
Abstract
BACKGROUND AND PURPOSE: Few studies assess nonstenotic carotid plaques on CTA, and the causative role of these plaques in stroke is not entirely clear. We used CTA to determine the prevalence of nonstenotic carotid plaques (<50%), plaque features, and their association with ipsilateral strokes in patients with cardioembolic and cryptogenic strokes.
MATERIALS AND METHODS: Data were from the Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke (STRATIS) registry, a prospective, nonrandomized registry of patients undergoing thrombectomy with the Solitaire device. The prevalence of nonstenotic carotid plaques ipsilateral and contralateral to the stroke was compared in patients with cryptogenic and cardioembolic strokes. Plaque features were further compared within both subgroups between patients with and without ipsilateral stroke. Adjusted associations among nonstenotic carotid plaque, plaque characteristics, and ipsilateral stroke in both subgroups were determined with logistic regression.
RESULTS: Of the 946 patients in the data base, 226 patients with cardioembolic stroke (median age, 72 years) and 141 patients with cryptogenic stroke (median age, 69 years) were included in the analysis. The prevalence of nonstenotic carotid plaque in the cardioembolic and cryptogenic subgroups was 33/226 (14.6%) and 32/141 (22.7%), respectively. Bilateral nonstenotic carotid plaques were seen in 10/226 (4.4%) patients with cardioembolic and 13/141 (9.2%) with cryptogenic strokes. Nonstenotic carotid plaques were significantly associated with ipsilateral strokes in the cardioembolic stroke (adjusted OR = 1.91; 95% CI, 1.15–3.18) and the cryptogenic stroke (adjusted OR = 1.69; 95% CI, 1.05–2.73) groups. Plaque irregularity, hypodensity, and per-millimeter increase in plaque thickness were significantly associated with ipsilateral stroke in the cryptogenic subgroup.
CONCLUSIONS: Nonstenotic carotid plaques were significantly associated with ipsilateral stroke in cardioembolic and cryptogenic stroke groups, and there was an association of plaque irregularity and hypodense plaque with ipsilateral stroke in the cryptogenic group, suggesting these plaques could be a potential cause of stroke in these patient subgroups.
ABBREVIATIONS:
- aOR
- adjusted OR
- ESUS
- embolic stroke of undetermined source
- IQR
- interquartile range
- SyNC
- symptomatic nonstenotic carotid plaques
Secondary prevention of ischemic stroke relies on accurate determination of underlying stroke etiology. According to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria, which is the most commonly used classification system,1 large-artery disease is considered to be the stroke etiology in patients with carotid stenosis of >50%. The cutoff for TOAST–large artery disease was an arbitrary one, and later on, the 50% cutoff emerged from the NASCET trial, in which the maximal benefit of carotid endarterectomy was seen among patients with >50% carotid stenosis based on DSA measurements.2,3 Other common stroke etiologies according to TOAST are cardioembolic stroke and stroke with an undetermined source. However, the “undetermined source” category has some error because it includes patients with no source as well multiple sources. For this very reason, the term “embolic stoke of undetermined source” (ESUS) was coined in 2014, and it includes patients with “no source” only. ESUS accounts for up to one-third of ischemic strokes, and recent studies have shown that ESUS embodies various causes like a patent foramen ovale and atrial cardiomyopathy, in addition to nonstenotic carotid plaques.4
In a recent meta-analysis, the risk of recurrent stroke/TIA in patients with nonstenotic carotid plaques was 2.6/100 person-years and increased to 4.9/100 person-years if intraplaque hemorrhage was present.5 Furthermore, even in cardioembolic strokes, it has been shown that nonstenotic carotid disease (<50%) as a competing source of stroke is present in 9%–12%. Acknowledging these plaques as a competing cause of stroke may lead to reclassification of diagnoses in up to 22% of patients with cardioembolic stroke.6 Thus, it may be incorrect to conclude that the presence of a cardiac source, such as atrial fibrillation, is sufficient to establish stroke causality. In addition, the NAVIGATE ESUS trial, which evaluated the efficacy of oral anticoagulation with rivaroxaban in patients with ESUS compared with aspirin, failed to show any benefit with rivaroxaban. The trialists attributed this outcome to the high enrollment of patients with nonstenotic carotid disease, in whom antiplatelets may be more effective than anticoagulation.7
Recently, a classification suggested stratification of these nonstenotic carotid plaques on the basis of clinical and imaging features into possible, probable, and definite sources of stroke (symptomatic nonstenotic carotid plaques [SyNC]).8 This classification defines definite SyNC as patients with nonstenotic plaque with changing morphology on at least 2 different examinations with imaging findings consistent with stroke in the corresponding ICA territory in the absence of another cause. Probable SyNC was further stratified into the presence or absence of a cardiac cause with more strict criteria in presence of a competing cardiac cause.
