
Abstract
BACKGROUND AND PURPOSE: The slow adoption of new advanced imaging techniques into clinical practice has been a long-standing challenge. Principles of implementation science and the reach, effectiveness, adoption, implementation, maintenance (RE-AIM) framework were used to build a clinical vessel wall imaging program at an academic medical center.
MATERIALS AND METHODS: Six phases for implementing a clinical vessel wall MR imaging program were contextualized to the RE-AIM framework. Surveys were designed and distributed to MR imaging technologists and clinicians. Effectiveness was measured by surveying the perceived diagnostic value of vessel wall imaging among MR imaging technologists and clinicians, trends in case volumes in the clinical vessel wall imaging examination, and the number of coauthored vessel wall imaging–focused publications and abstracts. Adoption and implementation were measured by surveying stakeholders about workflow. Maintenance was measured by surveying MR imaging technologists on the value of teaching materials and online tip sheets. The Integration dimension was measured by the number of submitted research grants incorporating vessel wall imaging protocols. Feedback during the implementation phases and solicited through the survey is qualitatively summarized. Quantitative results are reported using descriptive statistics.
RESULTS: Six phases of the RE-AIM framework focused on the following: 1) determining patient and disease representation, 2) matching resource availability and patient access, 3) establishing vessel MR wall imaging (VWI) expertise, 4) forming interdisciplinary teams, 5) iteratively refining workflow, and 6) integrating for maintenance and scale. Survey response rates were 48.3% (MR imaging technologists) and 71.4% (clinicians). Survey results showed that 90% of the MR imaging technologists agreed that they understood how vessel wall MR imaging adds diagnostic value to patient care. Most clinicians (91.3%) reported that vessel wall MR imaging results changed their diagnostic confidence or patient management. Case volumes of clinical vessel wall MR imaging performed from 2019 to 2022 rose from 22 to 205 examinations. Workflow challenges reported by MR imaging technologists included protocoling examinations and scan length. Feedback from ordering clinicians included the need for education about VWI indications, limitations, and availability. During the 3-year implementation period of the program, the interdisciplinary teams coauthored 27 publications and abstracts and submitted 13 research grants.
CONCLUSIONS: Implementation of a clinical imaging program can be successful using the principles of the RE-AIM framework. Through iterative processes and the support of interdisciplinary teams, a vessel wall MR imaging program can be integrated through a dedicated clinical pipeline, add diagnostic value, support educational and research missions at an academic medical center, and become a center for excellence.
ABBREVIATIONS:
- RE-AIM
- reach, effectiveness, adoption, implementation, maintenance
- VWI
- vessel wall MR imaging
Vessel wall MR imaging (VWI) is an emerging technique for vasculopathy assessment. The primary clinical application is to differentiate among vasculopathies that cause stroke such as atherosclerosis, vasculitis, and arterial dissections.1,2 VWI was first introduced in the mid-1990s.3,4 However, even after nearly 30 years, a recent American Society of Neuroradiology (ASNR) Vessel Wall MR Imaging Study Group survey querying the clinical adoption of this technique across an international group of neuroradiologists showed that only 52% of survey respondents reported that their institution performed clinical VWI.5 The survey identified a need for educational and technical expertise and support to overcome the slow rate of clinical adoption. Understanding strategies to enhance the adoption process of new techniques and applications is needed, particularly as the next wave of innovative imaging and artificial intelligence–aided applications is fused into clinical practice.
The failure rates for implementing innovations in medicine range from 30% to 90%.6⇓-8 The translation of scientific discoveries and innovations has been called attempts to bridge over the “valley of death”9 and the implementation effort as a “failure to launch.”10 The cost in resources, time, and loss of potential benefit to patients is enormous. Recognizing a need to support translational bridges, the National Institutes of Health funded the Clinical and Translational Award Program in 2006 with >60 participating institutions by 2012. Frameworks were also designed to speed the translation of research discovery and promote the effective adoption of evidence-based interventions to improve patient care and health. Reach, effectiveness, adoption, implementation, and maintenance (RE-AIM; https://re-aim.org/) is one such framework.11 We applied the RE-AIM framework to plan and evaluate a new clinical vessel wall MR imaging program at an academic medical center. Effectiveness, adoption and implementation of the VWI program were measured through quality-improvement surveys among key stakeholders. We report best practices and how interdisciplinary teams were established leading to the successful scaling of this imaging program.
