
Abstract
BACKGROUND AND PURPOSE: Endovascular treatment of wide-neck bifurcation aneurysms has historically proved difficult with variable outcomes. Different endovascular techniques such as balloon-assisted coiling, stent-assisted coiling, or intrasaccular devices provide a varied range of efficacy and safety. Neqstent-assisted coiling is a new device and technique that aim to provide a maximum of both. We analyzed the early clinical and radiologic outcomes after the use of this new technique and device in our practice.
MATERIALS AND METHODS: This study was a retrospective analysis of ruptured and unruptured intracranial aneurysms treated with the Neqstent. The primary radiologic outcomes were quantified on DSA, CTA, or MRA using the modified Raymond-Roy criteria. The outcomes were defined as immediate complete occlusion (modified Raymond-Roy criteria 1) and complete (modified Raymond-Roy criteria 1) and adequate occlusion (modified Raymond-Roy criteria 1 and modified Raymond-Roy criteria 2) at 6 months posttreatment. The primary safety outcome was the rate of device-related adverse events. Secondary safety outcomes included time to discharge and change in the mRS score at 6-month follow-up.
RESULTS: Twenty patients were treated with the Neqstent from November 2020 to January 2023. Nine had unruptured aneurysms, and 11 were patients with subarachnoid haemorrhage due to ruptured aneurysms. Eighteen of 20 aneurysms (90%) treated demonstrated complete occlusion (modified Raymond-Roy criteria 1) on immediate postembolization angiograms. Sixteen of 17 aneurysms treated (94.1%) remained adequately occluded on 6-month follow-up (modified Raymond-Roy criteria 1 and modified Raymond-Roy criteria 2). Immediate postoperative complications occurred in 2 patients; only 1 patient had residual neurologic deficits at 6 months (mRS = 2).
CONCLUSIONS: Management of large, wide-neck aneurysms remains difficult, with high rates of recurrence and complications. The use of the Neqstent shows promising short-term results for the treatment of complex wide-neck aneurysms. Initial complication rates for our cohort were relatively high. However, this result is likely related to the initial learning experience of device deployment and the use of antiplatelets.
ABBREVIATIONS:
- mRRC
- modified Raymond-Roy criteria
- WNBA
- wide-neck bifurcation aneurysms
Since the International Subarachnoid Aneurysm Trial (ISAT) in 2002, coil embolization remains a safe and well-established technique for the treatment of ruptured and unruptured intracranial aneurysms.1 Aneurysm recurrence following endovascular therapy has been an associated unfavorable outcome since its emergence. Although posttreatment rebleed risk remains low, the anxiety for patients remains an issue.2
Wide-neck bifurcation aneurysms (WNBAs) are defined as bifurcation intracranial aneurysms with an absolute neck diameter of 4.0 mm or a dome-to-neck ratio of <2.0.3 The incidence of aneurysm recurrence is a particular issue relating to complex wide-neck aneurysms. Subsequently, technologic advancements for endovascular treatment of ruptured and at-risk incidentally diagnosed aneurysms have rapidly expanded.4
Our study analyzed the use of the Neqstent (Stryker), a novel intrasaccular device designed to aid in the treatment of complex wide-neck bifurcation aneurysms. The aim of this study was to evaluate the efficacy and safety of a large single-center experience using the Neqstent. To the best of our knowledge, this is the largest real-life single-center experience published using this novel device.
MATERIALS AND METHODS
Study Design
The study is a retrospective, single-arm study. The patient eligibility criteria included patients with acute SAH with acutely ruptured intracranial aneurysms and elective patients with incidental intracranial aneurysms. The aneurysm treatment criterion was defined as bifurcation aneurysms with a neck of at least 4 mm or a dome-to-neck ratio of <2. Patients were selected by the principal operators (T.P. and N.S.) without sponsor interference.
