
Abstract
SUMMARY: Pediatric patients with myelopathy expressing intradural spinal vascular ectasia without arteriovenous shunting were studied at four tertiary referral neuropediatric centers. Patients were identified by retrospective review of institutional records and excluded if spinal vascular pathology could be classified into a previously described category of spinal vascular malformation. Four patients meeting the study criteria were enrolled in the study. Clinical, magnetic resonance imaging, catheter-directed angiography, laboratory, histological and genetic data were analyzed to characterize the disease process and elucidate underlying pathomechanisms. Our study revealed a highly lethal, progressive multi-segmental myelopathy associated with a unique form of non-inflammatory spinal angiopathy featuring diffuse enlargement and tortuosity of spinal cord arteries, spinal cord hyperemia, and spinal cord edema (Arterioectatic Spinal Angiopathy of Childhood). The condition was shown to mimic venous congestive myelopathy associated with pediatric spinal cord arteriovenous shunts on MRI but to have distinct pathognomonic findings on catheter-directed angiography. Clinicopathological, genetic, and neuroimaging features, which are described in detail, closely overlap with those of mitochondrial disease.
ABBREVIATIONS:
- AESA
- arterioectatic spinal angiopathy
- AV
- arteriovenous
- CPA
- cerebral proliferative angiopathy
- RMA
- radiculomedullary artery
- WES
- whole exome sequencing
Spinal cord arteriovenous (AV) shunts, including AV malformations (AVM) and AV fistulae (AVF) are a rare but treatable cause of myelopathy.1⇓⇓-4 Marked ectasia of the spinal cord vasculature on MR imaging is traditionally considered pathognomonic. In children with spinal cord AV shunts, subarachnoid hemorrhage is the clinical presentation in two-thirds, while venous congestive myelopathy is the presentation in one-third.1,2 Notably, venous congestive myelopathy due to a spinal cord AV shunt is more common in children younger than 2 years of age and features cord edema that spares the cord periphery.3 A definitive diagnosis relies on demonstration of an AV shunt by catheter-directed DSA. Children with venous congestive myelopathy due to a spinal cord AV shunt most often present with progressive episodic neurologic decline, culminating in complete loss of spinal cord function within months to years.1⇓⇓-4 If the diagnosis is established early, treatment of the underlying AV shunt by embolization or microsurgical ligation leads to neurologic stabilization with varying degrees of functional recovery.1,5
Recognized forms of spinal cord vascular malformations include AV shunt lesions and nonshunting lesions. While multiple classification systems have been proposed, none account for spinal cord vascular ectasia in the absence of an AV shunt.6 The authors of this report have encountered pediatric patients with myelopathy presenting with striking enlargement of the spinal cord vasculature and vasogenic edema of the central spinal cord in the absence of AV shunting. In this report, we describe this previously uncharacterized spinal angiopathy and review the literature to identify cases that have phenotypic overlap. Experiences with different treatment strategies are presented, and alternate theories of pathogenesis are considered.
MATERIALS AND METHODS
This study received institutional review board (Cincinnati Children’s Hospital Medical Center) approval for exempt research and a waiver of informed consent. Neuropediatric specialists at 4 tertiary referral centers retrospectively reviewed their records to identify children with myelopathy who underwent catheter-directed DSA to evaluate abnormally enlarged spinal cord vessels found on MR imaging. Patients were excluded if DSA showed an AV shunt or vascular abnormality that could be classified into a known category of spinal vascular malformation. Clinical, laboratory, MR imaging, DSA, histopathologic, and genetic data were retrospectively analyzed at each study site. Descriptive analysis of anonymized data submitted by each site was performed.
Presenting clinical features, clinical course, and laboratory findings were assessed by electronic medical record review at the site where the patient’s care was provided. Spinal MR imaging studies and catheter-directed spinal DSA studies of each patient were also reviewed by study investigators at the site where patient care was provided. When available, brain MR imaging, cerebral MR spectroscopy, and catheter-directed cerebral DSA studies were similarly reviewed.
Results of standardized genetic testing performed on blood samples were reviewed at the site where the corresponding patient’s care was provided. In 1 case, whole exome sequencing (WES) and deletion analysis of nuclear and mitochondrial DNA from blood and nuclear DNA from radiculomedullary artery (RMA) tissue, performed at ×150 and ×159 resolution, respectively, were reviewed. In this case, targeted nuclear sequence analysis was also performed, covering multiple gene superfamilies (RHO, RHEB, and RAS) and individual genes implicated in the pathogenesis of AVMs (MEK, PTEN, NOTCH1, and so forth).7 In another case, WES of nuclear DNA from blood was performed. Genetic panels for hereditary hemorrhagic telangioectasia and capillary malformation AVM syndrome were used to examine nuclear DNA from blood samples of 3 patients.