MATERIALS AND METHODS
The RE-AIM framework served as the implementation science framework for this initiative.12 This project was conducted between 2019 and March 30, 2023, and was reviewed and qualified as quality improvement by the University of Pennsylvania institutional review board. The Standards for Quality Improvement Reporting Excellence 2.0 guidelines were reviewed to report this practice improvement.13
Processes and pitfalls for six phases based on the RE-AIM framework are detailed in the Table. These six phases comprise of assessing patient and disease representativeness, patient access and facility resources (Reach domain), establishing radiology VWI expertise and interdisciplinary teams focused on patient care and education (Effectiveness domain), establishing workflows, effective communication, and best practices (Adoption and Implementation domains), and integrating and scaling the program (Maintenance domain). Contextual elements that contributed to the success, failure, pitfalls, and efficiency are qualitatively summarized based on feedback from the users and stakeholders of the program.
Study Setting and Intervention
The clinical VWI exam was the intervention and was implemented at 3 acute-care hospitals and 3 outpatient imaging centers, all of which are part of the health system of the academic medical center. Within these 6 sites, the VWI protocols were built on seven 3T (Skyra, Skyra Fit, 3 Vida, 2 PRISMA Fit) and two 1.5T (Avanto Fit and Aera) Siemens MR imaging scanners. The VWI imaging protocols built on each MR imaging scanner included protocols optimized for intracranial, scalp, and cervical carotid and vertebral artery imaging to assess intracranial vasculopathies, giant cell arteritis, and cervical carotid plaque or dissections in the neck, respectively.
Domain Outcomes and Data Analysis
Assessment of the Reach and Effectiveness domains to establish patient and disease representativeness and radiologic expertise was based on systematic reviews of the literature by the interdisciplinary team as part of a planning stage. Two surveys were also designed and distributed to the ordering clinicians and MR imaging technologists to obtain data on the Effectiveness, Adoption and Implementation, and Maintenance domains (Table). On March 30, 2023, e-mail groups and Listservs were used to distribute the surveys on a Qualtrics platform (https://www.qualtrics.com/platform/) (Online Supplemental Data) followed by 2 e-mail reminders sent 1 and 4 weeks from the initial survey distribution. The effectiveness of diagnostic value added was measured by survey results reporting the perception of the value of VWI for patient care among the ordering clinicians and the MR technologists. We also measured VWI case-volume trends between 2019 and 2022 by tallying the number of VWI fit-for-purpose examination codes. The effectiveness of educational value added was measured by trends in coauthored VWI-focused publications by the institutional interdisciplinary teams. Adoption and Implementation domains were measured by survey results among clinicians reporting the ease of ordering clinical VWI and the ease of selecting specific VWI protocols on MR imaging consoles and scanning a patient for VWI among MR imaging technologists. The Maintenance domain was measured by survey results about the value of the online tips sheets and training materials among MR imaging technologists to support scaling the program, and Integration was measured by the number of submitted research grants incorporating VWI by the interdisciplinary team. Qualitative results based on feedback from the clinicians and MR imaging technologists from the survey are summarized and provided insight into the implementation barriers. Quantitative results are reported in counts, percentages, and means.
