
Abstract
SUMMARY: Lateral dural tears as a cause spontaneous intracranial hypotension occur in ∼20% of patients. Common imaging modalities for their detection are lateral decubitus digital subtraction myelography or dynamic CT myelography. Reports on the use of conebeam CT are scarce. We show 3 patients in whom the targeted use of conebeam CT during digital subtraction myelography was helpful in confirming the site of the leak.
ABBREVIATIONS:
- CBCT
- conebeam CT
- DCTM
- dynamic CT myelography
- DSM
- digital subtraction myelography
- SIH
- spontaneous intracranial hypotension
- SLEC
- spinal longitudinal extradural CSF collection
Spontaneous intracranial hypotension (SIH) typically causes orthostatic headaches but can also lead to serious impairment, with coma as the most severe complication.
Patients with SIH who show a spinal longitudinal extradural CSF collection (SLEC) on MR imaging of the spine usually have an underlying ventral (type 1 leak) or lateral dural tear at the site of the nerve root sleeve (type 2 leak); patients negative for SLEC, on the other hand, may have a CSF-venous fistula.1
Patients positive for SLEC who are suspected of having a lateral dural tear undergo either digital subtraction myelography (DSM), usually in the angiography suite, or dynamic CT myelography (DCTM) with multiple scans with the patient in the lateral decubitus position. Today, there is no consensus on which method is more beneficial for detecting type 2 leaks. The radiation dose has been reported to be 3-fold higher in DCTM2 but may provide better spatial coverage and resolution. However, conebeam CT (CBCT) may offer comparable cross-sectional images by flat panel detector in the angiographic suite but was only reported once showing spinal dural tears.3 It seems reasonable to start diagnostics with a less radiation-intensive technique with high temporal resolution such as DSM and supplement it with targeted use of CBCT in the same session to confirm or exclude unclear findings by providing 3D images. This approach combines the best features of the 2 techniques, DSM and DCTM, potentially resulting in higher spatial resolution and a lower overall radiation dose.
In this brief report, we focus on type 2 leaks only. We demonstrate 3 patients in whom CBCT was helpful in detecting a lateral leak during DSM and discuss all 3 different imaging techniques.
Cases
Case 1.
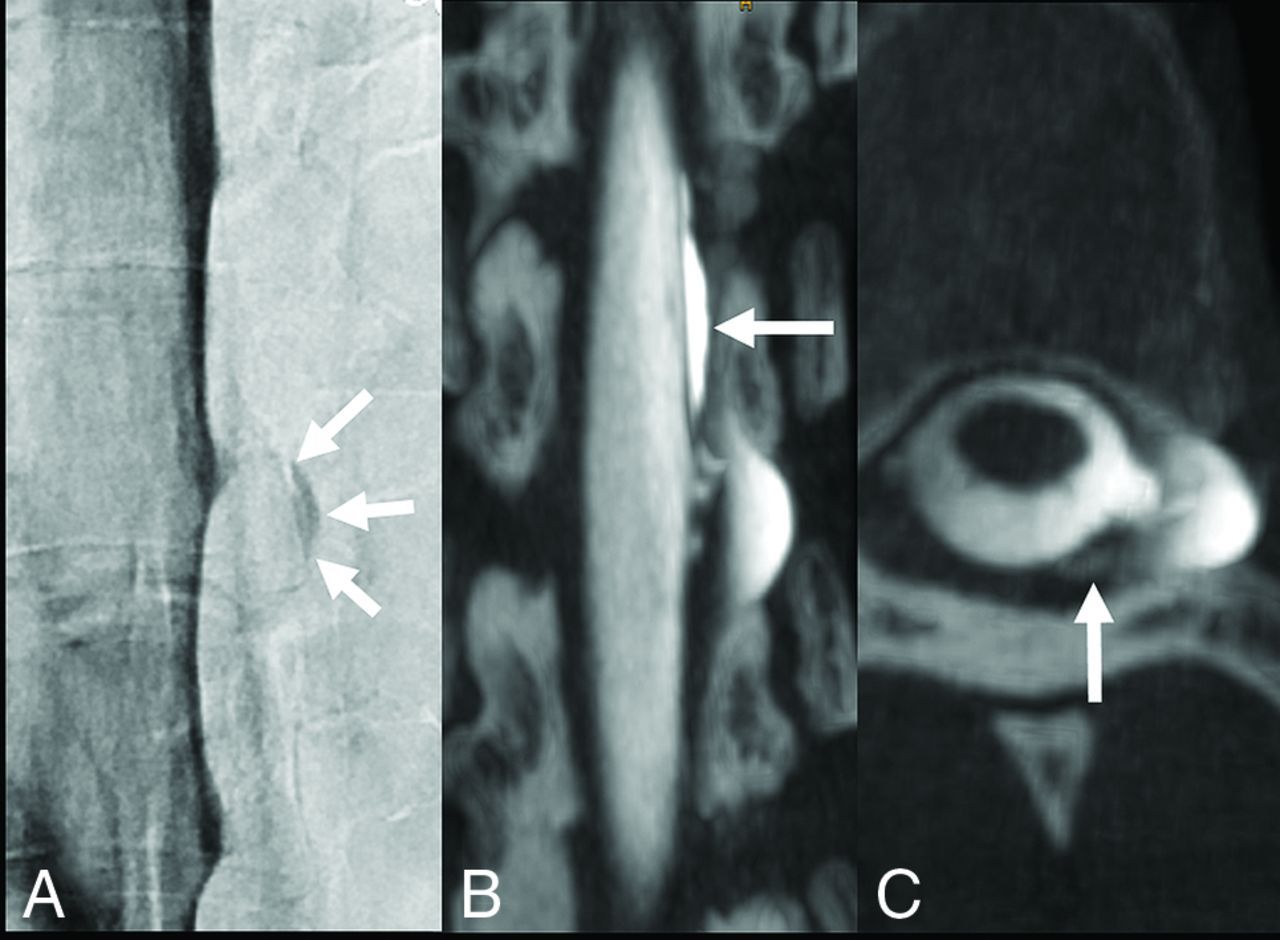
A 47-year-old man was admitted to a local hospital with confusion and personality changes. Bilateral subdural hematomas were detected on cranial CT and surgically treated. Due to the young age of the patient, we performed an MR imaging of the spine, revealing an SLEC. However, MR imaging of the head disclosed only minimal postoperative findings and a Bern SIH score of 1, and the patient could not recall the orthostatic headache.4 Because there were suspicious nerve root sleeve diverticula at the L1/2 level on both sides, we performed a DSM on the left and subsequently on the right side, each followed by CBCT (Fig 1). Imaging findings were subtle, most likely due to a slow-flow leak and only visible on CBCT. Intraoperative findings confirmed a lateral dural tear on both sides. After surgical repair, no recurrence of subdural hematomas was noted at the last clinical follow-up at 2 months.