The authors performed a literature review to identify spinal vascular pathology that phenotypically overlaps with the angiopathy described in this report. We searched the PubMed database for English language reports published between January 1953 and January 2022 using the search terms “ectasia,” “dolichoectasia,” “arteriopathy,” and “arteriovenous” crossed with the term “spinal.”
RESULTS
Each of 4 participating sites identified 1 patient that met the study criteria, contributing a total of 4 patients (2 females) in a record review period that spanned 14–35 years; median, 18 (SD, 8) years. Every patient in this series presented before the advent of the Severe Acute Respiratory Syndrome coronavirus disease 2019 (SARS-CoV-2) pandemic. Presenting clinical features of each patient are detailed in the Online Supplemental Data. The first symptoms of myelopathy presented at a median age of 17.5 (SD, 8.5) months (range, 11–24 months). All patients initially presented with delayed onset or regression of ambulatory motor skills and hypotonia. Physical findings included cutaneous vascular birth marks in 2, eczema in 1, and bilateral cataracts in 1. Three of 3 patients with a perinatal history had complications including preeclampsia, prematurity, postmaturity, or breech presentation. One was noted to have a neonatal history of subdural hygromas. In 1 case, there was a maternal family history of recurrent spontaneous abortion.
Laboratory study results for each patient are detailed in the Online Supplemental Data. Two patients underwent electromyography and nerve-conduction studies, with normal results. CSF analysis showed normal protein and glucose levels and cell counts in all patients. CSF from 2 patients was submitted for comprehensive studies including lactate, amino acids, pyruvate, neurotransmitters, myelin basic protein, aquaporin 4, immunoglobulin G, oligoclonal bands, neopterin, and biopterin. CSF lactate was abnormally elevated in one, and CSF pyruvate was abnormally elevated in another. Hematology lab studies revealed microcytic anemia in 1 patient. Two had abnormally elevated serum transaminase levels late in their clinical course.
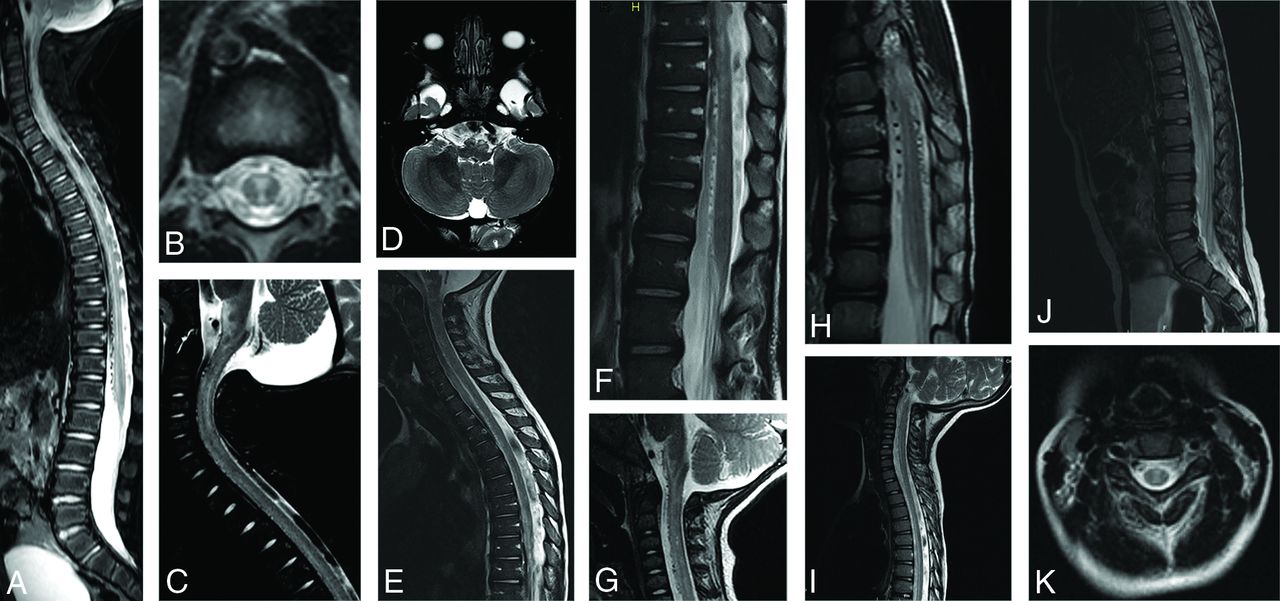
Spinal MR imaging results for each patient are detailed in the Online Supplement Data and are highlighted in Fig 1. On T2-weighted images, abnormally ectatic and tortuous pial blood vessels surrounded the spinal cord and conus medullaris. There was abnormal T2 signal hyperintensity in the central spinal cord (anterior > posterior) and cord tumefaction in all patients. T2 signal hyperintensity longitudinally involved the entire cord and extended into the ventral medulla. Variable cord parenchymal enhancement was present in 2 patients.

