
Abstract
BACKGROUND AND PURPOSE: Autoimmune encephalitis is a rare condition in which autoantibodies attack neuronal tissue, causing neuropsychiatric disturbances. This study sought to evaluate MR imaging findings associated with subtypes and categories of autoimmune encephalitis.
MATERIALS AND METHODS: Cases of autoimmune encephalitis with specific autoantibodies were identified from the medical record (2009–2019). Cases were excluded if no MR imaging of the brain was available, antibodies were associated with demyelinating disease, or >1 concurrent antibody was present. Demographics, CSF profile, antibody subtype and group (group 1 intracellular antigen or group 2 extracellular antigen), and MR imaging features at symptom onset were reviewed. Imaging and clinical features were compared across antibody groups using χ2 and Wilcoxon rank-sum tests.
RESULTS: Eighty-five cases of autoimmune encephalitis constituting 16 distinct antibodies were reviewed. The most common antibodies were anti-N-methyl-D-aspartate (n = 41), anti-glutamic acid decarboxylase (n = 7), and anti-voltage-gated potassium channel (n = 6). Eighteen of 85 (21%) were group 1; and 67/85 (79%) were group 2. The median time between MR imaging and antibody diagnosis was 14 days (interquartile range, 4–26 days). MR imaging had normal findings in 33/85 (39%), and 20/33 (61%) patients with normal MRIs had anti-N-methyl-D-aspartate receptor antibodies. Signal abnormality was most common in the limbic system (28/85, 33%); 1/68 (1.5%) had susceptibility artifacts. Brainstem and cerebellar involvement were more common in group 1, while leptomeningeal enhancement was more common in group 2.
CONCLUSIONS: Sixty-one percent of patients with autoimmune encephalitis had abnormal brain MR imaging findings at symptom onset, most commonly involving the limbic system. Susceptibility artifact is rare and makes autoimmune encephalitis less likely as a diagnosis. Brainstem and cerebellar involvement were more common in group 1, while leptomeningeal enhancement was more common in group 2.
ABBREVIATIONS:
- AIE
- autoimmune encephalitis
- anti-Gq1b
- anti-ganglioside Q1b
- anti-LGI1
- anti-leucine-rich glioma inactivated 1
- CASPR2
- contactin-associated protein-like 2
- GABA
- gamma-aminobutyric acid
- GAD
- glutamic acid decarboxylase
- GFAP
- glial fibrillary acidic protein
- NMDA
- N-methyl-D-aspartate
- PD-1
- programmed cell death protein 1
- VGCC
- voltage gated calcium channel
- VGKC
- voltage-gated potassium channel
Autoimmune encephalitis (AIE) is an increasingly recognized cause of acute or subacute altered mental status and neurologic disturbance associated with antibodies against neuronal antigens.1 Such antibodies may develop independently or in response to malignancies such as small-cell lung cancer and ovarian teratomas, which may be occult at the time of presentation.2 The clinical diagnosis of AIE can be challenging because the initial presentation can mimic other neurologic problems or primary psychiatric disorders.2,3 MR imaging of the brain plays an important role in excluding other neurologic diagnoses and in suggesting the possibility of AIE.4,5 Common MR imaging findings in AIE include limbic encephalitis, though findings may vary by antibody subtype, with some antibodies showing a predilection for the deep gray nuclei, brainstem, or cerebellum.1,6 Prior studies of AIE have also shown that more than half of all cases may have normal MR imaging findings at presentation.7
Antibodies associated with AIE have been classified into 2 groups: antibodies with intracellular neuronal antigens (group 1) and antibodies with extracellular neuronal antigens (group 2) (Table 1). AIE associated with group 1 antibodies is more often associated with an underlying malignancy, has an overall poorer prognosis, and is relatively less responsive to treatment. In contrast, AIE associated with group 2 antibodies has a better prognosis, and antibody titers more closely correlate with the severity of symptoms and response to treatment.2,8
Classification of autoantibodies in this cohort into group 1 (intracellular antigens) versus group 2 (extracellular antigens) autoimmune encephalitis
Timely diagnosis of AIE is important because earlier treatment is more likely to reverse symptoms.9 Although there are many reports in the literature detailing the imaging appearance of specific individual autoantibodies,1,8⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓-25 there are currently very few scientific articles investigating the distribution of imaging features associated with different antibodies in a large population of AIE,7,26⇓-28 allowing the development of a framework with which to evaluate this category of diseases.1 In this study, we analyzed the brain MR imaging of 85 patients from our institution diagnosed with AIE, with imaging performed around the time of diagnosis. We hypothesize there are specific MR imaging findings more commonly associated with certain antineuronal antibodies and antibody groups.
