
Abstract
BACKGROUND AND PURPOSE: Dominant radiculomedullary arteries such as the artery of lumbar enlargement and the artery of cervical enlargement are well-documented. However, variability exists as to the size, number, and location of other radiculomedullary arteries contributing supply to the anterior spinal artery. The aim of this anatomic study was to document the prevalence and characteristics of the dominant anterior thoracic artery in cadaveric specimens.
MATERIALS AND METHODS: Microsurgical dissection of cadaveric human spinal cord specimens (n = 50) was conducted. The artery of lumbar enlargement was injected with colored latex until the small-caliber arterial vessels were filled. The dominant anterior thoracic artery was identified, injected, and filled with diluted industrial paint. The course, diameter, and location of the dominant anterior thoracic artery, artery of lumbar enlargement, and artery of cervical enlargement were documented.
RESULTS: The artery of lumbar enlargement was identified between T3 and L2 in all 50 specimens (100%), and the artery of cervical enlargement was identified in 84% of specimens (42/50). At least 1 dominant anterior thoracic artery distinct from the artery of lumbar enlargement and the artery of cervical enlargement was identified between T1 and T11 in 47 of the 50 specimens (94%). The most frequent origin of the dominant anterior thoracic artery was at the level of T4 on the left. The average size of the dominant anterior thoracic artery was 0.446 mm (range, 0.300–0.759 mm on the left and 0.270–0.569 mm on the right).
CONCLUSIONS: A dominant anterior thoracic artery is present in 94% of individuals. Variations of the arterial supply to the anterior thoracic cord are of great importance due to their implications for ischemic events as well as surgical and endovascular procedures.
ABBREVIATIONS:
- ACE
- artery of cervical enlargement
- ALE
- artery of lumbar enlargement
- ASA
- anterior spinal artery
- DATA
- dominant anterior thoracic artery
- RMA
- radiculomedullary artery
Variations of the arterial supply to the anterior thoracic cord are important due to their implications for ischemic events as well as surgical and endovascular procedures. Radiculomedullary arteries (RMAs) represent the dominant arterial supply to the spinal cord and are the sole segmental supply to the anterior spinal artery (ASA) along the ventral cord.1 The ASA ranges from 0.2 to 0.8 mm and has an inconstant caliber along its length.2⇓-4 The fluctuating size is related to the variable number of RMAs specifically providing arterial supply to the ventral cord.4,5 The number, caliber, and entrance level of the anterior RMAs have been previously studied6⇓-8 and ranges in number from 2–14.2
Dominant radiculomedullary and radiculopial arteries such as the artery of lumbar enlargement (ALE),2⇓-4 the artery of cervical enlargement (ACE),1 and the great posterior radiculomedullary artery8 are well-documented. Historically, 2 RMAs have received the most consideration. In the lower thoracic or upper lumbar region, the dominant and most important radiculomedullary supply is the ALE, otherwise known as the arteria radiculomedullaris magna or, more commonly, the artery of Adamkiewicz.2⇓-4 The ALE arises between T8 and L2 in 75% of individuals with a diameter ranging between 0.5 and 1.2 mm.2,3 The largest anterior cervical radiculomedullary branch is generally in the region of C5 through C6 and has been termed the ACE.1 Although dominant RMAs such as the ALE and ACE are well-documented, variability exists as to the size, number, and location of other RMAs contributing supply to the ASA. Because RMAs other than the ALE have a considerably smaller diameter, they are difficult to identify on imaging, including angiography. Traditionally, RMAs arising from upper thoracic segmental arteries are generally regarded as branches only rarely present and therefore of little clinical significance. This notion has led to the commonly taught and widely held belief that the anterior thoracic arterial system represents a watershed territory.
A spinal angiography study conducted in 50 individuals identified a significant upper thoracic anterior RMA distinct from the ALE in 86% of patients.9 Due to the relatively constant nature of this artery, the author suggested naming this vessel the artery of von Haller. This was proposed in honor of Albrecht von Haller, who documented the arterial supply to the ASA including this vessel as well as the ALE in 1754,5,10 more than a century before Albert Adamkiewicz11,12 and Kadyi.13 However, instead of the artery of von Haller, we opted to refer to this vessel as the dominant anterior thoracic artery (DATA) so that the name could provide easy recognition and support more reliable terminology. The DATA has attracted little attention in the literature, and its importance is not widely known or taught. In addition, its angiographic identification is quite difficult due its caliber as well as obscuration by overlying structures, including osseous and muscular arterial branches as well as the trachea.9 The aim of this anatomic study was to analyze the arterial supply to the ventral spinal cord and determine the prevalence of the DATA along with its morphometric characteristics in cadaveric specimens.