RESULTS
Phase 1: Reach Domain—Patient and Disease Representativeness
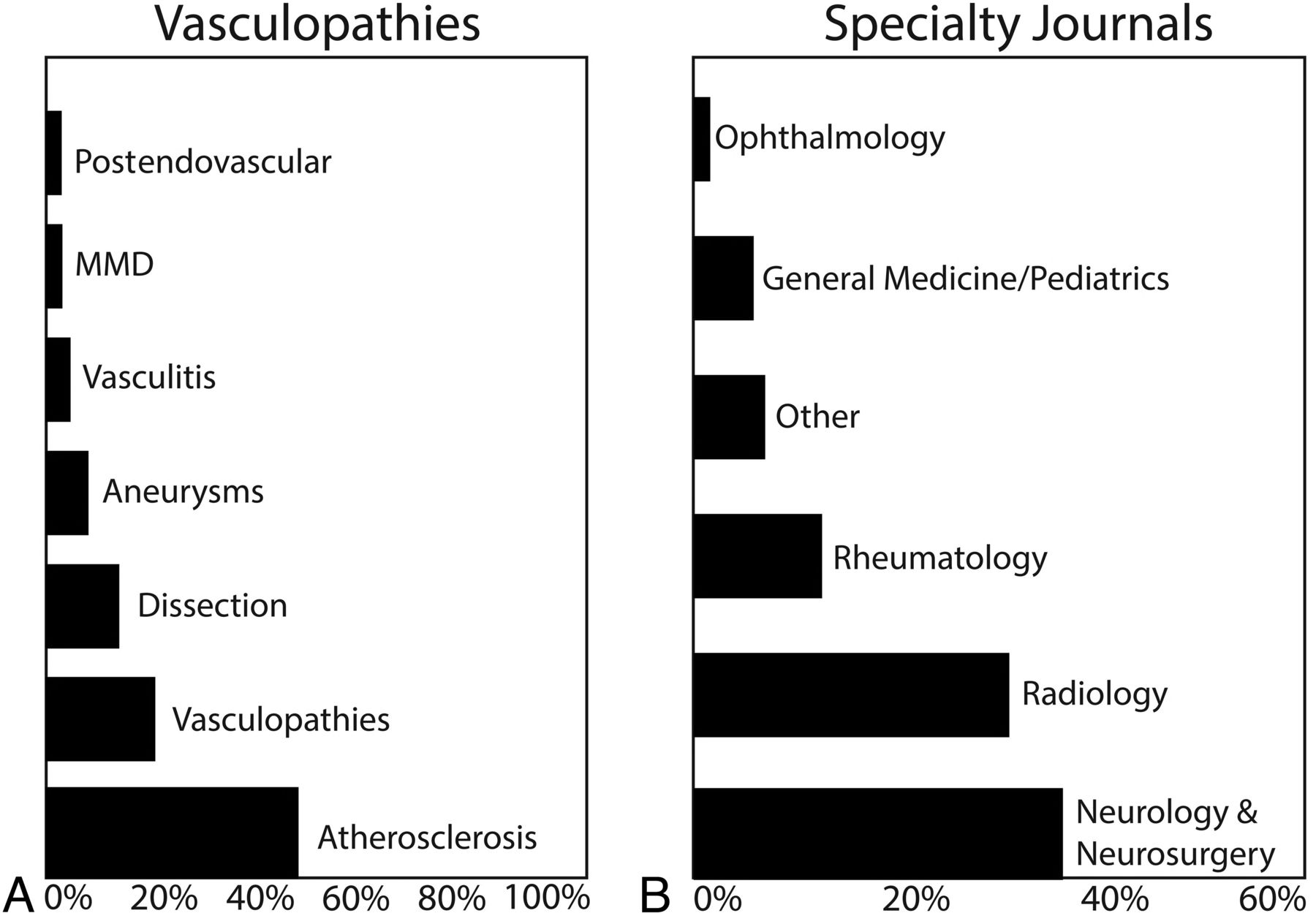
We first identified the target patient populations and the clinical specialists who care for these patients. Two systematic reviews of the literature were conducted to identify the types of vasculopathies commonly imaged using VWI and specialty journals publishing cases imaged by VWI to identify interested specialists.14,15 The results indicated that atherosclerosis was the most commonly studied vasculopathy (Fig 1A);14 neurology and neurosurgery had the most published VWI studies (Fig 1B).15 Next, to identify institutional priorities, we evaluated our local patient population and specialties with VWI interests, which included vascular neurology, neurointerventional, neuro-ophthalmology, and rheumatology. This planning phase established our needs and goals.

Reach domain: vasculopathy types and specialty journals. A, VWI and the types of vasculopathies for clinical and research applications. “Vasculopathies” include reversible cerebral vasoconstriction syndrome, vessel lesions, non-perimesencephalic hemorrhage, and radiation vasculopathy. MMD indicates Moyamoya disease/syndrome. B, Specialty journals that report on vasculopathies and vessel wall imaging findings. “Other” includes otolaryngology, infectious diseases, cardiology, oncology, and nephrology.
Pitfalls.
It was important to recognize a distinction between the use of VWI for clinical applications versus research. Tailored and efficient clinical MR imaging protocols were necessary to ensure diagnostic interpretations within a clinical MR imaging time slot. VWI protocols were not one-size-fits-all. Each protocol was designed with intention.16 Second, clinical subspecialists such as those in vascular neurology or neuro-ophthalmology often served as consultants who provided recommendations to internal medicine or emergency medicine care teams. Thus, there was a broader user base than anticipated, requiring communication and education across specialties.
Phase 2: Reach Domain—Patient Access and Facility Resources
Ensuring that VWI examinations are accessible to the target patient population was an important dimension of the Reach domain. Consistent with the principles of implementation science, we assessed available hospital and outpatient imaging facility resources to meet patient and provider needs. This assessment required careful planning and support from our MR imaging technologists and department, because we had to assess scanner availability, patient scheduling and throughput, examination volume, and the bandwidth of the MR imaging technologists. For example, acute stroke care required the VWI protocols to be available on emergency and inpatient MR imaging scanners. However, outpatient VWI requests for follow-up examinations and rheumatologic work-ups required outpatient centers to have VWI protocols to accommodate requests.
Pitfalls.