The primary efficacy end point was the successful occlusion of the aneurysm measured by the modified Raymond-Roy Classification (mRRC) at 6 months, proved by MRA, CTA, or DSA. Secondary efficacy outcomes included immediate postoperative angiographic occlusion rates and retreatment of aneurysm recurrences.
The primary safety end point was the rate of adverse events (any postprocedural neurologic deficit and a measure of the mRS score at 6 months). Secondary safety outcomes included time to patient discharge and the patient’s functional outcome at that point.
Neqstent
The Neqstent is an adjunctive intrasaccular flow-diverter device that has been developed specifically for the treatment of complex wide-neck bifurcation aneurysms. It is a nitinol microbraided mesh with dual construction, containing a platinum core wire for visualization. It is compatible with 0.021- and 0.027-inch microcatheters, with sizes of 7, 9, 11, and 14 mm. The design allows a microcatheter to advance through the mesh for aneurysm dome coiling. The sizing of the device is dependent on the neck width as demonstrated in Table 1.
Sizing guide for Neqstent
The similarity of the Neqstent to the Contour Neurovasvular System (Stryker) is in the dual-mesh construction. The benefit of the Neqstent is that it contains 44% of the total number of wires (64 wires) in its construction compared with the Contour, which has 144 wires. The wire diameter is larger in the Neqstent; therefore, the actual surface area coverage of the device is 67% of what the Contour provides. This difference has the ability to pass a microcatheter through the construct for dome coiling while providing a similar level of neck protection and reconstruction in addition to flow diversion like the Contour. An example of Neqstent flow diversion with subsequent appearances post-coil deployment is demonstrated in the Online Supplemental Data.
Procedural Data
All procedures were performed with the patients under general anesthesia in biplane angiography suites. A common femoral approach was used under sonographic guidance. This series did not prepare all patients with antiplatelets before the procedure. All patients received heparin intravenously after successful common femoral puncture with the aim of achieving an activated clotting time of 1.5–2 times the baseline. The use of triaxial or biaxial systems was decided before the procedure to ensure stable navigation and deployment of the microcatheters required and the Neqstent. This choice was dependent on the patient’s vascular anatomy and the location of the aneurysm. On navigation into the target vessel, initial biplane and 3D rotational angiograms were obtained for planning and aneurysm measurement.
A 0.021-inch Headway (MicroVention) microcatheter for 7-, 9-, and 11-mm Neqstent devices and a 0.027-inch Headway microcatheter for the 14-mm Neqstent were required for navigation and deployment. A check angiogram would be performed on device deployment before detachment to ensure good aneurysm neck apposition. A 0.017-inch microcatheter (Echelon 10; Medtronic, or Headway 17) was adjunctively used for coil deployment into the aneurysm dome. In our cohort, we would always begin by jailing the microcatheter adjacent to the Neqstent. In cases of incomplete neck coiling of larger aneurysms, we would re-enter through the Neqstent using an 0.014-inch microwire and any 0.017-inch microcatheter such as the Headway or Echelon. The aim would be to coil the aneurysm to complete occlusion. Finally, angiography was performed to assess aneurysm occlusion.
Two patients received a bolus dose of IV Integrilin (eptifibatide) and aspirin intraoperatively. Another 9 patients received IV aspirin intraoperatively. One patient was on warfarin before the procedure, which was continued immediately postoperatively with no other antiplatelet medications. Seven patients received short-term single-antiplatelet therapy (aspirin) for 3–6 weeks post treatment.
Aneurysm Occlusion
Immediate and 6-month posttreatment angiographic appearances were classified using the mRRC.5
RESULTS
A single regional interventional neuroradiology center enrolled patients from November 2020 to January 2023. Twenty patients with eligible aneurysms were treated with the Neqstent during the 27-month period.
The mean age of the population was 63 years (range, 44–78 years; 10 men, 10 women). Eleven patients presented with acute SAH due to aneurysm rupture. Nine patients had incidentally detected unruptured intracranial aneurysms for elective treatment. None of the aneurysms were previously treated.