MATERIALS AND METHODS
This retrospective, single-institution, cross-sectional study was Health Insurance Portability and Accountability Act–compliant and approved by the institutional review board of our institution (University of California San Francisco). All eligible participants were identified by searching the medical record for Internal Classification of Disease (ICD9 and ICD10) codes for AIE between 2009 and 2019. Inclusion criteria were the following (Fig 1): 1) diagnosis of AIE between 2009 and 2019; 2) specific laboratory-confirmed autoantibodies from CSF and/or blood that were thought to be contributory to the patient’s neurologic abnormality, on the basis of review of clinical notes; and 3) MR imaging of the brain obtained during the immediate work-up of the laboratory-confirmed AIE diagnosis. Patients with a diagnosis of autoimmune demyelinating disease, such as anti-aquaporin-4 antibody-mediated neuromyelitis optica and anti-myelin oligodendrocyte–associated disease, were excluded from this study because these entities constitute a different class of disease.

Flowchart of patient inclusion and exclusion criteria for the study. MOG indicates myelin oligodendrocyte; NMO, neuromyelitis optica.
The medical record was searched for demographic characteristics including sex and age and clinical/laboratory data including CSF cell count, CSF protein level, the presence of underlying malignancy, pre-existing or newly diagnosed at symptom onset, and the specific laboratory-confirmed autoantibody. The medical record was evaluated for the presence of potential confounding clinical factors, such as clinical seizures at the time of MR imaging and the initiation of steroid therapy before MR imaging.
MR imaging of the brain associated with the work-up and subsequent laboratory diagnosis was independently scored by 2 blinded neuroradiologists with 5 and 7 years of experience, and discrepancies were resolved by consensus. The magnetic field strength and available sequences by MR imaging were catalogued. MR imaging findings were classified as normal or abnormal. Studies with abnormal findings were scored for the presence of structural or signal abnormality in the following predefined locations, selected on the basis of their association with AIE in prior literature: limbic, extralimbic cortex, deep gray nuclei (including hypothalamus), deep white matter, periventricular white matter, subcortical white matter, brainstem, cerebellum, and cervicomedullary junction.1,10 Additionally, studies were scored on the basis of whether they demonstrated abnormality on DWI or SWI or enhancement in the following distributions: white matter, perivenular, leptomeningeal (including cranial nerve enhancement). Expected age-appropriate imaging findings, such as age-appropriate parenchymal volume loss or nonspecific T2 FLAIR hyperintensity in the white matter within expected limits for age, were not categorized as abnormalities for this study.
Statistical Analysis
Statistical analysis was conducted using STATA, Version 16 (StataCorp).29 We examined the distribution of patient characteristics among those with group 1 and 2 antibodies using χ2 and Wilcoxon rank-sum tests. We further examined the distribution of imaging findings between group 1 and 2 antibodies using the χ2 test. A P value < .05 was defined as a statistically significant result.
RESULTS
Clinical and Demographic Findings
Of 104 patients with antibody-proved AIE between 2009 and 2019, seven were excluded due to the lack of MR imaging from the time of diagnosis, 10 were excluded for the diagnosis of autoimmune demyelinating disease (5 cases of neuromyelitis optica and 5 cases of myelin oligodendrocyte glycoprotein associated disease), and 2 were excluded for the concurrent detection of 2 autoantibodies, precluding evaluation for the causative antibody (Fig 1). Eighty-five patients diagnosed with AIE had an MR imaging of the brain performed a median of 14 days (interquartile range, 4–26 days) before the laboratory-confirmed diagnosis of AIE.
