
Abstract
SUMMARY: A spinal CSF-venous fistula is an increasingly recognized type of CSF leak that causes spontaneous intracranial hypotension. The detection of these fistulas requires specialized imaging such as digital subtraction myelography or dynamic CT myelography, and several treatment options are available. A novel treatment for these CSF-venous fistulas consisting of transvenous embolization with the liquid embolic agent Onyx has been described recently, but some patients require further treatment if embolization fails. The purpose of this study was to evaluate the safety and effectiveness of surgery following transvenous embolization. In a series of 6 consecutive patients who underwent surgical ligation of the fistula after endovascular embolization, there were no surgical complications. Postoperatively, complete resolution of symptoms was reported by 5 of the 6 patients, and brain MR imaging findings of spontaneous intracranial hypotension resolved in all patients. This study suggests that surgical ligation of spontaneous spinal CSF-venous fistulas after endovascular embolization is effective and safe.
ABBREVIATIONS:
- DSM
- digital subtraction myelography
- SIH
- spontaneous intracranial hypotension
- SIHDAS
- SIH Disability Assessment Score
Spontaneous intracranial hypotension (SIH) is a condition characterized by low CSF volume in the craniospinal compartment.1 The classic symptom is an orthostatic headache, but numerous other clinical manifestations have been reported.1 With very rare exceptions,2 the cause of SIH is a CSF leak at the level of the spine, and several types of spontaneous spinal CSF leaks have been identified.3 The most recently recognized type of CSF leak is the CSF-venous fistula, which is a type of CSF leak not associated with the presence of extradural CSF and not visible on routine spine MR imaging or CT myelography.3,4 Digital subtraction myelography (DSM) or dynamic CT myelography performed with the patient in the lateral decubitus position is the preferred method to identify these fistulas.5⇓⇓-8 Since the first description of spontaneous spinal CSF-venous fistulas in 2014, many centers around the world have reported success with the identification and treatment of these fistulas.4⇓⇓⇓-8 In addition to epidural blood patching, several specific treatment options are available for these fistulas: percutaneous fibrin sealant injection,9 transvenous embolization,10 and microsurgical ligation of the fistula.7,11 Excellent results with resolution of symptoms and abnormal findings on brain MR imaging have been reported for all 3 of these treatment modalities. Transvenous embolization was first described by Brinjikji et al,10 in 2021, and is the most recently developed treatment option, with excellent results reported in up to 80% of patients.12 Surgical ligation of the CSF-venous fistula is an option if embolization fails. The purpose of this study was to evaluate the safety and effectiveness of an operation following transvenous embolization.
MATERIALS AND METHODS
This study was approved by the Cedars-Sinai Medical Center institutional review board.
Using a registry that has been prospectively maintained since January 2001 at our quaternary referral center for SIH, we identified all patients with SIH who underwent surgical ligation of a CSF-venous fistula following transvenous embolization with Onyx (Covidien). The diagnosis of SIH was based on the criteria of the International Classification of Headache Disorders, third edition,13 with minor modifications. These criteria require objective evidence of SIH, consisting of brain MR imaging showing stigmata of SIH (eg, pachymeningeal gadolinium enhancement or brain sagging), spinal imaging showing a CSF leak (ie, the presence of extradural CSF or a CSF-venous fistula), or low CSF opening pressure (ie, <6.0 cm of CSF). The modification consists of also including patients who do not have headaches but whose symptoms are best explained by SIH.
All patients underwent brain MR imaging and MR myelography (heavily T2-weighted MR imaging). Brain MR imaging was scored for the following findings typical of SIH: subdural fluid collections, enhancement of pachymeninges, engorgement of venous structures, pituitary enlargement, and sagging of the brain.14 Specifics of the MR myelography technique are reported elsewhere.15 For DSM, the technique as described by Hoxworth et al16 was used with some minor modifications. Briefly, DSM is performed with the patient under general endotracheal anesthesia with deep paralysis and suspended respiration for maximal detail and temporal resolution. Patients are positioned in the lateral decubitus position in a biplane angiography suite, with tilt table capability. Pillows or foam padding are placed to optimize the cervicothoracic alignment. A fluoroscopically-guided lumbar puncture is performed with a 22-ga needle. An opening pressure is obtained at this time using standard manometry. Then, an accurate needle position is confirmed with an injection of 0.5 mL of iohexol (Omnipaque; GE Healthcare).