MATERIALS AND METHODS
We conducted an institutional review board–approved study of 50 (49 male and 1 female) cadaveric specimens at the Institute of Forensic Sciences of Mexico City (Instituto the Ciencias Forenses de la Ciudad de Mexico). The cadavers ranged from 22 to 70 years of age, with a median age of 45 years. Spinal cord extraction was conducted after a posterior midline longitudinal incision from the occiput to the sacrum as well as laminectomies throughout the entirety of the cervical, thoracic, and lumbar spine. The spinal nerves were then cut with great care so as not to lesion the dura. Ventral and dorsal longitudinal midline durotomies were subsequently performed, and the spinal cord was irrigated with saline. To remove residual intravascular blood, the vascular system was irrigated with saline. After completing these steps, the ALE was identified, an angiocatheter of commensurate size was selected for cannulation, and injection of red natural latex was performed. Injection was conducted with close visual inspection and under moderate pressure in an attempt to prevent vessel rupture and contrast extravasation. The DATA was identified, and a microcatheter of commensurate size was selected to inject and fill this vessel with diluted industrial red paint. Diluted industrial paint was used in this step because natural latex was too viscous to fill vessels of this small caliber. We proceeded until latex and paint filled distal small-caliber arterial vessels. The specimens were then fixed in a 5% formaldehyde solution for 2 weeks. The spinal cord specimens were then studied with the aid of 5x surgical loupes. The ALE, the ACE, and any thoracic RMAs consistent with the DATA were identified and documented. Measurements were obtained with digital Vernier calipers. Digital photographic images were obtained including a measurement scale to corroborate caliper measurements with digital measurements.
RESULTS
No vascular malformations, fistulas, or other vascular abnormalities were identified in any of the specimens.
In only 3 specimens (3/50) was the DATA not identified. At least 1 DATA was evident in 94% of spinal cord specimens (47/50). A single DATA was present in 66% of the specimens (33/50) (Fig 1). Two DATAs were identified in 26% (13/50) (Fig 2). Three DATAs were identified in a single (1/50) specimen (2%), all arising on the left at the level of T3, T7, and T9. The laterality and spinal level of the DATA are summarized in Fig 3. A DATA was most frequently identified at the level of T4, with 15 left- and no right-sided specimens identified at this level. The average DATA size was 0.446 mm, with a range of 0.300–0.759 mm on the left and 0.270–0.569 mm on the right.

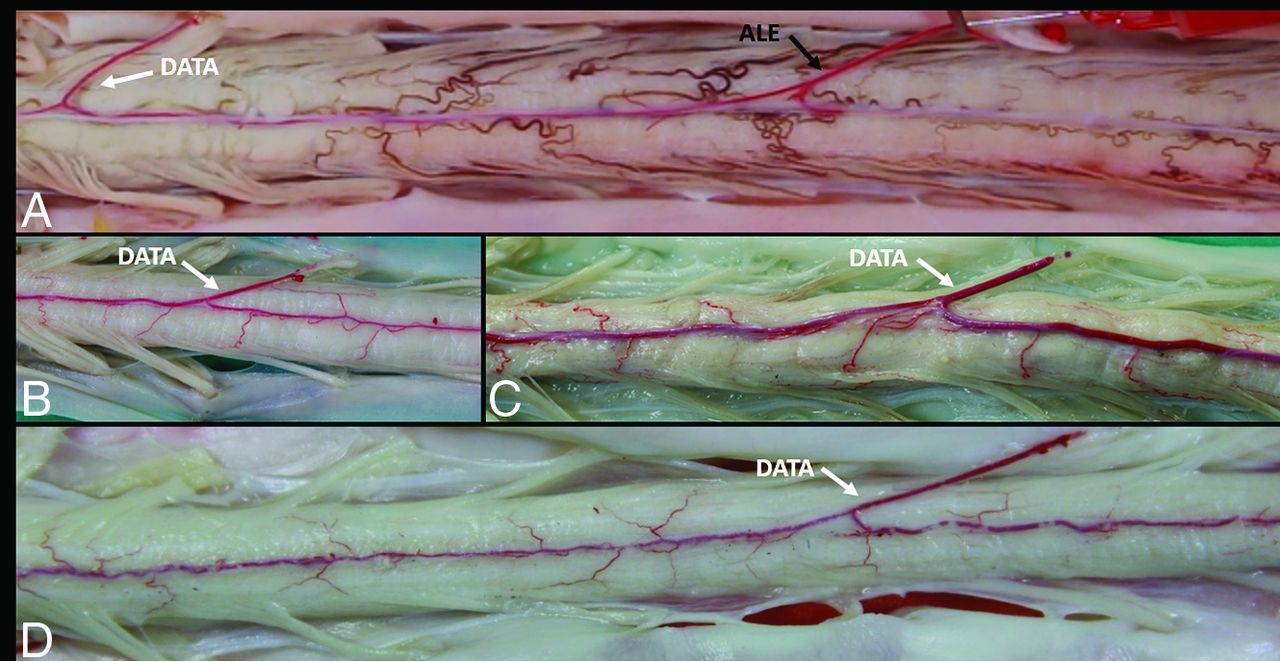
Single DATA. The anterior view of the spinal cord during arterial injection (A) clearly shows a T9 ALE (black arrow) as well as a single T4 DATA (white arrow), the most common level in our analysis. Three other specimens after fixation (B–D) clearly demonstrate a single dominant upper thoracic anterior RMA supplying the ASA, consistent with a DATA (white arrows).