The average aneurysm neck size was 5.6 mm (range, 2.89–10.8 mm). The average dome-to-neck ratio was 1.84 (range, 1.11–2.83). The aneurysm locations included 1 posterior communicating artery aneurysm, 2 ICA termination aneurysms, 6 anterior communicating artery aneurysms, and 5 basilar tip, and 6 MCA bifurcation aneurysms. Four basilar tip, 4 anterior communicating artery, 1 posterior communicating artery, and 2 MCA aneurysms were treated for rupture and consequent SAH. No patients have presented with postoperative bleeding from incidental aneurysms or rebleeding from ruptured aneurysms.
The Neqstent device size was chosen according to the aneurysm neck sizes. Four 7-mm devices, five 9-mm devices, five 11-mm devices, and six 14-mm devices were used. Coils were deployed in 17 patients. A single patient’s aneurysm thrombosed on device deployment without requiring any coils. All Neqstent devices were detached on completion of aneurysm dome coiling.
Balloon assistance was required in 1 case to prevent device protrusion. The Neqstent was protruding slightly into an M2 branch after device detachment but with no thrombus formation. A balloon was navigated into the branch and slightly inflated to push the edge of the device back into the aneurysm. This process resulted in no immediate angiographic complications. The patient awoke with no neurologic deficit.
Primary and Secondary Efficacy Outcomes
Table 2 demonstrates a summary of aneurysm characteristics and treatment efficacy. The Online Supplemental Data provide a breakdown of the clinical outcomes of the patient population. Eighteen aneurysms (90%) demonstrated complete occlusion (mRRC = 1) immediately postembolization. One aneurysm demonstrated contrast opacification within the coil interstices (mRRC = 3a), while another showed a small filling neck remnant (mRRC = 2).
Baseline aneurysm characteristics and occlusion outcomes
Seventeen patients underwent 6-month radiologic follow-up (MRA = 15, CTA = 1, DSA = 1). Fifteen of 17 aneurysms (88.2%) demonstrated complete occlusion, and 16 aneurysms (94.1%) demonstrated adequate occlusion (mRRC = 1 and 2). Three patients did not undergo 6-month follow-up, 2 of whom due to ongoing rehabilitation from their initial SAH and subsequent neurologic insult. The remaining patient died from the initial SAH, which was not related to the treatment.
The only individual with an undertreated residual aneurysm in our series was patient 5, with a large very wide-neck aneurysm treated with a 14-mm Neqstent. The aneurysm dimensions were 12 × 10.8 × 18.6 mm (width × neck× height). An initial attempt was made with the Neqstent to avoid placing a stent for such a wide-neck aneurysm. The 14-mm device occupied and protected most of the aneurysm neck; however, there was a small, uncovered component of the neck “dog ear.” The majority of the aneurysm was occluded with coils, but the decision was made to abandon the procedure at that point. Follow-up DSA showed interval growth in the neck residue, which was subsequently treated with further coiling and flow diversion with a Silk Vista Baby (Balt). Further follow-up DSA showed a decrease in size of the neck residue.
One patient underwent further treatment with a flow diverter. Patient 12, with a maximum dome diameter of 17 mm and a neck at 6 mm, had a small residual neck (mRRC = 2) on the immediate postembolization angiogram at the coil and device interface. The patient presented 6 weeks later with worsening headaches. MR imaging revealed worsening perilesional edema; however, the MR angiogram and subsequent DSA demonstrated a stable residual neck (mRRC = 2). A decision was made to treat with flow diversion, and a 6-month follow-up MRA demonstrated a stable residual neck, with pronounced reduction of the perilesional edema.
Primary and Secondary Safety Outcomes
Two of 20 patients developed focal neurologic deficits in the immediate postoperative period. One patient’s symptoms resolved on discharge. A single patient had a persistent neurologic deficit at 6-month follow-up (patient 1, mRS = 2). The remaining patients did not have a change in the pretreatment mRS after treatment with the Neqstent at 6-month follow-up.