Patients are then further positioned on the basis of the area of interest by tilting the table to achieve contrast flow to the cervicothoracic spine. Great care is taken to maximize contrast opacification of the lateral dural sac by adjusting the degree of tilting to a patient-specific spinal curvature and anatomy. Finally, contrast is injected manually, 1 mL per second, with suspended respiration for 40–120 seconds while acquiring biplane subtraction images at 1–2 frames per second. All imaging studies (ie, brain MR imaging, MR myelography, and DSM) were analyzed by a board-certified neuroradiologist and a board-certified neurosurgeon. Any discrepancies were adjudicated by a second board-certified neuroradiologist.
For transvenous embolization, the technique as described by Brinjikji et al10,12 was used. Briefly, the right common femoral vein was punctured to access the inferior vena cava. A 6F Benchmark guide catheter (Penumbra) was then advanced to the azygous vein with a coaxial technique using an inner 5F Select Berenstein catheter (Boston Scientific) and Terumo guidewire. A double-lumen (Eclipse 2L; MedLine Group) or single-lumen (Scepter XC; MicroVention) balloon microcatheter with a Synchro2 (Stryker) or Hybrid (Balt) microwire was used to access the paraspinal vein at the level of the fistula determined by DSM. The balloon microcatheter was positioned close to the neuroforaminal venous network, and Onyx-18 was injected slowly with the balloon inflated to prevent reflux into the azygous vein.
The surgical technique consisted of a hemilaminotomy and foraminotomy, exposing the lateral common thecal sac and exiting the nerve root sleeve. A titanium Yasargil aneurysm clip (B Braun) was then placed over the fistulous connection, or the fistula was coagulated with bipolar electrocautery if the fistula could be visualized, or a titanium aneurysm clip was placed over the nerve root sleeve without dividing the underlying nerve root. The operation did not require any modification from that used for CSF-venous fistulas not previously treated with endovascular embolization.
All patients (or their family/caregivers) completed a modified Migraine Disability Assessment score questionnaire to assess the severity of the symptoms before and after the last treatment.17 The modification consists of substituting “symptoms of SIH” for “headaches.” We refer to this modified questionnaire as the SIH Disability Assessment Score (SIHDAS) questionnaire. A score of 0–5 (grade I) is considered to equate to little or no disability, 6–10 (grade II) is mild disability, 11–20 (grade III) is moderate disability, and >20 (grade IV) is severe disability.
RESULTS
The mean age of the 4 women and 2 men was 64 years (range, 44–79 years). An orthostatic headache was the principal symptom in 5 patients, and 1 patient presented with coma. Disability as measured by the SIHDAS score varied from mild to severe (SIHDAS score grade II in 2 patients, grade III in 2 patients, and grade IV in 2 patients). The initial brain MR imaging findings were normal in 1 patient and showed the typical changes of SIH in 5 patients. The MR imaging findings consisted of pachymeningeal enhancement only in 1 patient; pachymeningeal enhancement and pituitary enlargement in 1 patient; pachymeningeal enhancement, venous dilation, and pituitary enlargement in 1 patient; subdural hematomas, pachymeningeal enhancement, pituitary enlargement, and brain sagging in 1 patient; and pachymeningeal enhancement, venous dilation, pituitary enlargement, and brain sagging in 1 patient. All patients had undergone bilateral lateral decubitus DSMs. Opening pressures ranged from 4 to 15 cm of CSF (<6 cm of CSF in 2 patients). Four patients had a single CSF-venous fistula, and 2 patients had bilateral CSF-venous fistulas for a total of 8 CSF-venous fistulas: Three fistulas were right-sided, and 5 fistulas were left-sided (Fig 1). All CSF-venous fistulas were located in the thoracic spine. Epidural blood patching was the initial treatment in all patients, with excellent-but-temporary relief of symptoms in 4 patients, and no symptom improvement in 2 patients. Six of the 8 CSF-venous fistulas in 6 patients were treated with transvenous embolization. The other 2 CSF-venous fistulas were treated with only surgical ligation before the development of embolization as a treatment technique. The operation following endovascular treatment was performed between July 2021 and February 2022.