Due to the need for high-spatial-resolution imaging, 3T MR imaging scanners provide optimal quality to image the vessel walls. However, with the increasing recognition of the diagnostic value of VWI, there were requests for VWI for patients with pacemakers and discussions about hospital transfers solely to acquire VWI. The VWI protocols were thus built on 2 additional 1.5T MR imaging scanners to address this need.
Phase 3: Effectiveness—Establishing Radiology VWI Expertise
Establishing expertise as a neuroradiologist focused on 3 areas: imaging technique,16 disease and vasculopathy,14,15 and interpretation.15,17,18 Technical expertise required knowledge of VWI pulse sequences, protocols, and its limitations and optimizations.16 This expertise was acquired through the scientific literature and collaborations with MR imaging physicists. An optimized vessel wall imaging pulse sequence was used for the protocols. Disease expertise on the vasculopathy spectrum, clinical presentations, and imaging appearances was acquired through multidisciplinary collaborations, participation in multidisciplinary clinical conferences and educational initiatives, and experience. Interpretive expertise was developed through the scientific literature,15,17,18 accruing experience by interpreting VWI cases, and participating in the ASNR Vessel Wall Imaging Study Group Webinars to learn from the collective experience of VWI experts.1
Pitfalls.
First, building the VWI protocols on the different scanners was an iterative and time-consuming process, given that many of the scanners differed in model, software, and magnet strength. This step was facilitated by all MR imaging scanners being Siemens products at our institution. Quality checks were still required and performed in an iterative fashion to ensure interpretable image quality on each scanner. MR imaging technologists and the Siemens Collaboration Manager were critical for these checks. Second, imaging patients with stroke and neurologic conditions often resulted in motion-degraded VWI. However, the ability to provide valuable and diagnostic image interpretations did not necessarily rely on perfect image quality. Rather, expertise about the disease and the evolution of imaging findings and posttreatment appearance was key. The initial focus on trying to achieve perfect image quality was, in retrospect, not as crucial for clinical applications. Nevertheless, this initiative had to be balanced with a need to conduct reproducible quantitative measurements for parallel research investigations.