We hypothesized that nonstenotic carotid plaques are a possible underlying stroke etiology in patients with cryptogenic and cardioembolic stroke, and we investigated the association of nonstenotic carotid plaques on CTA with ipsilateral strokes in patients with cryptogenic and cardioembolic stroke and aimed to identify plaque features that are independently associated with ipsilateral strokes within this patient sample.
MATERIALS AND METHODS
Study Population and Inclusion Criteria
The Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke (STRATIS) registry (https://clinicaltrials.gov/ct2/show/NCT02239640) is a prospective, multicenter registry evaluating the use of the Solitaire Revascularization Device (Covidien) and the Capture low-profile revascularization device (MindFrame) in patients presenting with an acute ischemic stroke in the setting of a large intracranial vessel occlusion (clinicaltrials.gov unique identifier: NCT02239640). Details of the registry have been previously reported.9 Ethics approval was received from the local institutional review board. Stroke etiology was classified according to the TOAST criteria1 as either large-artery atherosclerosis (the presence of >50% stenosis of the carotid or a major intracranial branch artery), cardioembolic (the presence of a cardiac embolic source such as atrial fibrillation detected on an electrocardiogram or a left atrial appendage thrombus detected on transthoracic or transesophageal sonography), small-vessel disease (the presence of lacunar infarction), other rare etiologies (eg, hypercoagulopathies), or undetermined source/cryptogenic (all other categories have been ruled out and the etiology cannot be determined, or multiple competing causes are present). In this study, only patients with cardioembolic and cryptogenic strokes (as classified by the investigator) were included, ie, those with large-artery atherosclerosis (>50% carotid or major intracranial branch stenosis) and small-vessel disease were excluded. Furthermore, assessment of both extracranial carotid arteries was mandatory for inclusion, ie, patients with extracranial carotid artery occlusion and those for whom neck CTA imaging was not available were excluded. We also excluded patients for whom no clinical data were available. Informed consent was obtained before the study from all individuals.
Image Analysis
Head and neck CTA collected from patients within 7 days of symptom onset was used to review carotid morphology. All CTAs were assessed before endovascular treatment. A radiologist and neurologist read all images by consensus using OsiriX 9.5.2 imaging software (http://www.osirix-viewer.com). Conflicts were resolved by a senior neuroradiologist. The readers were blinded to clinical information and follow-up imaging at all times. The interobserver agreement (unweighted κ) between the 2 observers was 0.7 (Online Supplemental Data).