The overall average time to discharge was 13.5 days. The average time to discharge of patients with acute SAH was 23.8 days, while the average time to discharge for elective patients was 2 days (range, 1–5 days).
The patient with complete recovery had a ruptured anterior communicating artery aneurysm (patient 3), with nonocclusive thrombus of left A2 origin post device deployment. The patient was administered 500 mg of aspirin IV. The clot remained stable. The patient awoke postoperatively with some right-sided weakness, and a postoperative CT demonstrated mild perirolandic ischemia. The patient continued on aspirin, 75 mg once a day, for 6 weeks and made a complete recovery, with no neurologic deficits.
The patient with persistent neurologic deficits was our first patient treated with the Neqstent (patient 1). This was an elective right MCA bifurcation aneurysm with a 4-mm neck. The device chosen was an 11-mm Neqstent. The patient initially presented with a stroke and was found to have a premorbid proximal stenosis involving the distal M1 segment. During the procedure, the device in combination with the microcatheter in situ through the stenosis likely caused compromise of the upper M2 branch. Subsequently, a small-volume thrombus was noted involving the upper M2 branch origin on the immediate postdeployment angiogram. An IV bolus of Integrilin and 500 mg of aspirin were administered, which cleared a significant volume of clot, with minor residual clot but no flow restriction. The patient developed a left-sided hemiparesis postoperatively. A postoperative CT demonstrated a left MCA infarct. The patient made a partial recovery and was mobilizing independently with a stick at 6-month follow-up (mRS = 2).
DISCUSSION
Wide-neck aneurysms are often technically challenging to treat due to the difficulty in stabilizing the coils inside the aneurysm. The difficulty is increased in wide-neck bifurcation aneurysms because branches often arise from the aneurysm neck. This scenario leads the operator to compromise on neck coverage with endovascular treatment, which can lead to high recurrence rates of wide-neck bifurcation aneurysms.6
A 2016 meta-analysis of endovascular coiling of wide-neck aneurysms, including bifurcation aneurysms, demonstrated long-term near-complete occlusion rates of 70%–75%, with recanalization rates of up to 10%.7
Several other endovascular techniques have been developed in the past 20 years, such as stent-assisted coiling and flow-diverter stents. A recent multicenter North American trial in 2020 of the use of stents in wide-neck anterior circulation aneurysms showed 84.7% complete aneurysm occlusion.8 However, the stroke risk and morbidity relating to stent-assisted coiling and flow-diverter stents are higher than in standard coiling and can be as high as 5%–8%.9 Additionally, the thromboembolic risk limits the use of these techniques in ruptured intracranial aneurysms, due to the requirement of dual-antiplatelet treatment and the subsequent difficult balance of thromboembolic stroke versus worsening hemorrhage due to the primary bleed or possible neurosurgical instrumentation.