Spine MR imaging findings. A, Midline T2-weighted sagittal MR image of the spine in patient 1 shows abnormal T2-weighted hyperintense signal in the thoracic spinal cord and conus medullaris. Spinal cord volume expansion is also present. There is conspicuous abnormal perimedullary vascular ectasia anterior to the conus medullaris and thoracic spinal cord. B, Axial T2-weighted image of the midthoracic spine shows the distribution of abnormal T2-weighted signal hyperintensity within the central and anterior spinal cord. C, Midline T2-weighted sagittal MR image of the cervical spine reveals abnormal T2-weighted hyperintense signal in the central cervical spinal cord and ventral medulla. There is diffuse spinal cord swelling affecting the region of the cervical enlargement. D, Axial T2-weighted image of the brain at the level of the medulla shows T2-signal hyperintensity in the pyramids, more conspicuous on the left. E, Midline T2-weighted sagittal MR image of the cervical and thoracic spine in patient 4 shows abnormal T2-weighted hyperintense signal in the ventral cervical and thoracic spinal cord and medulla. There is spinal cord volume expansion, prominent in the region of the cervical enlargement, and abnormal perimedullary vascular ectasia anterior to the thoracic spinal cord. F, Midline T2-weighted sagittal MR image of the lower thoracic and lumbar spine reveals abnormal T2-weighted hyperintense signal in the anterior spinal cord. There is diffuse spinal cord swelling, severely affecting the region of the lumbar enlargement. Note marked ectasia of the perimedullary vessels anterior to the spinal cord. G, Midline T2-weighted sagittal MR image of the cervical spine in patient 3 shows abnormal T2-weighted hyperintense signal in the central and anterior cervical spinal cord as well as in the ventral medulla. Mild expansion of cervical spinal cord volume is also present. Conspicuous abnormal perimedullary vascular ectasia anterior to the cervical spinal cord is demonstrated. H, Midline T2-weighted sagittal MR image of the lower thoracic spine reveals abnormal T2-weighted hyperintense signal in the central and anterior thoracic spinal cord and conus medullaris, with mild associated volume expansion. Note marked perimedullary vascular ectasia surrounding the spinal cord. I, Midline T2-weighted sagittal MR image of the cervical and thoracic spine in patient 2 shows abnormal T2-weighted hyperintense signal in the cervical and thoracic spinal cord. The region of the cervical enlargement is severely affected and shows mild volume expansion. J, Midline T2-weighted sagittal image of the lower thoracic and lumbar spine shows abnormal T2-weighted signal hyperintensity within the anterior spinal cord. There is conspicuous perimedullary vascular ectasia anterior to the conus medullaris. K, Axial T2-weighted MR image of the cervical spine reveals abnormal T2-weighted hyperintense signal in the central cervical spinal cord.
Brain MR imaging studies were performed in all patients. The results are detailed in the Online Supplemental Data and are highlighted in Fig 2. In 2 patients, there was mild diffuse encephalomalacia and ex vacuo enlargement of the cerebral ventricles and cortical sulci without signal abnormality. In another, there was signal abnormality in the anterior pons, pontine raphe, and middle cerebellar peduncles. Cerebral MR spectroscopy was performed in 3 patients. An abnormal lactate peak in the cerebral periventricular white matter was demonstrated in 1. Diffuse ectasia of the intracranial arteries shown on T2-weighted images of the brain was reported in 1 patient and unreported in 3 patients.

Brain imaging findings. A, Reference T2-weighted sagittal, axial, and coronal MR images of the brain from patient 1 and MR spectroscopy. There is mild diffuse cerebral parenchymal volume loss with commensurate ex vacuo ventriculomegaly. Note placement of a sampling voxel for MR spectroscopy in the subcortical white matter of the mesial left parietal lobe. MR spectroscopy shows an abnormal inverted doublet peak between 1.3 and 1.4 parts per million, corresponding to lactate (red circle). B, T2-weighted axial image of the brain shows ectasia of the basilar artery and bilateral intradural internal carotid arteries. C, T2-weighted axial image of the brain shows ectasia of the MCAs and posterior cerebral arteries bilaterally. D, Symmetric T2-weighted signal hyperintensity in patient 4 is demonstrated in the anterior edge of the pons, pontine raphe, and middle cerebellar peduncles. E, Axial T2-weighted images at level of foramen of Monro in patients 1 and 4 show mild cerebral parenchymal volume loss with ex vacuo dilation of the cerebral ventricles and cortical sulci.