The following plaque features were reported for both carotid arteries in each patient: degree of stenosis (≤30% versus 31%–50%), maximum plaque thickness (in millimeters), the presence of plaque irregularity, ulceration (defined as contrast in a plaque extending >1 mm beyond the opacified lumen with indentation, fissure, or erosion on the luminal surface of a plaque), focal hypodensity, and the presence of a carotid web and plaque calcification (predominantly calcified plaque [≥50% calcified plaque components] versus predominantly noncalcified [<50% calcified plaque components]). The degree of stenosis was measured as per the NASCET criteria2 (≤30% versus 31%–50%). Carotid stenosis was measured on axial source images at the narrowest portion of the carotid bulb/proximal internal carotid artery after a straight course of the artery perpendicular to the axial plane had been confirmed on sagittal images. In vessels with substantial tortuosity, the degree of stenosis was measured on either sagittal or coronal images, depending on the orientation of the course of the artery. The distal internal carotid artery diameter was measured 1- to 2-cm distal to the bulb, where the vessel walls are parallel and no longer tapering.10 Plaque features were identified for both carotid arteries in each patient. These were the following: degree of stenosis (≤30% versus 31%–50%), plaque thickness (in millimeters, in which the abluminal marker was set at the interface between vessel wall and surrounding tissue and the inner marker was set at the interface between plaque and vessel lumen), the presence of plaque irregularity (qualitative assessment of the surface of the plaque that is not smooth but without a crater),11,12 ulceration11 (qualitative assessment of crater/ulcer presence at the plaque surface), focal areas of hypodensity within the plaque (yes/no) (plaque hypodensity was defined as plaque density values that are unequivocally hypodense compared with the adjacent vessel wall on visual inspection),11 and the presence of carotid web (yes/no)13,14 and plaque calcification (yes/no).15
Donut sign for intraluminal carotid thrombus was defined as a filling defect within the lumen completely surrounded by contrast on at least 2 contiguous axial source images.16 Plaques were classified as either predominantly calcified (calcified plaque component on visual assessment ≥50%) or predominantly noncalcified. A carotid web was identified when there was a thin, smooth, membrane-like intraluminal filling defect along the posterior wall of the carotid bulb on oblique sagittal images and a corresponding thin septum on axial images.17 An unremarkable carotid artery was defined by the absence of any carotid plaque, web, or intraluminal thrombus. In keeping with a previous publication of our group, nonstenotic carotid plaque was defined as the presence of ≥1 plaque in the cervical ICA with <50% luminal narrowing. Isolated, small (<2 mm), abluminal calcifications without any luminal narrowing were not considered nonstenotic plaque.13 We deliberately excluded predominantly calcified plaques from this definition because they have been shown to be less likely to be symptomatic.14 Thus, carotid arteries with isolated abluminal calcifications were included in plaque feature analysis but were excluded from the definition of SyNC. An unremarkable carotid artery was defined by the absence of any carotid plaque, web, or intraluminal thrombus.