Subsequently, the concept of intrasaccular devices has come about, with the aim of creating a barrier at the level of the neck but no implant into the parent artery, therefore reducing the thromboembolic risk and the need for long-term dual antiplatelets. Such pure intrasaccular devices include the Woven EndoBridge (WEB; MicroVention) and the Contour Neurovascular System. The WEB and Contour retrospective and prospective studies have demonstrated good long-term outcomes and relatively low morbidity, with long-term complete occlusion rates of 54% and 73%, respectively, with both showing adequate occlusion rates of up to 85%.10,11 The concept of aneurysm neck reconstruction has been targeted through devices such as the pCONus (phenox) and the PulseRider (Pulsar Vascular). These devices are deployed in the parent vessel to cover the aneurysm neck, which differs from the Neqstent, which is deployed in the aneurysm. The pCONus and PulseRider have demonstrated 60% and 64.2% short-term complete occlusion rates, respectively.12,13
Our study looked at the short-term efficacy and safety outcomes with the use of the novel Neqstent device. A recent publication by Diana et al14 reviewed outcomes of adjunctive coil treatment with the Neqstent and Contour, with some cases of 6-month follow-up. The recent Coil-Assisted Flow Diversion Safety and Performance (CAFI) trial published results of 6 centers in Europe, which demonstrated a complete occlusion rate of 80% at 6-month follow-up, with a device-related morbidity rate of 10.5%. Our study is the largest single-center series to date with 6-month follow-up.15
Our early experience shows good outcomes relative to the recently published Woven EndoBridge Intrasaccular Therapy (WEB-IT) and Contour trials, with a complete occlusion rate of 88.2% and adequate occlusion of 94.1%. Only 1 patient had long-term treatment-related morbidity at 6 months. There is a notable chronologic decline of complications with increased technical experience and a better perioperative antiplatelet regimen. An example of successful embolization of a complex wide-neck bifurcation aneurysm is demonstrated in Fig 1.

Sample case of the treatment of a ruptured basilar tip aneurysm. A, Selective angiography demonstrates a 5-mm wide neck and 9-mm maximum dome width. B, Deployed 11-mm Neqstent device with a jailed adjacent microcatheter and deployment of the first coil. C, Final angiographic result after detachment of the Neqstent device and complete aneurysm dome coiling. Reduced flow of the right P1 segment. D, Right posterior cerebral artery flow uptake by a large-caliber posterior communicating artery.
Our experience shows that as with any pure intrasaccular device, accurate sizing is essential. The sizing of the device is simple and based purely on aneurysm neck width as demonstrated in Table 1. There are circumstances in which we would consider upsizing or downsizing. In cases of shallow wide-neck aneurysms, the operator would consider a smaller Neqstent, if suitable, to ensure opening of the device. In cases of an irregularly shaped aneurysm with multiple lobules close to the aneurysm neck, the operator might decide to increase the size to ensure inclusion of the all the aneurysm neck components in the treatment.
The navigation and deployment of the device is similar to that in Contour and, in our experience, is easier than the WEB in large, complex aneurysms.
The WEB device sizing can be challenging, particularly in complex irregular aneurysms.16 The VIA catheter (MicroVention) used for navigation and deployment of WEB devices is stiffer and more difficult to navigate through tortuous anatomy. In cases of treatment of larger aneurysms, distal aneurysms, or through tortuous anatomy, we have found that navigating a smaller-profile Neqstent through a standard 0.021- or 0.027-inch microcatheter in addition to an 0.017-inch microcatheter for adjunctive coiling is easier than navigating a stiffer VIA catheter for WEB deployment. In cases of difficult anatomy or smaller vessels that would not allow 2 adjacent microcatheters, the Neqstent can be deployed and detached with a standard 0.021- or 0.027-inch microcatheter according to the size, removing the delivery system once deployed, then navigating a coiling microcatheter through the Neqstent to complete the coiling. Additionally, the WEB requires a larger shelf inventory for treatment of different-sized aneurysms, while the Neqstent offers easier sizing and can treat aneurysms with neck diameters up to 10 mm, with a requirement of only 4 different device sizes. Hence, the Neqstent allows coiling larger aneurysms as long as the neck is ≤10 mm and the device can be well-apposed to the wall of the neck. If the device is not well-apposed or undersized, the aneurysm will invariably recur as seen in patient 1.