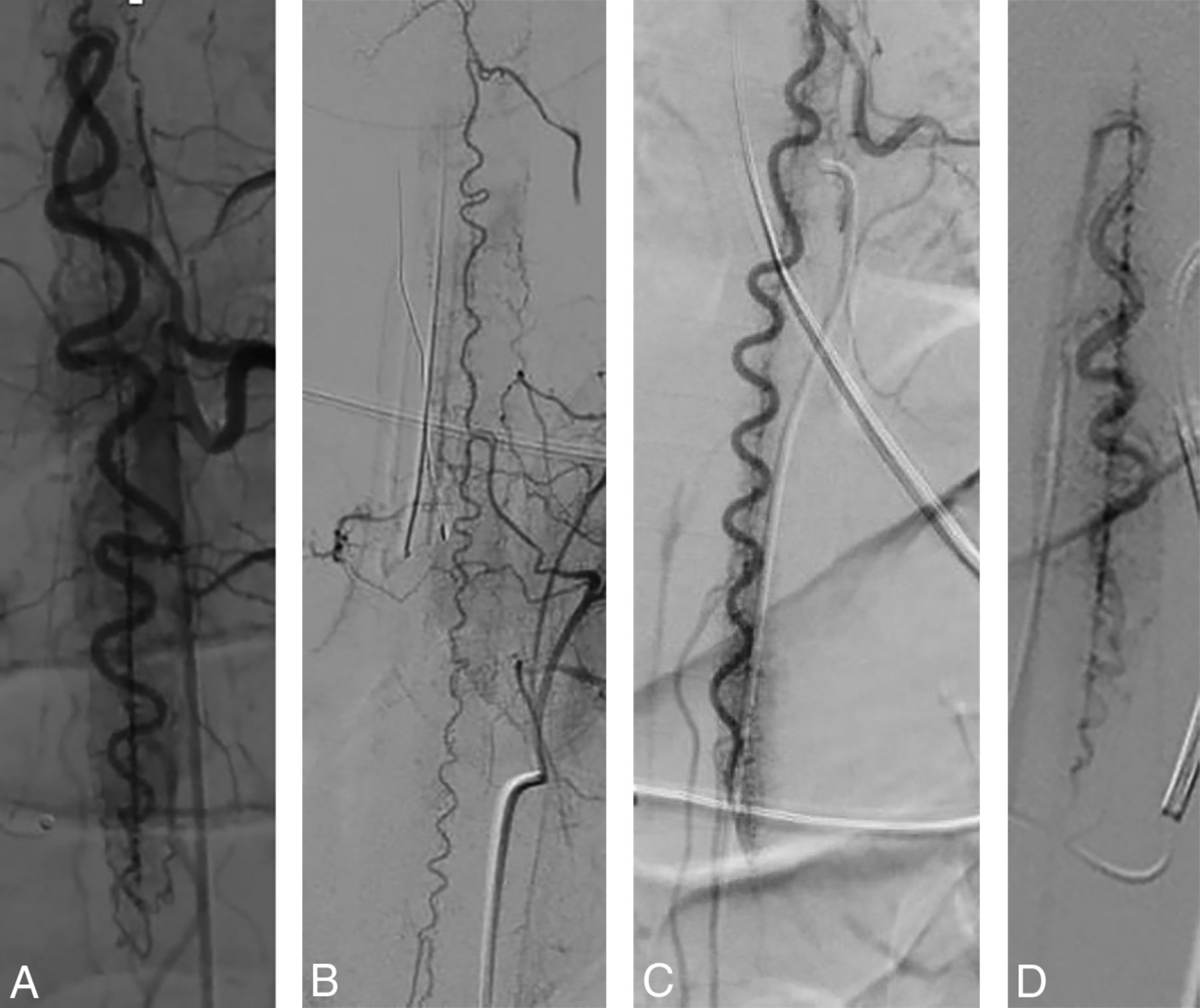
The results of catheter-directed spinal DSA are detailed in the Online Supplemental Data and highlighted in Fig 3. In all patients, catheter-directed DSA showed marked ectasia and tortuosity of the anterior spinal artery. In 3 of 4 patients, DSA of the dominant lower thoracic RMA showed the descending ramus of the anterior spinal artery to be much larger than the ascending ramus. Multiple RMAs were markedly ectatic in each patient, though the dominant lower thoracic RMA was most ectatic. In every patient, the central sulcal penetrators were markedly enlarged, producing a conspicuous pattern resembling the steps of a spiral staircase cycling between “on end” and “elongated” orientations in frontal-projection angiograms (Fig 3). By comparison, the posterolateral spinal arteries and radiculopial arteries were only modestly enlarged. Extrinsic spinal cord veins were modestly enlarged. Intrinsic spinal cord veins were not demonstrably enlarged. All patients demonstrated spinal cord hyperemia with brisk parenchymal venous drainage. In all patients, the prompt and diffuse angiographic appearance of the medullary and perimedullary veins followed the angiographic appearance of a hyperemic spinal cord parenchymal blush. There was no angiographic documentation of direct arterial-to-venous shunting (ie, AVF or AVM) in any patient.