The outcome of interest was ipsilateral/“concordant,” defined as strokes due to occlusion of an intracranial vessel in the territory of the ipsilateral ICA vascular territory. Bilateral and posterior circulation strokes were, therefore, not classified as ipsilateral/concordant strokes because these strokes are in a vascular territory that is not supplied by the ipsilateral carotid artery; hence, they cannot be caused by a nonstenotic carotid plaque in the carotid artery. Figures 1⇓–3 show some examples of predominantly calcified and noncalcified nonstenotic carotid plaques, respectively, in patients with ipsilateral ischemic stroke. All imaging was also assessed for the presence of intracranial atherosclerotic disease (>50% stenosis).

Sagittal oblique reformatted and axial CT angiographic images of exemplary cases of nonstenotic carotid plaques with varying morphology in patients with ipsilateral ischemic stroke. All plaques were classified as predominantly calcified. A, Predominantly calcified plaque. B, C, and D, Predominantly calcified plaque with hypodense plaque features.

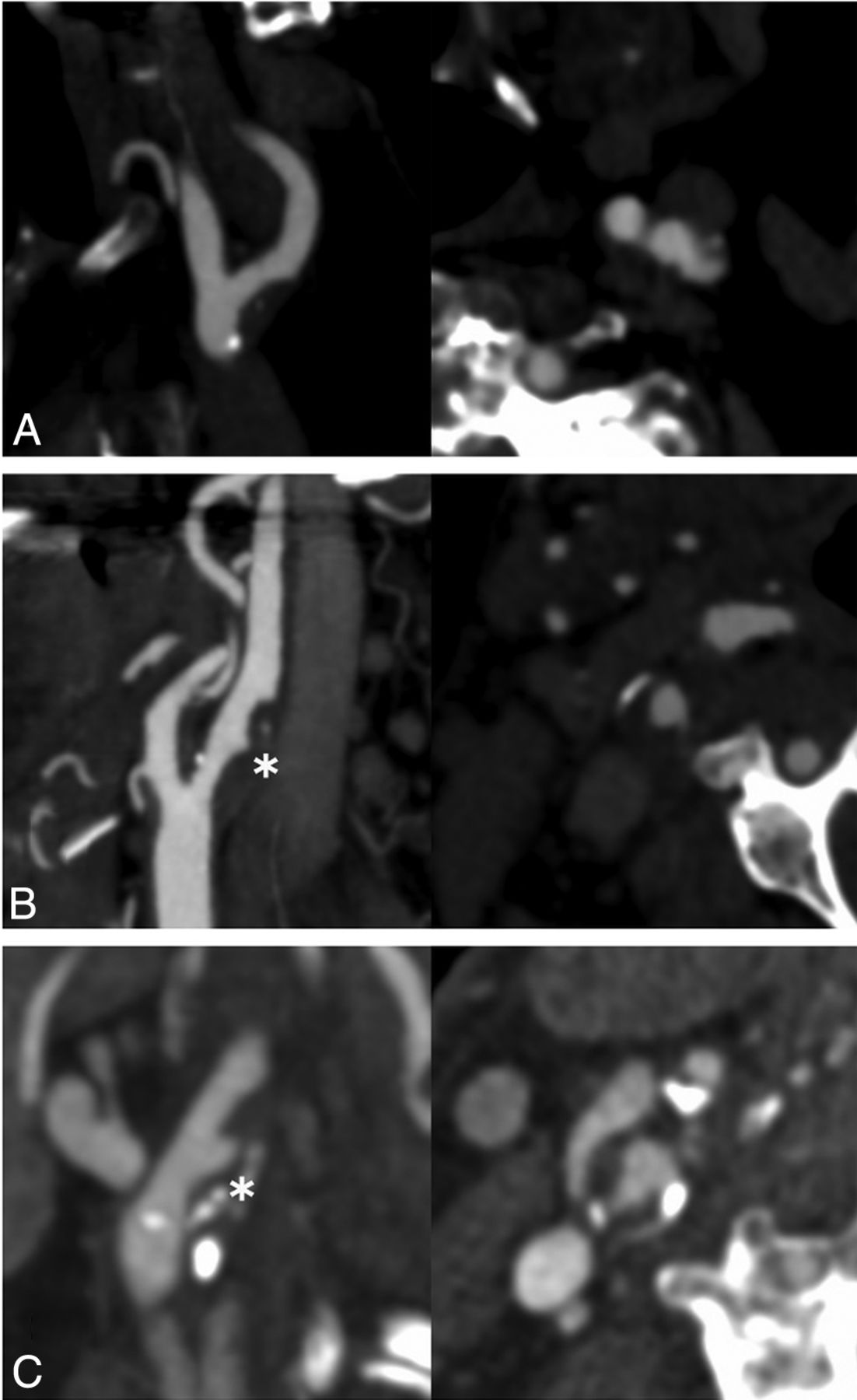
Sagittal oblique reformatted and axial CT angiographic images of exemplary cases of nonstenotic carotid plaques with varying morphology in patients with ipsilateral ischemic stroke. All plaques were classified as predominantly noncalcified. A, Predominantly noncalcified and hypodense plaque. B, Predominantly noncalcified, hypodense, and irregular plaque. C, Predominantly noncalcified, hypodense, and ulcerated plaque.

Sagittal oblique reformatted and axial CT angiographic images of exemplary cases of nonstenotic carotid disease with varying morphology in patients with ipsilateral ischemic stroke. A, Predominantly noncalcified plaque with an irregular surface. B, Carotid web. C, Predominantly noncalcified plaque with ulceration. D, Predominantly noncalcified plaque with hypodense plaque features.
Statistical Analysis
Baseline characteristics and imaging features for the overall patient sample and for the cryptogenic and cardioembolic subgroups, respectively, were reported using descriptive statistics. The prevalence of any nonstenotic carotid plaque and differences in baseline characteristics of patients with cryptogenic and cardioembolic strokes with-versus-without nonstenotic carotid plaques were assessed with the Fisher exact test (categoric variables) and the Wilcoxon rank sum test (continuous variables). We then conducted additional analyses on a carotid level to determine the prevalence of nonstenotic carotid plaques on ipsilateral-versus-contralateral strokes in cryptogenic and cardioembolic strokes. Differences were assessed using the Fisher exact test. In a next step, univariable logistic regression analysis was performed to assess whether any of the assessed plaque features were significantly associated with ipsilateral stroke in both subgroups (on a carotid level). In case of a statistically significant association in univariable analysis, multivariable analysis was performed with adjustment for patient age and sex as forced variables. Because the unit of analysis was the carotid artery, the patient was included as a cluster variable in the model.15,18 Adjusted and unadjusted odds ratios were reported for these models with their corresponding 95% CIs. Two-sided P < .05 was considered statistically significant. Statistical analysis was performed with STATA/MP 15.1 (StataCorp).