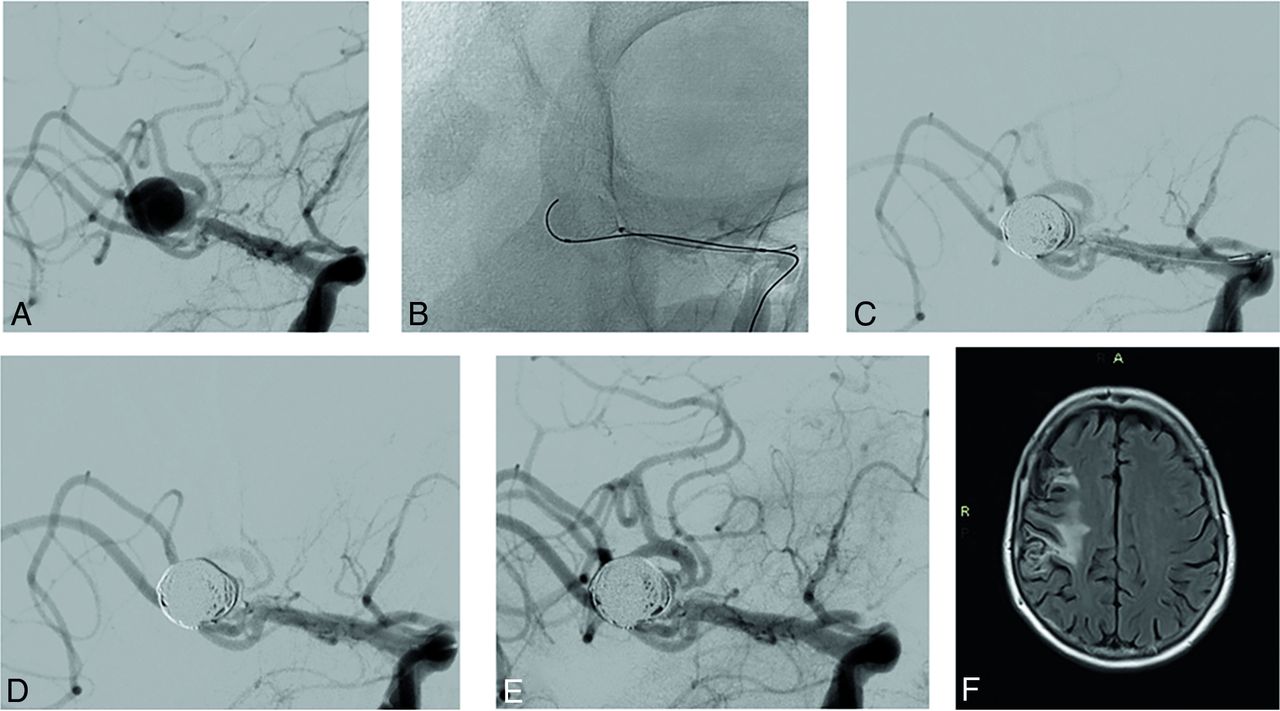
Accurate 3D sizing of the aneurysm neck is particularly important because oversized devices might risk compromise of adjacent vessels in wide-neck bifurcation aneurysms, particularly if the vessels arise from the aneurysm neck. Such a difficulty was observed in our first regional case of an MCA bifurcation aneurysm, in which there was slight compromise on an M2 branch with subsequent small clot formation as can be seen in Fig 2. Retrospectively, it was probably not the best case because there was proximal stenosis that would compromise the flow to the M2 branches. On the other hand, it shows the possibility of treating these complex aneurysms with proximal underlying stenosis safely with the Neqstent devices. After deployment, the operator withdrew the catheter proximal to the detachment marker and navigated the coiling catheter into the aneurysm. Therefore, at any 1 stage, only 1 catheter was across the stenosis. This scenario allowed treating the aneurysm but certainly led to compromise of the flow, but was managed with antiplatelets.

Sample case of a treated right MCA aneurysm. A, Working-projection angiogram with a superior M2 branch arising from the aneurysm neck. B, An 11-mm Neqstent device deployed with an adjacent jailed microcatheter and initial deployment of the first coil. C, Final angiographic result after detachment of the final coil and the Neqstent device. D, Compromise of the superior M2 branch due to device encroachment, with thrombus formation and reduced flow. E, Administration of IV aspirin and Integrilin, which reduced the clot volume and improved flow through the M2 branch. This result remained stable on 20- and 30-minute check angiograms. F, A 6-month follow-up FLAIR sequence demonstrates a sizable right-MCA cortical infarct.
