
Abstract
SUMMARY: Susac syndrome is a rare disorder affecting the brain, retina, and inner ear, probably triggered by an immune-mediated endotheliopathy. Diagnosis is based on clinical presentation and ancillary test findings (brain MR imaging, fluorescein angiography, and audiometry). Recently, vessel wall MR imaging has shown increased sensitivity in the detection of subtle signs of parenchymal, leptomeningeal, and vestibulocochlear enhancement. In this report, we describe a unique finding identified using this technique in a series of 6 patients with Susac syndrome and discuss its potential value for diagnostic work-up and follow-up.
ABBREVIATIONS:
- SuS
- Susac syndrome
- VW-MRI
- vessel wall MR imaging
Susac syndrome (SuS) is a rare disorder affecting the brain, retina, and inner ear.1 Although the underlying pathogenesis is not clear, it is thought to be an immune-mediated endotheliopathy affecting precapillary arterioles, causing microvascular occlusion and multiple microinfarcts in involved territories.2
It predominantly affects young adults, particularly women.3 The classic clinical triad comprises encephalopathy, with or without focal neurologic deficits; sensorineural hearing loss; and visual disturbance secondary to branch retinal artery occlusions. However, the complete triad is present in only 13%–27% of patients at disease onset.3
SuS diagnosis is based on clinical presentation and evidence of brain, retinal, and vestibulocochlear involvement on brain MR imaging, fluorescein angiography, and audiometry.4 The main neuroimaging findings are multifocal, T2 FLAIR hyperintense white matter lesions with hallmark imaging patterns known as “snowballs,” “spokes,” “icicles,” and “string of pearls.”5 Fluorescein angiography shows arterial wall hyperfluorescence and branch retinal artery occlusions, and audiometry detects sensorineural hearing loss even in asymptomatic patients.4,5
Vessel wall MR imaging (VW-MR imaging) is based on black-blood 3D T1-weighted sequences, enabling selective suppression of blood signal with high spatial resolution and a high contrast-to-noise ratio.6 Although initially developed to depict intracranial vessel walls, it has demonstrated greater sensitivity in showing subtle leptomeningeal as well as parenchymal and vestibulocochlear enhancement, compared with gradient-echo and spin-echo sequences.7⇓-9