Catheter-directed angiography findings. A, Frontal projection of a left T11 posterior intercostal artery angiogram in the early arterial phase from patient 1 shows marked ectasia of the dominant lower thoracic RMA and descending ramus of the anterior spinal artery (ASA). The ascending ramus of the ASA is mildly enlarged. The left posterolateral spinal artery is mildly enlarged. There is a uniform, unusually intense parenchymal capillary blush and early appearance of parenchymal draining veins. Note striking ectasia of the central sulcal penetrators. B, Frontal projection of a left supreme intercostal artery angiogram in the early arterial phase from patient 4 shows moderate diffuse ectasia of the ASA and central sulcal penetrators. Two RMAs are shown to be moderately ectatic. Note patchy intensification of the parenchymal capillary blush. C, Frontal projection of left posterior intercostal artery angiogram in the early arterial phase from patient 3 shows marked ectasia of the dominant lower thoracic RMA and descending ramus of the ASA. There is striking ectasia of the central sulcal penetrators. There is a uniform, unusually intense parenchymal capillary blush most prominent in the region of the conus medullaris and early appearance of parenchymal draining veins. D, Frontal projection of the right posterior intercostal artery angiogram in the early arterial phase from patient 2 shows ectasia of the dominant lower thoracic RMA and descending ramus of the ASA. Note striking ectasia of central sulcal penetrators.
Catheter-directed cerebral angiography was performed in 1 patient. Results detailed and shown in the Online Supplemental Data describe moderate diffuse intracranial arterial ectasia.
The clinical course for each patient is detailed in the Online Supplemental Data. All patients developed a spastic gait disorder with bilateral lower-extremity paraparesis. Three of 4 progressed to quadriparesis within 7–34 months. One patient also had loss of head control and respiratory depression within 15 months. This patient died of aspiration pneumonia. Another died with lactic acidosis and progressive encephalopathy (Online Supplemental Data). Two patients remained ambulatory at last follow-up 1–4 years after onset. Two patients had marked transient exacerbations of neurologic deficits after febrile illness or general anesthesia. One patient was treated with vitamin E and carnitine to augment mitochondrial function but had no improvement. One patient treated with steroids failed to improve. This patient was also treated with microsurgical ligation of the dominant RMA in an attempt to reduce spinal cord hyperemia and edema. After a few days of neurologic worsening corresponding to the effects of anesthesia, the patient returned to neurologic baseline but died of complications from aspiration pneumonia 5 weeks later. Histopathologic examination of the resected RMA showed normal vessel wall architecture without evidence of inflammation (Fig 4).

RMA histopathology. Patient 1. A, Hematoxylin and eosin–stained axial cross-section perpendicular to the long axis of the vessel at medium power (original magnification ×50) shows a normal trilaminar arterial wall architecture with no evidence of inflammation. B, Trichrome-stained axial cross-section perpendicular to long axis of the vessel at medium power (original magnification ×50) delineates normal elastic tissue architecture and integrity of the artery.
Testing with negative results for hereditary hemorrhagic telangioectasia (3-gene panel: endoglin, SMAD4, and activin receptor-like kinase) was performed on blood samples from 3 patients. Genetic testing for capillary malformation AVM syndrome (2-gene panel including ephrin B4 and RASA1) with negative results was performed on blood samples from 2 patients. WES of nuclear DNA from blood revealed a pathologic mutation in 1 allele of the TFRC gene in 1 patient. WES and targeted sequence analysis did not reveal confirmatory evidence of pathologic mutations in blood or RMA tissue in another patient. Mitochondrial DNA testing in the same patient did not reveal evidence of a pathologic mutation.
Our literature search yielded 1154 publications. Three reports warranted full-text review after abstract evaluation.8⇓-10One report described a “spinal arterial malformation” without a venous component in a child with hereditary hemorrhagic telangioectasia based on findings at surgery.8 Two additional references describing “spinal arterial anomalies” were found in the bibliography of this report.11,12 Neither MR imaging nor catheter-directed angiography was performed in any of the cases from these reports. Consequently, our literature review was unable to confirm any cases of nonshunting spinal cord arterial ectasia.