In this cohort, the median age at presentation was 36 years (interquartile range, 24–62 years, Table 2), and most patients were women (71%). Regarding the CSF cell count, 57 (67%) patients had CSF leukocytosis and 33 (39%) patients had elevated protein. There was a trend toward elevated CSF protein more frequently seen in those with group 1 antibodies compared with group 2 (61% versus 33%, P = .06). Fifteen patients (18%) had a malignancy discovered around the time of their AIE diagnosis, and 10 (12%) had nonmalignant tumors such as hamartomas and teratomas. Only 2 patients with malignancy had pre-existing malignancy known before symptom onset. The rate of malignant tumor was significantly higher in group 1 than in group 2 (33% versus 13%, P < .05, Table 2), though there was no significant difference in the rates of teratomas and hamartomas between the two groups. Thirty-five patients (41%) had clinical or electroencephalography seizures around the time of MR imaging. Nine patients (11%) had been treated with steroids, and 3 patients (4%) with IV immunoglobulin up to 1 month before imaging.
Demographic and clinical features of 85 patients with laboratory-proved autoimmune encephalitis, stratified by antibody group
Specific Autoimmune Antibodies
In 85 patients, 16 distinct types of AIE antibodies were found (Online Supplemental Data). The most common antibodies were anti-N-methyl-D-aspartate (NMDA) receptor antibodies (n = 41), anti-glutamic acid decarboxylase (GAD) antibodies (n = 7), and anti-voltage-gated potassium channel (VGKC) antibodies (n = 6). Eighteen of 85 (21%) were in group 1, and 67/85 (79%) were in group 2 antibodies.
MR Imaging Findings by AIE Group
Of the 85 brain MR images evaluated in this study, 30/85 (35%) were performed at 3T and 55/85 (65%) were performed at 1.5T. Eighty-four of 85 (99%) studies included DWI, 85/85 (100%) included T1-weighted imaging, 85/85 (100%) included T2 FLAIR imaging, 68/85 (80%) included SWI in the form of either SWI/iron sensitive imaging/gradient recalled-echo/multiplanar gradient-recalled, and 80/85 (94%) included T1-postcontrast imaging. The frequency of imaging findings by AIE group and for all specific antibody subtypes is shown in the Online Supplemental Data.
There were significant differences between group 1 and group 2 AIE with respect to the percentage with signal abnormality in the brainstem and cerebellum (Online Supplemental Data). Brainstem signal abnormality was more common in group 1 AIE, seen in anti-Hu, anti-Ma2/Ta, and anti-CV2 (Online Supplemental Data). Among group 2 AIE, brainstem signal abnormality was seen with anti-glial fibrillary acidic protein (GFAP) and anti-voltage gated calcium channel (VGCC) but was less common compared with group 1. Cerebellar signal abnormality was also significantly more common in group 1 AIE, seen in anti-Hu, anti-Yo, anti-CV2, and anti-GAD (Online Supplemental Data). Among group 2 AIE, cerebellar signal abnormality was seen in anti-NMDA, anti-GFAP, anti-VGCC, anti-programmed cell death protein 1 (PD-1), and anti-ganglioside Q1b (GQ1B), but it was less common compared with group 1.
Antibody Subtype Based on MR Imaging Findings
MR imaging findings were abnormal in 52/85 (61%) patients. The most common areas of signal abnormality in the overall cohort were limbic (28/85, 33%), extralimbic cortex (18/85, 21%), and periventricular white matter (17/85, 20%, Online Supplemental Data). Ten cases (12%) had reduced diffusion, which was not significantly more common in either group 1 or group 2 (1/18, 6% versus 9/67, 13%, P = .36). Only 1/68 (1.5%) had susceptibility artifacts, which were in a case of anti-NMDA encephalitis.
Normal MR Imaging Findings.
Thirty-three of 85 (39%) patients with AIE had normal findings on MR imaging of the brain. Patients with anti-NMDA encephalitis constituted those with the most normal MR imaging findings (20/33, 61%). Other patients with normal MR imaging had laboratory-confirmed anti-Hu, anti-Yo, anti-GAD, anti-NMDA, anti-α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAr), anti-VGCC, anti-DPPX, anti-GQ1B, anti-VGKC, anti-leucine-rich glioma inactivated 1 (LGI1) and anti-contactin-associated protein-like 2 (CASPR2).
Limbic Signal Abnormality.