Lateral decubitus DSMs showing 8 spontaneous spinal CSF-venous fistulas (arrows) in 6 patients. A, A right T8 fistula. B, A left T1 fistula. C, A left T8 fistula. D, A right T5 fistula. E, A left T7 fistula. F, A left T6 fistula. G, A left T11 fistula. H, A right T3 fistula. A and B and C and D, Bilateral fistulas in 2 patients. Multiple CSF-venous fistulas are found in about one-tenth of patients.18
Transvenous embolization was performed at our institution in 5 patients and at another institution in 1 patient. In 1 patient, the targeted paraspinal vein thrombosed during the embolization procedure, and Onyx could not be delivered. Onyx was successfully delivered in the other 5 patients, including within the veins of the neural foramen in 4 patients (Fig 2). There were no procedural complications, and all patients reported initial improvement of symptoms, including the patient with paraspinal vein thrombosis. After recurrence of symptoms, DSM was repeated in 3 of the 6 patients before surgical ligation of the recurrent/residual CSF-venous fistula (Fig 3). There was no evidence of recruitment of fistulous vascular connections from adjacent spinal levels.

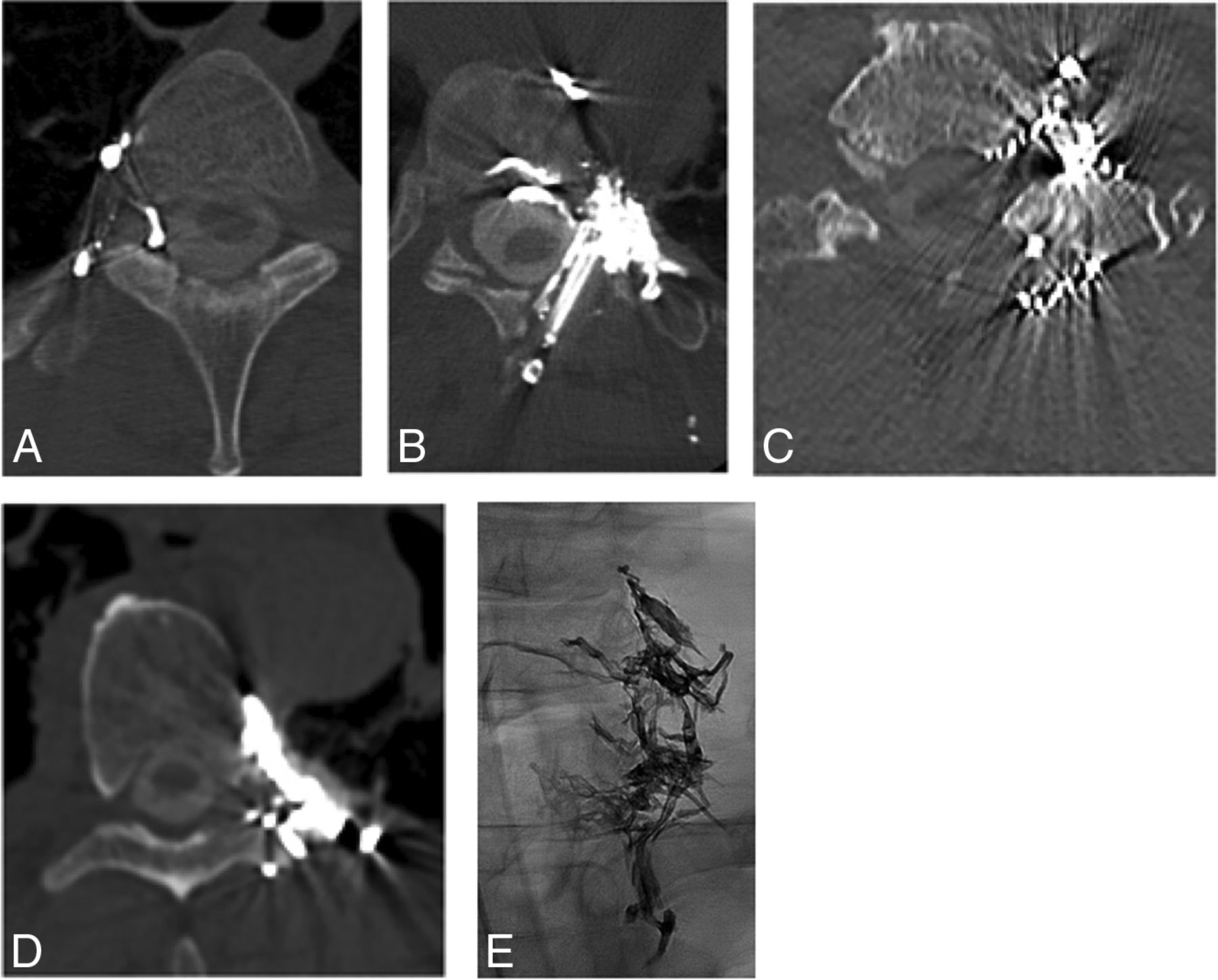
Post-transvenous embolization CT scans (A–D) and an anterior-posterior radiograph (E) showing Onyx within the neural foramen in 4 patients (A–C and E) and just outside the neural foramen in 1 patient (D). The CT scan in B shows the results after surgical clip ligation following transvenous embolization.