RESULTS
Of 946 patients included in the registry, 381(36%) were excluded due to lack of imaging data. Of the remaining 565 patients, 130 (23%) were classified as having stroke due to large-artery atherosclerosis and were excluded. Of the remaining 435 patients, 174 (40%) patients were classified as having cryptogenic stroke and 261 patients (60%) were classified as having cardioembolic stroke. Of those, ICAs could be assessed bilaterally in 141 patients with cryptogenic stroke and 226 with cardioembolic stroke who were included in the following analysis (Online Supplemental Data). None of the patients had evidence of intracranial stenosis. In patients who received alteplase, the mean onset-to-alteplase time was 113.4 (SD, 50.5) minutes. Baseline clinical and imaging characteristics of the overall cohort and patients with cryptogenic and cardioembolic strokes can be found in Table 1.
Patient baseline characteristics for the entire patient sample (n = 367), patients with cardioembolic stroke (n = 226), and patients with cryptogenic stroke (n = 141)
Prevalence of Nonsenotic Carotid Plaques in Cryptogenic and Cardioembolic Subgroups
The prevalence of nonstenotic carotid plaque on any side was 65/367 (17.7%), of which 23 patients (6.3%) had bilateral nonstenotic carotid plaques. The prevalence of nonstenotic carotid plaque in the cardioembolic and cryptogenic subgroups was 33/226 (14.6%) and 32/141 (22.7%), respectively, whereas 10/226 (4.4%) patients with cardioembolic stroke and 13/141 (9.2%) with cryptogenic stroke had bilateral nonstenotic carotid plaques. Baseline characteristics for patients with-versus-without nonstenotic carotid plaques for both subgroups are shown in the Online Supplemental Data. Patients with cryptogenic stroke with nonstenotic carotid plaques were younger than those with cryptogenic stroke without nonstenotic carotid plaques (median, 71; interquartile range [IQR], 60–79; and median, 61 years; IQR, 51–71), respectively, p value 0.20). No significant differences in baseline characteristics were seen in patients with cardioembolic stroke.
Prevalence of Ipsilateral/Nonstenotic Carotid Plaques (Carotid-Level Analysis).
In patients with cardioembolic stroke, nonstenotic carotid plaques were significantly more common ipsilateral to the side of the stroke than contralateral to it (35/210 [16.7%] ipsilateral versus 23/242 [9.5%] contralateral, P = . 025). In patients with cryptogenic stroke, nonstenotic carotid plaques were nominally also more frequent ipsilateral to the side of the stroke (31/130 [23.9%] ipsilateral versus 24/152 [15.8%] contralateral), though the difference did not reach statistical significance (P = . 099; Table 2).
Ipsilateral and contralateral nonstenotic carotid plaque in patients with cryptogenic and cardioembolic stroke
In univariable analysis, nonstenotic carotid plaques were significantly associated with ipsilateral/concordant strokes in cryptogenic stroke (unadjusted OR = 1.67; 95% CI, 1.04–2.69) and cardioembolic strokes (unadjusted OR = 1.90; 95% CI, 1.15–3.16). After we adjusted for patient age and sex with patient as a cluster variable, this relationship remained significant (cryptogenic stroke: adjusted OR [aOR] = 1.69; 95% CI, 1.05–2.73; cardioembolic stroke: aOR = 1.91; 95% CI, 1.15–3.18).
Carotid Plaque Features Associated with Ipsilateral Ischemic Stroke (Carotid-Level Analysis).
In univariable analysis, none of the plaque features were significantly associated with ipsilateral stroke in the cardioembolic subgroup. Thus, multivariable analysis was not performed. In the cryptogenic subgroup, plaque irregularity (aOR = 2.50; 95% CI, 1.22–5.14), plaque hypodensity (aOR = 1.89; 95% CI, 1.14–3.14), and maximum plaque thickness (aOR = 1.29; 95% CI, 1.05–1.57) were significantly associated with ipsilateral stroke, with nearly twice the odds of ipsilateral stroke. These associations were not confounded after adjusting for patient age, sex, and clustering by patients (Table 3).