DISCUSSION
This report describes 4 cases of early-onset childhood myelopathy, each expressing a similar pattern of clinical and neuroimaging features and each associated with an unusual form of arterioectatic spinal angiopathy (AESA). All children initially presented with hypotonia and impaired ambulatory motor skills during the first 2 years of life. Most showed rapid progression to quadriparesis, and half died from disease-related complications within 6 years of onset. The clinical and neuroimaging features of AESA have striking overlap with those expressed in venous congestive myelopathy due to spinal cord AVM/AVF. Clinical recognition of the former and differentiation from the latter are critical to prevent misguided and potentially harmful vascular interventions. Our literature review confirms that AESA is a currently unrecognized form of spinal cord vascular pathology. Perhaps the most important factor contributing to the lack of prior recognition is the similarity that AESA bears to childhood spinal cord AVM/AVF. All of the cases presented in this series were initially misdiagnosed as AVM/AVF. It is likely that other cases were also misdiagnosed and perhaps even treated as AVM/AVF.
Every child in the current series showed ectasia and tortuosity of the spinal cord vasculature on MR imaging. Each case also demonstrated T2 signal hyperintensity in the central and anterior spinal cord, as well as cord tumefaction. This combination of MR imaging findings is common in children with intradural spinal AVF and adults with spinal dural AVF, though spinal dural AVF has not been convincingly reported in children.13 Notably, gold standard catheter-directed DSA excluded AVF in all our patients. The overlapping neuroimaging features of AESA and spinal cord AVF of childhood may indicate that some aspects of pathogenesis are shared. The pattern of spinal cord signal abnormality and tumefaction demonstrated in our patients suggests vasogenic edema and cord swelling, as seen in children with an intradural spinal AVF. In both conditions, the spinal cord experiences an imbalance between arterial inflow and venous outflow, resulting in vascular congestion. In the former, spinal cord arterial inflow is augmented, and in the latter, spinal cord venous drainage is diminished. The entire spinal cord and ventral medulla are shown to be affected in our patients. Clinically severe (lethal) cases also showed variable cord enhancement, indicating cord–blood barrier disruption.
In contrast to children with intradural spinal AVF, patients with AESA demonstrate cord hyperemia causing early, dense parenchymal staining on DSA. AESA is further characterized by brisk, diffuse angiographic filling of spinal cord veins draining hyperemic spinal cord capillary beds. This pattern of circulation is a characteristic finding on which the diagnosis of AESA may be based. The angiographic features of spinal cord parenchymal venous drainage in AESA contrasts with those seen in cases of an AV shunt with medullary venous hypertension (ie, spinal dural AVF) in which there is an absent or delayed angiographic appearance of the veins serving the affected spinal cord segments.14 Marked arterial ectasia, out of proportion to venous ectasia, is another diagnostic hallmark of AESA. In our series, catheter-directed DSA shows ectasia and tortuosity of the anterior spinal artery and corresponding central sulcal perforators. Most cases show relatively mild enlargement of posterolateral spinal arteries, suggesting that ectasia is proportional to the size of the vascular territory within the cord. This finding loosely correlates the magnitude of angiopathic changes with blood-flow demand.
AESA as defined by the clinical and neuroimaging features reported here has not been previously described in the peer-reviewed, indexed medical literature. Two cases satisfying the diagnostic criteria for AESA set forth here were described in a book chapter on spinal cord AVM.15 These patients underwent catheter-directed DSA for further evaluation of myelopathy, one at 2 years of age and the other at 5 years of age. In both cases, spinal DSA revealed ectasia of the anterior spinal artery and central sulcal perforators with corresponding cord hyperemia.
The etiology of AESA and its precise relationship to myelopathy are presently unknown. Analysis of blood, CSF, and RMA tissue from our patients showed no evidence of inflammation. Furthermore, glucocorticoid steroid therapy showed no beneficial effect in 1 patient. Early in our experience, the observation of spinal cord hyperemia and edema led us to hypothesize that neurologic impairment might be the consequence of abnormally increased arterial perfusion of the spinal cord, unbalanced by venous drainage. We thus speculated that controlled reduction of spinal cord hyperemia by surgical ligation of the dominant RMA might reduce cord edema and improve neurologic function. Unfortunately, this intervention was not beneficial, suggesting that cord hyperperfusion is not a primary driver of myelopathy.