Despite the minimal device contact with the parent artery, the small flow-diverting component of the braided device increases the thromboembolic risk. The risk of adverse events relating to the technique and device in our study was in 2 of 20 patients (10%). This number is lower than the authors’ review of WEB-related adverse events at 15.6%.17 Our current population size is small, with early operator experience and an improving learning curve.
The thromboembolic risk can be tackled with intraoperative IV antiplatelet therapy if early angiographic thromboembolism is identified, or another option would be to load patients suspected of warranting treatment with the Neqstent with a short course of antiplatelets before the procedure. During our initial and early experience, we had not yet made the decision to routinely preload with an antiplatelet regimen. We currently do not give antiplatelets routinely. The decision to give prophylactic antiplatelets is based on device location across the aneurysm neck and whether there is any compromise of the parent or bifurcation vessels. The exact regimen is also heterogeneous and subjective, ranging from a single IV dose of aspirin to a possible short term (4–8 weeks) of single antiplatelets. The authors have extensive experience in intrasaccular devices including the WEB and Contour and recommend, if possible, giving perioperative antiplatelets. The Neqstent offers an advantage of avoiding preoperative antiplatelets because the device appears certainly less thrombogenic than the Contour or WEB in WNBAs. Additionally, the small thromboembolic risk can be offset by a short-term postoperative course of single or dual antiplatelets. Studies of the antiplatelets have shown them to be relatively safe in patients with SAH, as was demonstrated in both our elective and acute series populations.18
The presence of coils for dome protection offers favorable immediate occlusion of the treated aneurysms, as demonstrated by the immediate occlusion rate of 90% in our study. This situation compares more favorably with other intrasaccular devices such as the Contour,19 which can be more attractive to operators who prefer coiling aneurysms. Although markedly similar to the Contour device, the adjunctive nature of the Neqstent with the use of coils to occlude the aneurysm dome offers immediate protection, hence the ability to use it in acutely ruptured intracranial aneurysms, while some operators may still have reservations about using the Contour for treatment of acutely ruptured aneurysms.
The Neqstent offers the best of both worlds. The easy-to-size device is used in conjunction with coils, which provide the ability to use the Neqstent for treatment of both ruptured and unruptured aneurysms. The flow-diverting property of the device reduces the risk of coil compaction and aneurysm recurrence. In the event of recurrence, the construct of the Neqstent allows re-entry for further coil deployment, offering easier re-treatment options than standard flow diverters or traditional pure intrasaccular devices.
Limitations
There are several limitations to this study. This was a retrospective, single-arm, single-center study for carefully selected WNBA aneurysms based on the suitability of the aneurysm location and morphology. Despite our center being a large-volume one treating approximately 300 aneurysms per year, the cohort size is relatively small, due to the initial learning experience required for this technique and careful aneurysm selection. However, with increased experience, our cohort of Neqstent-treated aneurysms has nearly doubled. The current cohort has a short-term follow-up of only 6 months. The next interval follow-up for our patients will be in 2 years from treatment, which will be published.
CONCLUSIONS
The novel technique of Neqstent-assisted coiling shows promising early results in the treatment of complex wide-neck bifurcation intracranial aneurysms. Our results show favorable occlusion rates compared with other studies relating to stent-assisted coiling and flow diversion, with less morbidity and the ability to use them in ruptured intracranial aneurysms. It also shows favorable outcomes compared with recent studies involving intrasaccular devices such as the WEB and Contour.
Perioperative antiplatelets could be beneficial and warrant further research.
Future larger studies into the Neqstent with longer follow-up data as well as comparative clinical trials could be considered to identify the best treatments for wide-neck and wide-neck bifurcation aneurysms.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received October 26, 2023.
- Accepted after revision January 11, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.