The aim of this study was to assess findings on contrast-enhanced VW-MR imaging in a cohort of patients with SuS. To this end, we reviewed institutional electronic medical records (between July 1, 2017, and October 1, 2022) in search of patients with definite or probable SuS according to the criteria proposed by Kleffner et al,10 who had at least 1 contrast-enhanced VW-MR imaging study acquired at any stage of the disease. Of the 6 patients included, 4 had definite and 2 had probable SuS diagnoses (3 women and 3 men; mean age, 36.3 years; age range, 19–57 years). All patients were subject to extensive work-up to exclude other possible conditions such as demyelinating syndromes, encephalitis, and vasculitis. VW-MR images were evaluated blinded to clinical data, by a fourth-year resident (P.C.) and a neuroradiologist (H.C.) with >10 years’ experience, who has read >130 VW-MR imaging studies in the past 5 years.
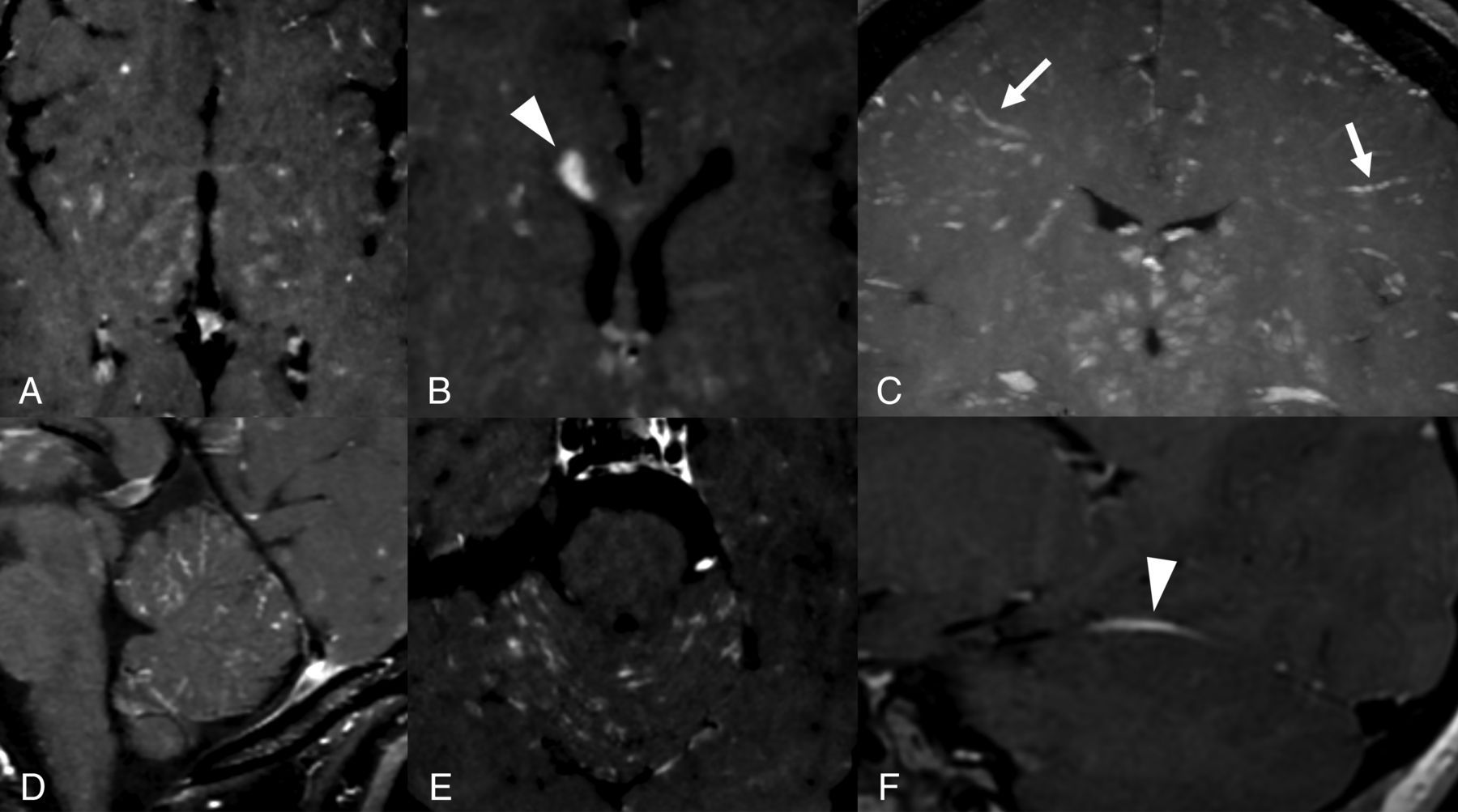
Main demographic, clinical, and VW-MR imaging findings are summarized on in the Online Supplemental Data. MR imaging scanner characteristics and T1-weighted vessel wall imaging sequence parameters are summarized on in the Online Supplemental Data. Contrast enhancement on VW-MR imaging was visible in 5 patients, with different patterns and distributions (Fig 1 and Online Supplemental Data). In 4 patients, multiple, short, linear foci of leptomeningeal interfoliar enhancement were observed in both cerebellar hemispheres (Fig 2). Additionally, contrast enhancement was more conspicuous on VW-MR imaging compared with 3D-FLAIR and 3D gradient-echo T1-weighted images (Online Supplemental Data). In one patient who had treatment initiated before the MR imaging acquisition, no enhancement was detected, and in another patient, follow-up VW-MR imaging after 1 year of treatment showed complete remission of parenchymal and leptomeningeal enhancement observed at symptom onset (Online Supplemental Data).

Different patterns of enhancement on VW-MR imaging: punctuate (A), focal (arrowhead, B), perivascular (arrows, C), leptomeningeal (D and E), and pachymeningeal (arrowhead, F). Images A, B, D, and E correspond to patient 2, and C and F, to patient 1.

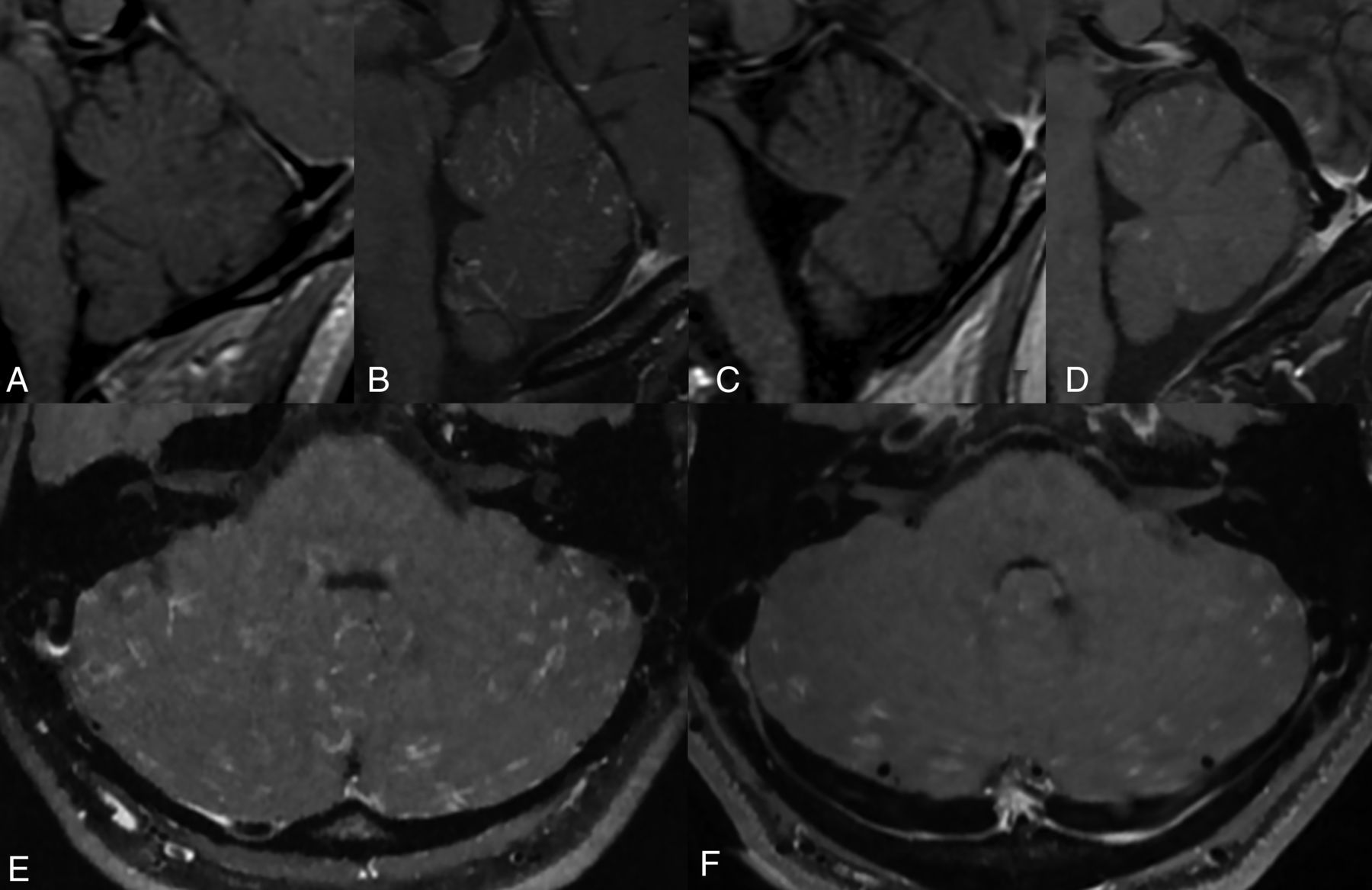
Interfoliar leptomeningeal enhancement on VW-MR imaging. Multiple thin, short, enhancing foci scattered along the folia of the cerebellar vermis and hemispheres. Patient 1 (A), patient 2 (B and E), patient 3 (C), and patient 6 (D and F).
DISCUSSION
Existing evidence describes classic neuroimaging features of SuS as white matter lesions, microinfarcts, and central callosal lesions. Gadolinium enhancement has also been considered a recurrent feature, presenting different patterns, including punctate or focal, and locations: perivascular, leptomeningeal, pachymeningeal, and cochleovestibular.11,12