Multiple findings suggest that AESA is a manifestation of metabolic myelopathy due to mitochondrial disease. Among these findings are elevated CSF lactate and a cerebral MR spectroscopy lactate peak in 1 case, systemic lactic acidosis and encephalopathy in a second case, and elevated CSF pyruvate in a third. Transaminasemia, premature cataracts, and microcytic anemia in our cohort further support a mitochondrial disease origin.16,17 Notably, none of our patients demonstrated evidence of myopathy (cardiac or skeletal muscle). Numerous metabolic disorders including mitochondrial diseases presenting with myelopathy in early childhood manifest MR imaging features that resemble those reported here.18,19 In our cohort, longitudinally extensive spinal cord lesions spanning >3 vertebral bodies were observed. This feature is characteristic of myelopathy in children with primary mitochondrial disease.19 Moreover, in our series, MR imaging revealed T2 signal hyperintensity and tumefaction involving the central and anterior cord. This MR imaging pattern of myelopathy has also been reported in a subset of children with primary mitochondrial disease.19 Additionally, cervical cord involvement with extension into the medulla is a common feature of childhood mitochondrial myelopathy seen in our cases.19
Pathogenic mutations that cause mitochondrial disease can occur in the nuclear genome or the mitochondrial genome.20 Notably, 1 patient in this series was heterozygous for a dominant pathologic mutation of a transferrin receptor gene (TFRC). Transferrin receptors are believed to play a vital role in the regulation of normal mitochondrial function and fragmentation.21 Additionally, mouse models show mitochondrial dysfunction in heterozygous transferrin receptor mutants.22 Incidentally, abnormalities of transferrin receptor function may also explain associated anemia and childhood-onset cataracts.23⇓⇓-26 Although 1 other patient in this series underwent extensive testing of nuclear and mitochondrial DNA without identification of a pathologic mutation, previous studies have shown that such testing yields a positive result in only 10%–20% of children with clinical mitochondrial disease.27⇓-29
Arteriopathy as a primary or secondary manifestation of mitochondrial disease is now widely recognized.30 Microvascular and macrovascular forms are well-described.30 In patients with mitochondrial disorders, secondary arteriopathies are manifestations of the vascular effects of metabolic dysfunction in distinct organ systems such as the liver or pancreas. One model of secondary arteriopathy in AESA could be based on an abnormally increased metabolic demand in the diseased spinal cord imposing an increased blood-flow requirement that promotes adaptive or maladaptive expansive remodeling of spinal cord arteries. If the AESA phenotype requires the combined effects of 2 mutations, one controlling mitochondrial function and the other controlling arterial adaptation to blood flow demand, it would account for the extreme rarity of AESA. Notably, primary mitochondrial arteriopathy is often characterized by arterial ectasia and aneurysm formation.30 Diagnostic markers of primary mitochondrial arteriopathy include abnormal expression of succinate-dehydrogenase or cyclooxygenase in vascular tissue or abnormal cristae formation in mitochondria from vascular smooth-muscle cells and pericytes.30 The former relies on immunohistochemical staining of fresh-frozen tissue, and the latter relies on electron microscopy of glutaraldehyde-fixed tissue.
Immunohistochemical and electron microscopy studies of affected vascular tissue may improve our understanding of AESA pathogenesis in the future. Abnormal ectasia of the aorta and cerebral arteries has been reported as a primary feature of clinical mitochondrial disorders.30 Mitochondrial arteriopathies involving retinal vessels, cochlear vessels, cervicocerebral vessels, brachial vessels, iliac vessels, skeletal muscle vessels, and cutaneous vessels have been reported.31Asymptomatic generalized cerebral arterial ectasia was present in 1 patient from the current series, suggesting that AESA may be part of an angiopathy spectrum that variably affects the entire CNS. Notably, 2 of our patients showed cerebral parenchymal volume loss, and a third experienced progressive encephalopathy, suggesting a diffuse CNS process.
Our review of the literature has not revealed prior cases of mitochondrial disease expressing AESA as a trait.30⇓⇓⇓⇓-35 It is possible that the cases described in this report represent the extreme end of a spectrum in which milder forms are more prevalent but difficult to detect. Mild forms of AESA may not be detected on MR imaging, just as perimedullary vascular flow voids may be inapparent in patients with spinal dural AVFs.36,37 CNS mitochondrial disorders are known to express a wide range of phenotypic heterogeneity.38 Subclinical mitochondrial vasculopathies revealed by specialized, nonclinical tests have been found in numerous studies.24 It is also possible that mild forms of AESA are overshadowed or preempted by other complications of mitochondrial disease such as heart failure, respiratory failure, and encephalopathy.39 Aortic root ectasia manifest on echocardiography was only recently recognized in children with mitochondrial cardiomyopathy, even though echocardiography was performed in this population for decades prior.40 Patients with severe forms of AESA likely succumb to complications of AESA before other features of mitochondrial disease manifest. Recognition of AESA as a feature of mitochondrial disease would thus be prevented. Because severe forms of AESA bear a striking similarity to spinal cord AVM/AVF, it is likely that most cases are misdiagnosed because many centers lack the expertise needed to differentiate AESA from AVM/AVF. Moreover, absence of a pre-existing diagnostic framework that accommodates AESA thwarts recognition.