Plaque features with significant association with ipsilateral strokes in patients with cryptogenic and cardioembolic strokes
Thus, we found an absolute risk of ipsilateral stroke with nonstenotic carotid plaques to be twice as high in the cardioembolic group and 1.5 times higher in cryptogenic group compared with the contralateral side (Table 2).
DISCUSSION
In this population of patients with acute ischemic stroke with proven intra-arterial occlusion, we found a significant association of nonstenotic carotid plaques with ipsilateral stroke in the cardioembolic group and a numeric increase in nonstenotic carotid plaques on the ipsilateral side in the cryptogenic group compared with the contralateral side. Nonstenotic plaques were more common on the ipsilateral side in the cryptogenic (23.9%) group versus the cardioembolic group (16.7%). These findings are in line with growing evidence suggesting nonstenotic carotid plaques as a potential etiology in ischemic stroke. Another recent substudy from the INTERRSeCT dataset of 138 patients with ESUS also showed that nonstenotic carotid plaques were significantly more common on the side of the stroke, suggesting a possible causal role.13 This study differs from the INTERRSeCT substudy because it includes only patients with large-vessel occlusion. In addition, it tries to assess the association of ipsilateral stroke in patients with a presumed cardioembolic etiology. Another study by Kopczak et al19 analyzed carotid artery plaques (CAPs) using MR imaging in patients with cryptogenic stroke compared with patients with stroke with small-vessel disease or cardioembolic stroke. They found a significantly higher prevalence of ipsilateral complicated carotid artery plaques in patients with cryptogenic stroke than in the reference group (31% versus 15%). Yet another study used a CTA-based assessment of plaque thickness and showed that plaque thickness was greater on the side of the ipsilateral stroke in the ESUS subgroup.20 These findings highlight the potential role of SyNC contributing to stroke mechanisms on the basis of morphologic features beyond the degree of stenosis.
We could not identify significant association between specific plaque features and ipsilateral stroke in the cardioembolic group. However, in the cryptogenic group, we could identify plaque features (plaque hypodensity, irregularity, and maximum plaque thickness) that were significantly more common on the ipsilateral side, even after adjusted analysis. These findings are hypothesis-generating and contribute to the identification of vulnerable plaques.14,21 They also suggest that a subset of cryptogenic strokes may be caused by these vulnerable plaques with significant plaque burden, despite low-grade luminal stenosis. Even though the strength of association of nonstenotic carotid plaques and ipsilateral stroke was higher with cardioembolic stroke than in the cryptogenic group, we found more high-risk plaque features in the cryptogenic stroke population.
Another recent study concluded that high-risk plaques were more prevalent ipsilateral to the ischemic hemisphere across several stroke subtypes (especially ESUS and cardioembolic categories), and accounting for them could have led to reclassification of the stroke etiology in up to 15% of cases in their sample.7 These observations support the possible causal association between nonstenotic carotid plaques and stroke, especially in patients presumed to have a cardioembolic etiology. Nevertheless, in the presence of a competing etiology, it would be prudent to see the distribution of DWI findings on MR imaging. The presence of DWI findings beyond a vascular territory or involving multiple vascular territories would support a cardioembolic etiology. In this study, we considered a stroke to be ipsilateral only in the absence of evidence of stroke in other arterial territories, further substantiating our findings. However, 64% of patients did not have follow-up MR imaging, and CT scans were used for assessment of stroke, which are not sensitive for detecting smaller embolic strokes. In addition, patients underwent endovascular thrombectomy, and small diffusion lesions outside the expected territory could be related to the procedure.
Results from these studies and several others are similar to ours and support our belief of moving beyond conventional stenosis measures to categorize carotid disease and broaden our horizon to identify stroke etiology, especially in the cryptogenic subpopulation.8,16,22⇓–26
Limitations
This study has several limitations. We used nonrandomized data that were analyzed in a retrospective fashion, and patients with missing imaging data were excluded, possibly having led to some selection bias. We do not have a detailed reasoning for lack of imaging data, but we suspect that this could be due to problems with the transfer of images. In addition, the registry included only patients with large-vessel occlusion, forming only a piece of the total population of ischemic stroke. It may be that these patients had a nonstenotic plaque on the ipsilateral side to begin with, which may have dislodged into the anterior circulation, leading to large-vessel occlusion. It may be insightful to assess the prevalence of these nonstenotic carotid plaques in patients with minor stroke and/or the non-large-vessel occlusion population.