Although previous literature has demonstrated the higher reliability of contrast-enhanced FLAIR compared with contrast-enhanced T1, no study to date has examined the diagnostic performance of VW-MR imaging in patients with SuS.13⇓-15 Only a limited number of reports have found that VW-MR imaging had higher sensitivity in distinguishing cases of SuS from other vascular conditions.11,12,16 Several authors have, however, described the greater sensitivity of VW-MR imaging compared with gradient-echo and spin-echo sequences for the detection of leptomeningeal and subtle parenchymal enhancement in other pathologies.7⇓-9
Leptomeningeal enhancement is a recurrent feature of SuS. Most interesting, we detected a unique pattern of diffuse, infratentorial, interfoliar enhancement in 4 patients, not previously described in other conditions, consisting of multiple thin, short, enhancing foci scattered along the folia of the cerebellar vermis and hemispheres. Cerebellar leptomeningeal enhancement seen in meningitis or carcinomatosis differs from this pattern, tending to be more contiguous and/or thicker.
Additionally, a recent report by Baskin et al16 presented a case of gadolinium-enhancement resolution of VW-MR imaging after immunotherapy. We observed 2 similar cases, one with no enhancement on VW-MR imaging in a patient already receiving corticosteroid therapy and another in whom parenchymal and leptomeningeal enhancement resolved after immunosuppressive therapy.
No patient in this series or in other published reports showed arterial vessel wall enhancement, possibly because SuS affects small-caliber vessels (precapillary arterioles) not detected using current VW-MR imaging techniques.
Taken together, this evidence suggests that acute inflammation could be the pathologic substrate underlying VW-MR imaging findings, and leptomeningeal enhancement could represent a marker of disease activity. It remains unclear whether an association exists between this enhancement pattern and severity or even triggering of the disease.
On the basis of the increased sensitivity and presumed high specificity of VW-MR imaging, we believe that this imaging technique will improve both the SuS diagnosis and monitoring of treatment response during follow-up. Larger diagnostic accuracy studies will, however, be needed to confirm this hypothesis, given the limited number of patients included in our study.
Although evidence on VW imaging in SuS remains scarce, emerging data showing similar findings from different groups worldwide support the use of this sequence as a diagnostic tool for SuS.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received December 7, 2022.
- Accepted after revision January 30, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.