is equally interested in both treatment options, the optimal physician strategy would be to give an overview of the differences between treatment options, instead of starting with one of the options. There may also be multiple physician types with different incentives regarding treatment of small UIAs. Additionally, the payoff matrices may have different values than we used in our thought experiment. Our aim was to investigate the importance of taking patient preferences into account in the decision-making about the treatment of small UIAs, and we found that patient preference can impact ultimate treatment decisions if one is attempting to achieve optimal outcomes.
Finally, this model assumes equipoise in the physician’s drive to treat versus monitor an aneurysm. If the conversation between the patient and the physician regarding the relative risks of treatment versus observation is presented as “a time bomb ticking in your head” versus “most likely this aneurysm will never bleed,” the patient will likely be led to very different treatment choices. Thus, patient preference is linked to physician preference in terms of the level at which treatment is offered or physician comfort with risk-taking. In this model, we assume that the physician does not have a preference as to whether to treat or not to treat the aneurysm. Therefore, the physician might consider eliciting patient preferences regarding treatment or observation of UIAs.
Identifying patient preferences would allow the physician to categorize patients into different types and offer them different options in terms of managing their UIA. On the other hand, in practice it may be difficult to elicit an individual patient’s preference, and unconscious biases may influence a physician’s perceptions. Therefore, it is possible that in clinical practice, an optimal strategy for the physician would be to play the sequential Bayesian game on the basis of the probability of meeting each patient type in their clinical practice, instead of spending time and effort eliciting individual patient preferences. This possibility should not be interpreted as an implicit bias in a clinical scenario because from the clinical perspective, the benefits of treatment are about equal to the risks of treatment. The sequential Bayesian game provides an efficient mechanism to take patient preferences into account quickly in the clinical setting.
In clinical practice, every patient should be offered the opportunity to choose aggressive or conservative management. Our analysis focuses on the first option a physician should prioritize or bring up in discussions with the patient. All other options should also be explained to ensure informed patient decision-making. Nevertheless, if a physician chooses the strategy on the basis of the probability of meeting an aggressive patient, the probability of the patient’s acceptance of the first proposed strategy is the highest, saving valuable time for the physician and patient. Besides, with this strategy, there is a higher chance that the patient’s preferred small, low-risk UIA management strategy is selected, which increases patient satisfaction.
CONCLUSIONS
Patient preferences need to be taken into account in decision-making to treat or observe low-risk aneurysms when on the basis of other factors like age and medical comorbidities, there is clinical equipoise. On the other hand, eliciting individual patient preferences in clinical care may not be practical. To achieve an optimal outcome, physicians should gauge preferences in their patient population and incorporate this knowledge into their management of small low-risk UIAs. Knowing the proportion of aggressive patients in their patient population may help physicians determine whether to offer treatment or conservative management first when equipoise exists.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received May 28, 2021.
- Accepted after revision November 1, 2021.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.