Phase 4: Effectiveness—Multidisciplinary Teams Focused on Patient Care and Education
Identifying leaders and champions for the VWI program among the different stakeholder groups was imperative. Among the MR imaging technologists, an MR imaging educator and a Siemens MR Collaborations Manager led support for promoting the VWI program and addressed technical challenges. Lead technologists at each site also supported and promoted the program. Among the clinicians, VWI promoters emerged through multidisciplinary engagement at case conferences and discussions included education about the utility of incorporating VWI. With challenging clinical cases, discussions about patient care naturally led to developing research questions together. Proactive engagement was through publications, preparation of research grants, lectures and case presentations to radiology, neurology, and internal medicine trainees, and grand rounds to the Department of Neurology.
Measures of Effectiveness
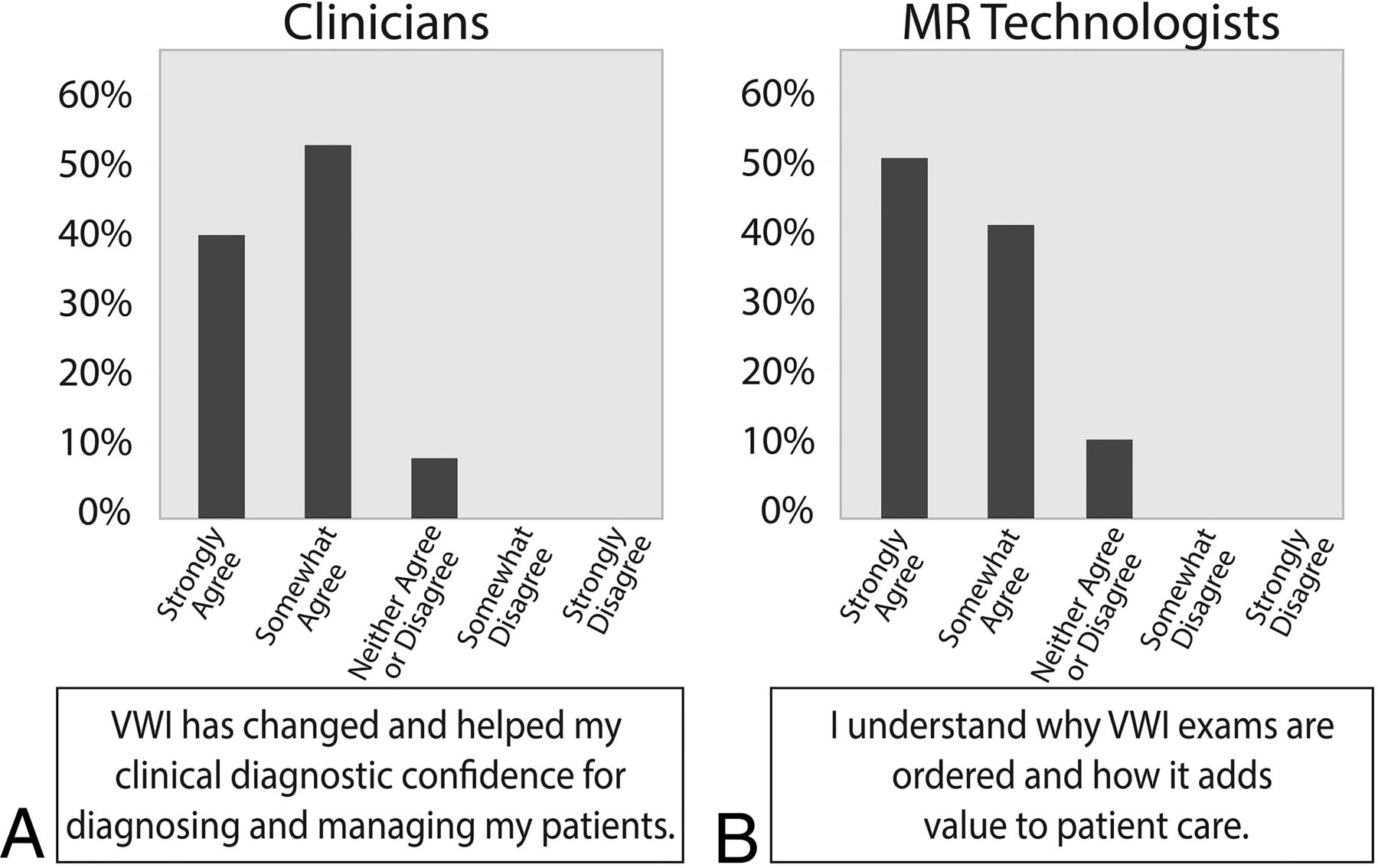
Response rates from the surveys from ordering clinicians were 71.4% (n = 30 of 42) and 48.3% (n = 14 of 29) from MR imaging technologists. Among the clinicians, 89.3% had previously ordered a VWI examination. Among clinicians who ordered VWI, 39.1% responded “Strongly Agree,” and 52.2% responded “Somewhat Agree” to the statement, “Vessel wall MR imaging has changed and helped my clinical diagnostic confidence of diagnosing and managing my patients” (Fig 2A). Among the MR imaging technologists, 100% reported that they had scanned a patient for a VWI examination and 50% responded “Strongly Agree” and 40% responded “Somewhat Agree” to the statement, “I understand why vessel wall MR imaging examinations are ordered and how it adds value to patient care” (Fig 2B).

Effectiveness domain: perceived diagnostic value among MR technologists and clinicians. A, The reported perception of the understanding of the diagnostic value of VWI for patients among clinicians. B, The reported perception of the diagnostic value of vessel wall MR imaging for patient care among MR technologists.
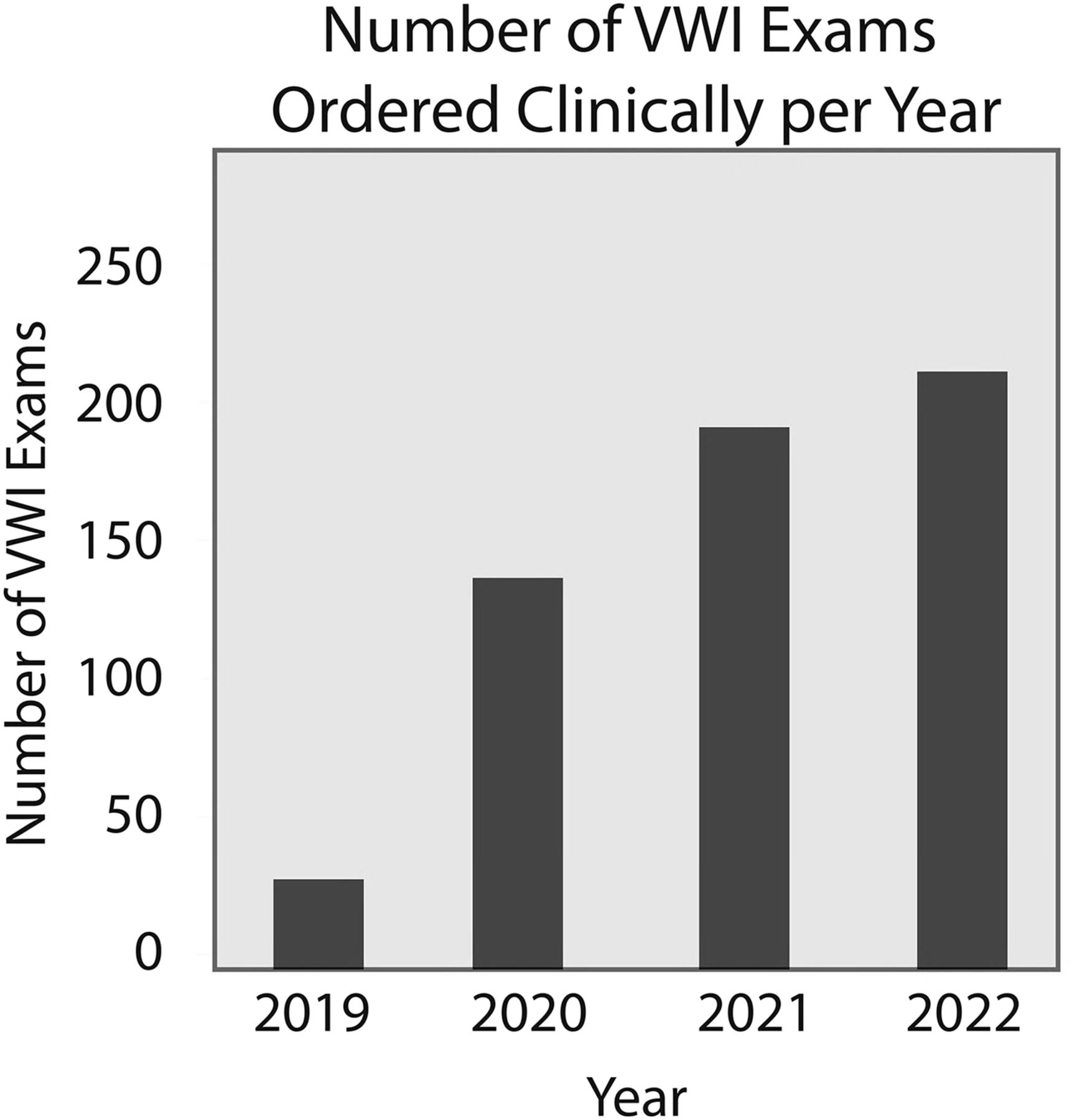
The number of clinical VWI examinations ordered and performed from January 1, 2019, to December 31, 2022, revealed increasing annual volumes rising from 22 to 205 examinations since the establishment of the program in 2019 (Fig 3).