Limbic signal abnormality was present in 28/85 (33%) patients and seen in anti-Hu, anti-Ma2/Ta, anti-CV2, anti-GAD, anti-NMDA, anti-gamma-aminobutyric acid (GABA)-B, anti-GFAP, anti-VGKC, and anti-CASPR2 (Online Supplemental Data).
Deep Gray Signal Abnormality.
Deep gray signal abnormality was present in 10/85 (12%) patients and seen in anti-Ma2/Ta, anti-CV2, anti-GAD, anti-NMDA, and anti-LGI1 encephalitis (Online Supplemental Data).
Deep White Matter Signal Abnormality.
Eleven of 85 (13%) patients had deep white matter signal abnormality, including those with anti-Hu, anti-CV2, anti-GAD, anti-NMDA, anti-GFAP, and anti-VGCC (Online Supplemental Data).
Subcortical White Matter Signal Abnormality.
Sixteen of 85 (19%) patients demonstrated subcortical white matter signal abnormality, including patients with anti-Hu, anti-Yo, anti-NMDA, anti-GABA-B, anti-GFAP, anti-VGCC, and anti-VGKC (Online Supplemental Data).
Periventricular White Matter Signal Abnormality.
Seventeen of 85 (20%) patients demonstrated periventricular white matter signal abnormality, including patients with anti-CV2, anti-GAD, anti-NMDA, anti-GFAP, anti-VGCC, and anti-VGKC (Online Supplemental Data).
Extralimbic Cortex.
Eighteen of 85 (21%) patients demonstrated extralimbic cortical signal abnormality, including patients with anti-CV2, anti-GAD, anti-NMDA, anti-GABA-A, anti-GFAP, anti-VGCC, anti-VGKC, anti-LGI1, and anti-CASPR2 (Online Supplemental Data).
Brainstem.
Five of 85 (6%) patients demonstrated brainstem signal abnormality, including patients with anti-Hu, anti-Ma2/Ta, anti-CV2, anti-GFAP, and anti-VGCC encephalitis (Online Supplemental Data). Brainstem signal abnormality was more commonly seen in group 1 AIE (Online Supplemental Data).
Cerebellum.
Ten of 85 (12%) patients demonstrated cerebellar signal abnormality or volume loss, including patients with anti-Hu, anti-Yo, anti-CV2, anti-GAD, anti-NMDA, anti-GFAP, anti-VGCC, anti-PD-1, and anti-GQ1B encephalitis (Online Supplemental Data). Cerebellar abnormality was more common with group 1 than group 2 AIE (Online Supplemental Data).
White Matter Enhancement.
Three of 80 (4%) patients demonstrated white matter enhancement, including patients with anti-GFAP and anti-PD-1 encephalitis (Online Supplemental Data). For anti-PD-1 encephalitis, the white matter enhancement was cerebellar in location.
Deep Gray Enhancement.
One of 80 (1%) patients demonstrated deep gray enhancement seen in a patient with anti-LGI1 encephalitis (Online Supplemental Data).
Perivenular Enhancement.
Four of 80 (5%) patients demonstrated perivenular enhancement, including patients with anti-GAD, anti-NMDA, and anti-GFAP (Online Supplemental Data).
Leptomeningeal/Cranial Nerve Enhancement.
Two of 80 (2.5%) patients demonstrated leptomeningeal enhancement, both of whom had anti-GQ1B encephalitis. One demonstrated cranial nerve enhancement, and the other demonstrated enhancement along the cerebellar folia in regions of abnormal cerebellar signal (Online Supplemental Data).
DISCUSSION
In our retrospective study of consecutive patients from our institution diagnosed with laboratory-confirmed AIE, we found MR imaging abnormalities present in approximately two-thirds of patients at the time of symptom onset, and limbic signal abnormality was the most common, seen in 33% of patients. Although there were many overlapping features among the specific autoantibody subtypes, group 1 antibodies more commonly involved the brainstem and cerebellum, while group 2 more commonly demonstrated leptomeningeal enhancement. Certain imaging findings were seen more commonly with specific antibody subtypes. Our findings support an imaging framework for suggesting AIE by imaging and potentially specific AIE subtypes based on MR imaging findings (Fig 2).26,28,30

Proposed imaging stratification algorithm for patients with suspected AIE. Boldface antibodies belong to the group 1 classification.