A and B, Pre-transvenous embolization lateral decubitus DSM and post-transvenous embolization lateral decubitus DSM showing a residual/recurrent CSF-venous fistula. Anterior-posterior post-transvenous embolization radiograph (C) shows the distribution of intravascular Onyx.
An operation was performed between 1 and 6 months after the transvenous embolization (mean, 5 months). At the operation, variable amounts of Onyx could be visualized surrounding the nerve root sleeve in all 4 patients who had Onyx delivered within the neural foramen (Fig 4). The Onyx-filled vasculature was compressible and was easily resected from around the nerve root sleeve. These maneuvers allowed unobstructed visualization and clip placement over the nerve root for noneloquent thoracic nerve roots (3 patients) and direct visualization and subsequent clip placement and bipolar coagulation of the fistulous site itself for a CSF-venous fistula of the first thoracic nerve root in 1 patient. Uneventful clip ligation of the nerve root was also recorded for the 2 patients who did not have Onyx delivered within the neural foramen. There were no surgical complications and resolution of symptoms was reported by 5 of the 6 patients (grade I on the SIHDAS scale), while 1 patient had residual symptoms of SIH (grade III on the SIHDAS scale). Clinical follow-up ranged from 1 to 6 months (mean, 4 months). Before the surgical procedure, brain MR imaging findings had normalized in 3 of the 6 patients. Postoperatively, resolution of brain MR imaging findings of SIH was noted for the remaining 3 patients as well.

Intraoperative photograph showing Onyx (arrows) within the epidural veins.
DISCUSSION
Patients and their health care providers are fortunate that the armamentarium for treating spontaneous spinal CSF-venous fistula is expanding. In the absence of any data from robust randomized trials, it is likely that all 3 specific treatment options will remain viable, at least in the foreseeable future. In this study, we found that an operation after transvenous embolization is effective and safe. Complete symptom resolution was obtained in all except 1 patient, and there were no surgical complications.
The best results of transvenous embolization are obtained when Onyx is placed within the veins of the neural foramen. Onyx is an intravascular embolic agent that is permanent and could hinder surgical dissection around the nerve root sleeve. We found that at the operation, the Onyx was compressible and easily resectable, allowing undisturbed surgical dissection and clip ligation of the fistula. Another concern of embolization is that with subtotal occlusion of the fistula, recruitment of new fistulous connections could occur at adjacent spinal levels, but we did not observe that in any of the presently reported patients who underwent repeat DSM following unsuccessful embolization before surgical clip ligation.
Our study has several limitations. It represents a highly selected group of patients referred to a quaternary referral center for SIH, and the generalizability of our findings is unknown. The number of patients was relatively small, and follow-up ranged from only 1 to 6 months. However, transvenous embolization of spontaneous spinal CSF-venous fistulas is a recently developed technique that was first reported in 202110 and was first used in our institution in February 2021.
CONCLUSIONS
In this series of patients with SIH who underwent surgical ligation of a spinal CSF-venous fistula following transvenous embolization, surgery was effective and safe.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received March 30, 2022.
- Accepted after revision May 9, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CSF-Venous Fistula Transvenous Onyx Embolization: Evaluation of Onyx Migration into the CSF and Potential One-Way Physiology
- Clinical and imaging outcomes of 100 patients with cerebrospinal fluid-venous fistulas treated by transvenous embolization
- Spinal CSF Leaks: The Neuroradiologist Transforming Care
- Transvenous embolization of cerebrospinal fluid-venous fistulas: Independent validation and feasibility of upper-extremity approach and using dual-microcatheter and balloon pressure cooker technique