A 47-year-old man with SIH, resulting in bilateral subdural hematomas. DSM with the patient in left lateral decubitus position does not demonstrate a contrast extradural outflow at the level of a suspicious meningeal diverticulum at L1/2 (A). Subsequent CBCT in a coronal reconstruction reveals a subtle extradural contrast collection next to the diverticulum (arrows in B), confirming a slow-flow type 2 leak. The high spatial resolution of CBCT also indicates an accompanying arachnoid outpouching with an interrupted dura (medial-cranial to the asterisk in B), appearing like a meningeal diverticulum (later confirmed by surgery). CBCT settings are the following: 3D-(5sDCT Body), 49-cm zoom, 90 kV, 544 mA, 90 images/sec in a 4.83-second runtime (397 total images).
Case 2.
A 37-year-old woman presented with typical orthostatic headache. MR imaging of the head from an outside hospital showed a high probability of SIH (Bern SIH score 9), an SLEC on spinal MR imaging, and a suspicious left-sided dorsal dural tear at the T7/8 level on DCTM. An epidural blood patch initially improved symptoms and imaging (Bern SIH score 2), but the SLEC persisted on MR imaging 11 months later. Accordingly, the patient asked for closure of the leak. We repeated imaging with the patient in the left lateral position, but only, the subsequent CBCT demonstrated the contrast outflow (Fig 2B, -C), which was most likely superimposed during previous biplane DSM. CBCT suggested that the leak at T7/8 might originate from the nerve root sleeve, which was confirmed by surgery. Six weeks later, the Bern SIH score was zero, and the patient had recovered completely at clinical follow-up after 2 months.

A 37-year-old woman with SIH and a persistent SLEC on MR imaging of the spine months after the epidural blood patch. Anterior-posterior DSM with the patient in the left lateral decubitus position shows a slightly contrast-filled prominent diverticulum at T7/8 (arrows in A) without extradural contrast egress. Coronal CBCT clearly demonstrates an epidural contrast collection (arrow in B) next to the diverticulum. Axial CBCT shows a type 2 leak with more posterior contrast leakage (arrow in C) (caused by encapsulation and neomembranes as reported from the operation), previously not visible on DSM due to superimpositions. CBCT settings are the following: 3D-(4sDCT Body Care), 49-cm zoom, 90 kV, 134 mA, 90 images/sec in 3.53-second runtime (248 total images).
Case 3.
A 26-year-old woman presented with a variety of symptoms, starting with head and neck pain, later accompanied by dizziness, nausea, and photosensitivity. The Bern SIH score was 7, and spinal MR imaging showed an SLEC. DSM revealed unclear findings next to a suspicious diverticulum (Fig 3A, -B), most likely due to a slow-flow leak. Immediately, supplemented CBCT and subsequent surgery confirmed the lateral leak at L1/2 right side (Fig 3C). The SLEC disappeared on spinal MR imaging 6 weeks after the operation, and symptoms completely resolved after 4 months of clinical follow-up.