The results of our imaging analysis reinforce the findings of many smaller studies and case reports on specific autoantibodies.4,7,9,10,13,18,20,21,24⇓⇓-27,31 The anti-NMDA receptor antibody was the most common antibody in our cohort, similar to findings in other cohort studies.19,27,38 Only 1 patient in the cohort demonstrated susceptibility artifacts suggestive of hemorrhage, and this was in a patient with anti-NMDA receptor encephalitis, who developed AIE after herpes simplex virus encephalitis. This finding reinforces prior studies and case reports on AIE, which have not described susceptibility artifacts as an imaging feature of AIE; thus, the presence of susceptibility typically makes AIE a less likely diagnosis.16,32
In our study, 39% of patients had normal MR imaging findings despite antibody-proved AIE. Normal MR imaging findings were seen in several AIE subtypes, most commonly anti-NMDA encephalitis. Prior studies have demonstrated that a subset of patients with AIE will have normal MR imaging findings despite clinically-apparent neuropsychiatric disturbances.2 In 1 prior study, 40% of patients with NMDA receptor encephalitis had normal MR imaging findings, similar to the results in our study.19 A separate study analyzing 77 patients with a diverse subset of antibodies found that 63% of patients presented with normal or nonspecific MR imaging findings at symptom onset.7 Notably, brain MR imaging findings may initially be normal, and MR imaging changes can develop subsequently, thus demonstrating the importance of follow-up imaging in patients with a suspected diagnosis of AIE.5 Additional imaging modalities such as PET/CT and additional imaging sequences such as arterial spin-labeling perfusion may be helpful adjuncts in the work-up of those patients with AIE and otherwise normal MR imaging findings.33⇓-35 Most important, normal MR imaging findings do not exclude AIE as a diagnosis in the context of appropriate clinical suspicion, and appropriate laboratory work-up should ensue.
On a group level, our study found a higher percentage of brainstem and cerebellar involvement in group 1 AIE. Although the evaluation of individual subtypes of AIE was challenging due to the small number of patients with some subtypes, a few general trends could be appreciated. Multiple subtypes demonstrated limbic involvement, some of which, including anti-Ma2/Ta, anti-GAD, and anti-Hu also involved the brainstem or cerebellum. Anti-CV2 (Fig 3) and anti-LGI1 involved the limbic system, extralimbic cortex, and deep gray nuclei. Some cases of anti-NMDA involved all of the following: limbic, extralimbic cortex, deep gray nuclei, and brainstem/cerebellum (Fig 4). Multiple prior case reports and smaller studies support the conclusions of our study that these subtypes cause limbic encephalitis, often with additional involvement.2,6,9,12,23,26,36

Imaging findings in examples of group 1 antibody AIE. A, A 65-year-old woman with a history of ovarian cancer who developed emesis, ataxia, and gait instability. Axial FLAIR images demonstrate enlarged cerebellar folia (large white arrow), compatible with volume loss. Subsequent work-up revealed anti-Yo encephalitis. B, A 44-year-old woman with 9 months of progressive ophthalmoplegia, amnesia, mild hemiparesis, and vertigo. Axial FLAIR imaging demonstrates deep gray and periventricular white matter hyperintensity (white arrows). The patient was subsequently diagnosed with anti-CV2 encephalitis.