Effectiveness domain: annual number of VWI examinations (2019–2022). The annual number of vessel wall MR imaging examinations clinically ordered and performed from 2019 to 2022 increased from 22 (2019) to 205 (2022) VWI examinations.
The number of coauthored VWI publications and accepted abstracts by the local multidisciplinary teams trended from 2 (2019), 5 (2020), 8 (2021), to 12 (2022). This effort further promoted education about VWI and engaged the teams.
Pitfalls.
As enthusiasm grew, VWI became incorporated into clinical practice algorithms. The incorporation of VWI demonstrated its value but required discussions about the appropriate use and limitations of resource-intensive MR imaging requests. These discussions highlighted a need for rigorous evidence-based effectiveness studies. A timely effort from the American College of Radiology is the formation of a committee to write a Vessel Wall Imaging Practice Parameters and Technical Standards white paper, which is currently in preparation.
Phase 5: Adoption and Implementation—Easy Work-Flows, Communication, and Best Practices
Adoption and Implementation strategies are facilitated when processes and communication are streamlined, and workflow disruptions are minimized.11 Adoption strategies were iteratively reviewed with VWI program promoters. Informal and formal feedback was proactively solicited for quality improvement to identify and address problems. Low-complexity processes, education, and engagement bring greater consistency in the delivery of a program and were our goal.19 Feedback from the survey results from clinicians indicated challenges with ordering examinations. Initially, VWI examinations were ordered as special requests after a 1:1 discussion between a clinician and a radiologist, Examinations were protocoled with typed-in instructions to the MR imaging technologists. With increasing requests, VWI fit-for-purpose examination codes were created for clinicians to order indication-specific VWI examinations. Ordering interfaces were designed with an order set to request vessel wall MR imaging and MRA examinations together. The fit-for-purpose codes facilitated communication. The clinical indication was evident in the examination name, which could be matched to the intended protocoling interface for the neuroradiologist and VWI protocol folders on the MR imaging consoles (Fig 4). This workflow improved communication and reduced phone calls for order clarifications between ordering clinicians and radiologists and MR technologists and radiologists.