A 26-year-old woman severely impaired by SIH. DSM with the patient in a right lateral decubitus position shows a small but remarkable diverticulum at the L1/2 level. A subtle contrast flickering is visible at the bottom of the diverticulum (arrow in A). Delay single x-ray shows a faint hyperdense line as a questionable indication of extradural contrast outflow (arrow in B). Subsequent CBCT in a coronal reconstruction confirms the findings as a type 2 leak (arrow in C). CBCT settings are the following: 3D-(4sDCT Body Care) 49-cm zoom, 90 kV, 404 mA, 90 images/sec in 3.53-second runtime (248 total images).
MATERIALS AND METHODS
In all patients, DSM and CBCT were performed on a flat panel detector unit (Artis icono biplane; Siemens) with the patients in the lateral decubitus position while awake, with ∼10 mL of contrast agent (300 mg iodine/mL). DSM settings in all patients were the following: 60-second run (1 frame per second) with additional fluoroscopy and single x-ray imaging. For DSM, the table was tilted 6°–8° head down, and patients continued shallow breathing. Settings for the CBCT slightly differed among patients and were, therefore, specified in the legend of each figure. For CBCT, the table was returned to horizontal to avoid contrast agent runoff, and patients held their breaths during the CBCT acquisition (4- to 5-second run).
DISCUSSION
In this report, we demonstrate the value of cross-sectional CBCT to detect type 2 leaks in 3 patients. These leaks were not detectable on DSM, either due to their slow flow or low volume, respectively, or superimposition of the thecal sac.
DSM is a technique comprising series with and without subtraction and may be supplemented by fluoroscopy and single x-rays. The temporal and spatial resolution (0.2 mm) is excellent, and the radiation dose is only one-third of the dose in DCTM.2 It allows full control over the intrathecal contrast column (by gradually tilting the table). Downsides are planar rather than cross-sectional images and limited detector coverage. Motion artifacts during DSM may be an issue. However, because type 2 leaks are usually located in the less-breath-dependent lower spine,1 motion artifacts are often minimized with continuous shallow breathing. As reported previously, this technique is well-suited for high-flow leaks.5 In our experience, approximately three-fourths of patients with lateral leaks (in a cohort of 30 patients with type 2 leaks) can definitely be identified by DSM, presenting high-flow leaks. At our institution, further CT scans are performed in the remaining cases (CT following DSM or DCTM another day) to visualize underlying slow flow or leaks previously superimposed at DSM. This procedure is increasingly being replaced by CBCT, as illustrated here.
DCTM has been frequently reported as a diagnostic tool for type 2 leaks.6⇓–8 CT is readily available, offers a great advantage with cross-sectional imaging, and is feasible to capture the entire spine. However, temporal and spatial (0.4–0.6 mm) resolution is relatively lower compared with DSM, and the radiation dose is high (often requiring multiple scans).2,6 A recent study modified this technique to lower the radiation dose.8
CBCT is usually applied to better illustrate complex anatomic vascular structures in 3D. A flat panel detector generates conebeam data sets while the C-arm rotates around the patient, providing highest spatial resolution (up to 0.14 mm) and high contrast resolution.3 In 2013, Chu and McAuliff3 suggested using CBCT to identify the time point of dural contrast egress for high-volume lateral dural leaks in patients with SIH, because true dynamic examinations were rarely used at this time. Today, the advantage of CBCT may be more to selectively confirm or exclude questionable findings during DSM without delay so that the contrast egress can still be assigned to the actual site of leak (which may not be possible after transporting the patient to the CT scanner). Depending on institutional standards, this information could reduce or omit further CT investigations. The radiation dose of CBCT is assumed to be comparable with that of conventional CT,9 but this assumption has not been evaluated in spinal imaging of patients with SIH so far. Moreover, the high spatial resolution of CBCT may provide additional insight into underlying anatomy. In the future, targeted use of CBCT could also be helpful to detect ventral dural leaks (type 1) with the patient in the prone position by clarifying indeterminate findings during DSM.
CONCLUSIONS
In selected cases with equivocal DSM findings, simultaneous CBCT acquisition may help reveal lateral dural CSF leaks.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received February 19, 2023.
- Accepted after revision April 6, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Advanced Imaging of Type 2 Spinal CSF Leaks with Ultra-High-Resolution Conebeam CT Myelography
- Conebeam CT Myelography for the Detection of Spinal CSF Leaks
- Spinal CSF Leaks: The Neuroradiologist Transforming Care
- Lateral Spinal CSF Leaks in Patients with Spontaneous Intracranial Hypotension: Radiologic-Anatomic Study of Different Variants