Endothelial dysfunction is believed to be an important feature of mitochondrial arteriopathies, and observational data suggest that intravenous L-arginine infusion may have therapeutic benefits, particularly in patients with mitochondrial encephalopathy experiencing strokelike episodes.41,42 It is possible that L-arginine therapy may be helpful in children with AESA. One patient in this series failed to respond to carnitine supplementation. While carnitine supplementation is commonly administered to patients with mitochondrial disorders because of theoretic biochemical effects, therapeutic efficacy has not been shown outside a subset of patients with mitochondrial myopathy.5,43 Mitochondrial augmentation and transplantation strategies are currently being investigated as a therapeutic approach to mitochondrial diseases.20
An alternative, though a less likely possibility, is that AESA is a transitional form of spinal cord vascular malformation whose developmental progression toward the AVM phenotype has been at least temporarily arrested at an early stage. In animal models, initiation of the brain AVM phenotype begins with angioectasia in precapillary and capillary regions of the developing cerebral circulation, exposing the cerebral microcirculation to an atypical arterial pattern of flow.44 Transition to the brain AVM phenotype occurs when exposure to this anomalous flow signal triggers aberrant developmental programing. It is possible that AESA fails to progress toward the AVM phenotype because precapillary angioectasia is unaccompanied by the aberrant genetic programming needed for the transition. While clinical experience and animal models suggest that the window of developmental vulnerability for the phenotypic transition to AVM is limited to early childhood, longer-term follow-up is needed to determine whether AESA can transform to AVM, given the young age of patients in known cases.44 Although we did not identify genetic markers of dysfunctional vascular biology in our AESA cohort, novel pathogenic mutations in regulatory regions of DNA or copy number mutations cannot be excluded.
Cerebral proliferative angiopathy (CPA), which has been reported as an atypical cerebral AVM phenotype, has some features that overlap with those of AESA.45 The original description of CPA emphasized the presence of “capillary angioectasia” on catheter-directed DSA. The term denotes abnormal enlargement of capillaries. In the setting of catheter-directed DSA, capillary angioectasia is indirectly inferred by the presence of an unusually dense parenchymal capillary blush, accompanied by the brisk appearance of parenchymal draining veins. Thus, capillary angioectasia may be regarded as a feature of AESA. While direct evidence of vascular proliferation with cell-labeling methods was not shown in the original CPA case series, “angioproliferation” was presumed on the basis of transdural vascularization of AVMs and perinidal brain parenchyma. Lasjaunias et al45 suggested that angioproliferative vascular changes in CPA were induced by cerebral ischemia engendered by AVM blood-flow steal. Similarly, in AESA, it is possible that angiopathy is the result of altered blood-flow demand attributable to metabolic derangement within the CNS parenchyma.
In contrast to CPA however, AESA is not associated with transdural vascularization or angioproliferative changes by extension. Moreover, published examples45 of CPA feature a discrete focal intraparenchymal nidal type AV shunt zone demonstrable on MR imaging and catheter-directed DSA. This aspect of CPA sharply differentiates it from AESA, which conspicuously lacks a focal intraparenchymal nidal AV shunt zone where blood circulates directly from arteries to veins without passing through parenchymal capillaries. Moreover, in CPA, catheter-directed angiography shows the vasculature within the intraparenchymal nidal AV shunt zone to be disproportionately ectatic relative to the extraparenchymal feeding arteries, which are frequently small and stenotic. In contrast, diffuse arterioectasia45 involving the extraparenchymal vasculature is the most striking feature associated with AESA.
CONCLUSIONS
AESA is a noninflammatory pathologic vascular manifestation of preschool children characterized by diffuse enlargement and tortuosity of spinal cord arteries, spinal cord hyperemia, and cord edema in the absence of AV shunting. AESA is associated with a highly lethal multisegmental myelopathy that mimics venous congestive myelopathy on MR imaging but which shows distinct pathognomonic findings on catheter-directed spinal DSA. While the clinicopathologic, genetic, and neuroimaging features of AESA overlap with those of mitochondrial disease, the pathogenesis remains uncertain.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received December 28, 2021.
- Accepted after revision April 18, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.