Communication: team, role, and platform. We identified the primary role of each team member (ordering clinician, neuroradiologist, and MR technologist) in the workflow and established a low-complexity platform for the team member to accomplish his or her task. This workflow improved communication between clinicians and radiologists and MR technologist and radiologists. EHR indicates electronic health record.
Educating and engaging the MR imaging technologists who performed the scanning and initial image quality control were paramount. A series of short educational lectures were given during staff meetings to explain VWI clinical indications and how to assess diagnostic image quality. During the initial stages of the program, the neuroradiologist was frequently called to check images. For all cases that were monitored by the neuroradiologist, personalized feedback was provided to the MR imaging technologist. Additionally, when possible, key annotated images and diagnoses were shared with both the clinician and scanning MR technologist. This process highlighted a patient care team for the imaging workflow, which comprised the clinician, the MR imaging technologist who had direct interaction with the patient, and the radiologist.
Measures of Adoption and Implementation: Ease of Workflow
Clinicians were surveyed about the ease of ordering VWI (Fig 5A), among whom 75% responded “Yes”. The survey feedback showed that clinicians wanted more education about VWI diagnostic indications, the limitations of the examinations, and a list of available sites that perform VWI.

Adoption domain: ease of ordering VWI by clinicians and scanning by MR technologists. A, The reported perception of the ease of clinically ordering VWI among clinicians. B, The reported perception of the ease of scanning a VWI examination among MR technologists.
MR imaging technologists were surveyed about the ease of VWI protocol selection on MR imaging consoles and scanning VWI examinations (Fig 5B). One hundred percent responded that it was easy to identify the VWI protocol folders on the MR imaging consoles. Two respondents reported that scanning VWI was challenging due to remembering coverage and field-of-views for some VWI pulse sequences. Feedback from the survey indicated that MR imaging technologists were concerned about challenges with long scan times and posed a request to protocol examinations in advance.
Pitfalls.
As everyone gained more experience with VWI applications and indications were refined, VWI protocols were revised. As a result, a second iteration of the VWI fit-for-purpose examination codes was presented and approved. Initial examination codes were called “vessel wall,” which were subsequently revised to specify the clinical indications (eg, vessel wall vasculopathy, giant cell arteritis, or vessel wall dissection). Additionally, to accommodate new, rotating, and expanding work forces, an online website was created for instructions on ordering VWI by indication for clinicians and training materials on performing VWI scanning for MR imaging technologists.
Phase 6: Maintenance—Integration and Scale
The key to the sustainability of a program starts with recognizing that the new program addresses a clinical need, has purpose, and identifies knowledge gaps. Research questions were identified through ongoing discussions, especially with challenging clinical cases. Between 2019 and 2022, thirteen research grants incorporating VWI protocols were submitted for institutional, foundational, or National Institutes of Health funding. This metric is an outcome measure reflecting the integration dimension of the VWI program into an academic mission.
Second, because the clinicians valued the vessel wall imaging program, after the infrastructure was built, needs continued to increase. Processes to scale the program were started to address this need. With a changing work force of MR imaging technologists, ongoing education for the technologists was important. Survey results from the MR imaging technologists indicated that 100% found the online VWI imaging protocol tip sheets and instructions helpful, given their accessibility. Additionally, a group of 7 neuroradiologists within the neuroradiology division with cerebrovascular and advanced imaging interests were identified to become VWI superusers and accrue experience. Reporting templates, case conferences, interpretation tip sheets, and a dedicated chat group were created to share cases, for questions, and to create a forum for dialogue. Enhancing comfort levels with protocoling and assessing appropriate use, evaluating image quality, and VWI interpretations were prioritized. At the onset of the rollout initiative among neuroradiologists, all were encouraged to share input and suggestions and foster discussion.
Pitfalls.
Recognizing a neuroradiologist with expertise as a resource was important. Balancing the need to establish expertise by accruing experience through case volume and not diluting the experience were limitations to scaling. Conversely, consistency in image interpretation and minimizing long differential diagnoses and descriptive reports were also important for clinical adoption among clinicians at the beginning of the program. Interpretation tip sheets were created and VWI-focused case conferences were held to address this challenge. Another challenge was the clinical application of VWI for stroke assessment. Stroke care is emergent. During the establishment of the clinical program, nearly all cases and queries were directed to 1 neuroradiologist to ensure consistency in reporting quality and instructions to clinicians and MR imaging technologists. Creation of accessible training materials and an instructional website and expanding the program with a group of superuser neuroradiologists reduced this need to be continuously available for all cases at all times.