There are no validated criteria for carotid plaque assessment on CTA. The degree of stenosis and plaque measurements were obtained on axial CTA source images, but it is not uncommon to see the carotid artery following a curved course that is not perpendicular to the axial plane. This may have limited the accuracy of our measurements in comparison with more complex planimetric and volumetric measurements.12 We did not use high-resolution MR imaging to identify plaque features, which may have led to underreporting of plaque features such as ulceration. However, we aimed to assess plaque features in a manner that could be easily used in the acute stroke setting. Owing to one-time cross-sectional assessment, we were unable to comment on nonstenotic plaques ipsilateral to the asymptomatic hemisphere as they may have caused events in the past or may become symptomatic in future. The registry did not capture the side of previous strokes/TIAs, and it was, therefore, not possible to correlate previous stroke location to carotid vascular territories. In addition, we did we not have sufficient data on cardiovascular risk factors and workflow times for a detailed analysis. From an etiologic classification standpoint, a detailed cardiology work-up, including 24-hour electrocardiograms and echo-cardiograms, was not available for most patients in this dataset, and a cryptogenic etiology was investigator-determined. Thus, some patients with >1 cause may have been classified into this category. Last, these findings prove only an association and not causation. Larger longitudinal prospective studies are needed to establish a causal link between nonstenotic carotid plaques and ipsilateral ischemic stroke.
CONCLUSIONS
We found a significant association between the presence of nonstenotic carotid plaques with ipsilateral strokes in patients with both cryptogenic and cardioembolic strokes. Plaque hypodensity, irregularity, and maximum plaque thickness were significantly associated with ipsilateral strokes in the cryptogenic group. This finding suggests that nonstenotic carotid plaques could be a potential stroke etiology in patients with ischemic stroke who are classified into causes other than large artery disease. Further research to confirm a causative role of nonstenotic carotid plaques and to identify potential high-risk plaque features on CTA and other imaging modalities is needed.
Footnotes
Disclosures: Osama O. Zaidat—UNRELATED: Consultancy: Consultant/advisory board member at the National Institutes of Health (NIH) StrokeNet, Penumbra, Medtronic Neurovascular, Codman, and Stryker; Grants/Grants Pending: grant for the multicenter TESLA study; Patents (Planned, Pending or Issued): Galaxy Therapeutics and O.O.Z., Comments: grants under Galaxy Therapeutics and to O.O.Z. Nils H. Mueller-Kronast—RELATED: Fees for Participation in Review Activities such as Data Monitoring Boards, Statistical Analysis, Endpoint Committees, and the Like: Medtronic, Comments: Steering Committee of the STRATIS registry. David S. Liebeskind—RELATED: Consulting Fee or Honorarium: Medtronic, Comments: imaging core lab; UNRELATED: Consultancy: Cerenovus, Genentech, Medtronic, Stryker, Vesalio, Comments: imaging core lab. Mayank Goyal—RELATED: Consulting Fee or Honorarium: Medtronic, Comments: advice on acute stroke intervention; UNRELATED: Consultancy: Stryker, MicroVention, Mentice; Grants/Grants Pending: Stryker, Cerenovus, NoNO*; Patents (Planned, Pending or Issued): GE Healthcare, MicroVention; Royalties: GE Healthcare, MicroVention. *Money paid to the institution.
References
- Received January 4, 2021.
- Accepted after revision April 27, 2021.
- © 2021 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Symptomatic non-stenotic carotid disease: current challenges and opportunities for diagnosis and treatment
- MR Imaging of Carotid Artery Atherosclerosis: Updated Evidence on High-Risk Plaque Features and Emerging Trends
- Symptomatic non-stenotic carotid disease: current challenges and opportunities for diagnosis and treatment
- Nonstenotic Carotid Plaques and Embolic Stroke of Undetermined Source: A Multimodality Review