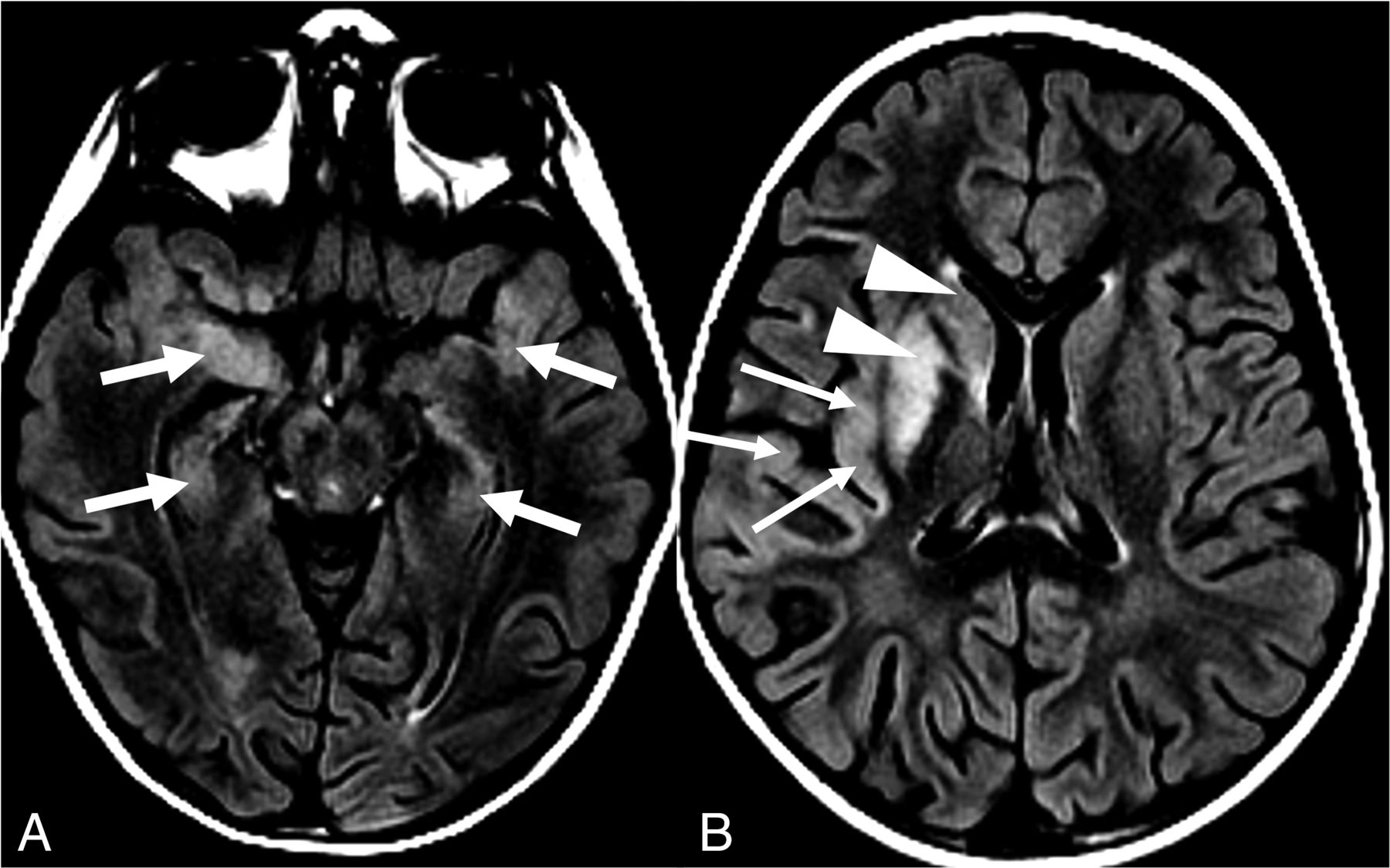
A 22-year-old man with no major medical history presented with subacute, progressive, altered mental status and psychiatric symptoms including paranoia and visual and auditory hallucinations. He subsequently developed memory loss and aphasia and was ultimately diagnosed with anti-NMDA receptor encephalitis. Axial FLAIR images of the patient at 2 different levels are shown. A, At the level of the temporal horns, there is FLAIR hyperintensity and swelling of bilateral hippocampi and medial temporal lobes (white arrows). B, At the level of the lateral ventricular bodies, there is FLAIR hyperintensity and swelling of the right insular and superior temporal cortices (thin white arrows), as well as the right caudate head and putamen (white arrowhead).