Two DATAs. The anterior view of the spinal cord clearly reveals evidence of the ALE (black arrow) as well as 2 left-sided DATAs consistent with 2 separate DATAs (white arrows) supplying the ASA.

Distribution, number, and side of the ACE, DATA, and ALE.
The ALE was identified between T3 and L2 in all 50 spinal cords (100%). A left-sided ALE was present in 44 specimens, and a right-sided ALE was present in 6 specimens. The most proximal ALE was evident at the level of T3 on the left, and the most distal, at the level of L2 on the left. The side and spinal level of ALEs are summarized in Fig 3. On average, the diameter of the ALE was 0.83 mm, with the smallest caliber ALE measuring 0.49 mm and the largest measuring 1.21 mm.
The ACE was identified in 84% of specimens (42/50). A single ACE was present in 20 specimens; 2 separate ACEs, in 12 specimens; 3 ACEs, in 6 specimens; and 4 ACEs, in 4 specimens. A total of 78 ACEs were, therefore, documented, with 38 on the left and 40 on the right. The most proximal ACE was evident at the level of C2, and the most distal, at the level of C8. The side and spinal level of the ACEs are summarized in Fig 3. On average, the diameter of the ACE was 0.49 mm, with the smallest caliber ACE measuring 0.13 mm and the largest measuring 0.73 mm. In the 8 specimens in which no ACE was identified, the DATA originated at T2 in 2 specimens, T3 in 3 specimens, T4 in 1 specimen, and T8 in 2 specimens.
DISCUSSION
Our results demonstrate that a DATA is present in most individuals (94%). Our findings are similar but more robust than those in the study of Gailloud,9 in 2013, in which a total of 43 of 50 patients (86%) had at least 1 RMA branch between T3 and T7, with a single anterior branch in 68% (34/50), 2 anterior branches in 18% (9/50), and none with 3 anterior branches. In contrast, we found a single DATA in 66% (33/50), 2 in 26% (13/50), and 3 in 2% (1/50). Improved detection in our cadaveric findings is likely due to increased sensitivity and accuracy because the upper thoracic RMAs may be obscured by overlying osseous or muscular branches on spinal angiography.
Although the caliber of the DATA did not approximate that of the ALE, the vessels were truly dominant and easily distinguished from the tiny caliber of the radicular arteries that accompany spinal nerves. Of note, no absolute cutoff measurement was used to establish the presence of a DATA because establishing the presence of a dominant arterial feeder is a relative process specific to each individual. For instance, paucisegmental and plurisegmental ASA circulations are associated with markedly differing calibers of the ALE.
Although naming RMAs is necessarily arbitrary in nature, the presence of an ALE, ACE, and DATA in 42 of our specimens validates the naming of each of these vessels. In other words, the dominant upper thoracic RMA in a specimen clearly demonstrating an ALE and an ACE is best regarded as a DATA rather than a high-origin ALE or a low-origin ACE. Furthermore, in the 8 cases in which we did not identify an ACE, the DATA distribution from T2 through T8 did not demonstrate a high thoracic clustering, arguing against naming all these vessels as low-origin ACEs. In particular, it is difficult to justify the classification of the cases with no ACE and a DATA at either T4 or T8 as a low ACE variant instead.
These results are contrary to the notion that in most individuals, there is a thoracic spinal cord watershed zone at risk of ischemia. The presence of a DATA in most individuals counters the erroneous belief that there is a poorly arterialized thoracic segment. Instead, the concept that in most individuals there are at least 3 dominant RMAs such as the ALE, ACE, and DATA should be endorsed and taught during anatomic discussions (Fig 4). Our results have implications for reducing the risk of arterial spinal and aortic surgical and endovascular procedures. In particular, our findings are important for addressing vascular malformations of the spinal cord. The degree of involvement of the DATA in spinal cord pathology has yet to be studied, and we believe this would be a fruitful area for future research.

Dominant RMAs. In most individuals, at least 3 dominant RMAs exist and include the ALE, ACE, and DATA as illustrated and labeled above. The DATA is shown on the left at the level of T4, the most common side and level in our study. a. indicates artery.
The number of specimens we examined supports the reliability of our vessel distribution, laterality, and diameter determinations. However, because most of our anatomic specimens were from male cadavers, we cannot exclude the unlikely possibility that sex differences exist. In addition, the possibility of racial variations cannot be excluded on the basis of this study.
CONCLUSIONS
A DATA is conclusively present in most individuals (94%). A more robust understanding of the intricate spinal arterial anatomy and its variations is critical for endovascular procedures. A better appreciation of the spinal cord circulation will lead to a reduced risk of surgical and endovascular spinal and aortic procedures.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 31, 2022.
- Accepted after revision October 25, 2022.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.