Patients with anti-Yo antibody–associated AIE in our cohort had cerebellar signal abnormality and volume loss (Fig 3), which has been described in prior articles describing anti-Yo antibodies as a cause of paraneoplastic cerebellar degeneration.21,24 Previous reports of anti-Ma2/Ta describe brain abnormalities with T2 hyperintensities primarily in the mesial temporal lobes with occasional involvement of the brainstem and thalami.13,37
Patients in our cohort with anti-GFAP astrocytopathy demonstrated periventricular and deep white matter signal abnormality, with perivenular enhancement in the deep white matter (Fig 5), consistent with previous review articles and case reports.4,11,25 Patients with anti-GQ1b antibody–associated AIE (Fig 6) were the only ones in our cohort to demonstrate leptomeningeal and cranial nerve enhancement, consistent with previous descriptions in the literature.20 Because anti-GQ1b is thought to cause Miller Fisher syndrome, a variant of Guillain-Barre syndrome affecting cranial nerves, this imaging feature corresponds to clinical symptoms.15 In a study analyzing 15 patients with anti-GQ1b antibodies, 14 of 16 MR imaging examinations demonstrated at least 1 cranial nerve abnormality.20

A 43-year-old woman with progressive, altered mental status and right-leg and buttock paresthesia. Subsequent testing revealed anti-GFAP encephalitis. Axial (A) and sagittal (B) postcontrast T1-weighted imaging demonstrates linear perivenular enhancement (white arrows) radiating into the periventricular white matter.

A 20-year-old man with a several-day history of headache and new-onset diplopia with a subsequent work-up revealing anti-GQ1b encephalitis. Axial (A) and coronal (B) postcontrast T1-weighted imaging demonstrates leptomeningeal enhancement of the right cerebellar hemisphere (white arrows).
In keeping with prior studies,26,28,30 most patients with AIE in our study were women (71%) and young (median age, 36 years). There was a significantly higher rate of associated malignancy with group 1 antibodies, in line with the findings in prior literature.2,38 Patients with group 1 antibodies demonstrated elevated CSF protein compared with group 2. A prior study investigating CSF findings in AIE found similar results, with 53% of patients with group 1 antibodies demonstrating elevated CSF protein versus 37% of those with group 2 antibodies.39 The predominant theory for this phenomenon is that CSF protein generally increases with age, and because patients with group 1 antibodies typically are older, the increased incidence of elevated CSF protein could be correlated to increased age.30,39
To our knowledge, this study represents the largest scientific imaging evaluation of a consecutive cohort of patients with laboratory-proved AIE. While prior literature has been published on individual AIE subtypes, few articles have studied AIE as a whole and provided a framework for approaching the diagnosis by imaging. However, our study does have several limitations. While we studied many cases of AIE in aggregate, there were few individual cases of rare antibody subtypes. Our study lacked an age-matched control group, but age-related changes were intentionally not scored in our imaging review. Because the cohort dates back to 2008, many older MR images were obtained with 2D sequences at 1.5T; however, these studies are of diagnostic quality and remain consistent with image quality in current clinical practice. Not all patients had SWI or postcontrast imaging performed around the time of diagnosis, limiting the detection of abnormalities on those sequences. Additionally, approximately 15% of patients had received prophylactic steroid or IV immunoglobulin therapy before imaging, which may decrease the severity of the findings seen on MR imaging. Because 41% of patients in this study had seizures around the time of imaging, it is possible that some imaging findings may represent the manifestation of concurrent seizures, particularly cortical- and deep gray–reduced diffusion; however, no patients had imaging abnormalities confined only to these regions; thus, we believe that most abnormalities are attributable to the underlying AIE in these cases. Finally, because we studied only the initial MR images obtained around the time of symptom onset and not subsequent follow-up imaging, we did not study the evolution of these imaging findings and whether patients with initial normal MR imaging findings subsequently developed abnormalities. Future longitudinal, multicenter studies are needed to increase the follow-up time and sample size to generate more specific conclusions in this population.
CONCLUSIONS
In this single-institution study of 85 consecutive patients with the confirmed diagnosis of AIE, approximately two-thirds had abnormal findings on brain MR imaging, with limbic signal abnormality the most common abnormal imaging finding. Susceptibility artifacts are rarely seen in AIE (only noted in 1 patient in our study); thus, their presence makes AIE less likely. While we documented certain imaging features to be more frequent in certain subtypes of AIE, in many cases, imaging findings at symptom onset were normal but were still useful to rule out alternative causes of the patient’s neurologic presentation. Early identification of neuroimaging features of AIE will lead to earlier diagnosis, treatment, and potentially improved clinical outcomes.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received July 24, 2022.
- Accepted after revision May 24, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.