DISCUSSION
The successful implementation of a clinical VWI program was driven by aligning initiatives in parallel across multiple stakeholders. First, we assessed clinical care needs, teams, and resources. Second, we built optimized VWI protocols and evidence-based content to deliver tailored images and diagnostic interpretations, respectively. Third, we implemented the program through a low-complexity workflow, education, and continued engagement. High effectiveness was measured by most surveyed stakeholders reporting that VWI added diagnostic value to their patient care and manifested by the rising trends in VWI case volumes. Finally, we sustained the program by continuously refining our approach to create educational materials, evaluate outcomes, and expand the team of neuroradiologists to meet needs. The stages reflect the RE-AIM framework.
Several key strategies were identified during implementation. First, communication was key. Communication was written, verbal, and in person (eg, MR imaging technologist staff meetings and multidisciplinary conferences with clinicians). With the MR imaging technologists, personalized communication while providing oversight during real-time patient scanning was supplemented with face-to-face communication and short didactic lectures at staff meetings. These steps promoted connection. The survey showed that 90% of MR imaging technologists agreed that they understood how VWI added value to patient care. The teaching and communication during scanning and staff meetings most likely contributed to this understanding. Studies show that engagement and adherence to protocols are higher when one understands the purpose.20 A sense of community, support, engagement, and adding value to patient care also serve to improve retention.21
Second, a low-complexity workflow was critical. Iterative improvements were made to facilitate clinical workflows for clinical teams and the MR imaging technologists. For example, specific VWI indications required tailored MR imaging protocols. As a result, VWI examination codes were renamed to match the indications, such as dissection, vasculopathy, or giant cell arteritis. Refining fit-for-purpose examination codes resulted in an easier workflow. For the MR imaging technologists, an interface with protocol selection strategies was designed on the MR imaging console to facilitate VWI protocol identification. These steps likely explain why 100% of the MR imaging technologists reported that it was easy to identify named VWI protocol folders on the MR imaging consoles. Auto-protocoling these cases could be a consideration in the future to further reduce protocoling burden. Studies show that a barrier to implementation is a complex workflow or insisting on change when existing workflow is perceived sufficient.22,23 However, with new imaging programs and new tools, once the value is recognized, this perception of change as a barrier is altered and adoption is facilitated with streamlined workflows.
A barrier identified in the ASNR vessel wall imaging survey included the need for technical and vendor support for protocol development.5 An optimized intracranial VWI pulse sequence from a cerebrovascular MR imaging physicist collaborator was acquired,24 and multiple protocol revisions on the clinical MR imaging scanners across the health system were supported by a clinical MR imaging educator, a Siemens applications specialist, and site-based lead MR imaging technologists. Diversifying and partnering with these teams were critical to the success of the imaging program.
The successful adoption and maintenance of the VWI program hinged on interpretations of the clinical report. Descriptions of vessel wall findings alone were inadequate because they provided little clinical context. Providing diagnostic interpretations relied on experience and expertise. Systematic reviews of the literature supplemented the experiential expertise. Understanding the disease process and imaging manifestations was a critical component of VWI interpretation and staying relevant. The VWI interpretations are the most likely reason that 91.3% of clinician survey respondents agreed to the statement, “Vessel wall MR imaging has changed and helped my clinical diagnostic confidence of diagnosing and managing my patients.”
Several limitations of the implementation strategies of this program were based on the team experiences and survey feedback. Scope creep of an MR imaging protocol can lengthen the protocol time. We balanced innovation with clinically achievable strategies for diagnostic quality. Iterative protocol optimizations included trimming the number of pulse sequences as more diagnostic expertise was gained. A second limitation was resource allocation. The availability of neuroradiologists with expertise in VWI interpretation should be balanced with inpatients and emergency patients needing VWI 24–7. As the coronavirus 2019 (COVID-19) pandemic ended, awareness for changing management to effectively navigate resources was needed. Another consequence of the pandemic was a turnover of both clinicians and MR imaging technologists. This changing workforce required adaptability in the program. Creation and dissemination of training materials and resources were an efficient strategy. Finally, the low response rate to the surveys may be related to new staff unfamiliar with the program and prior years of iterative process changes. Nevertheless, 48% and 71% response rates among MR imaging technologists and clinicians are comparable and higher, respectively, than those in most physician surveys.25,26 The response rates also reflect the relatively small number of respondents due to the study being a single-center institutional experience.
CONCLUSIONS
We describe how to establish a new imaging program using the RE-AIM framework. The framework guided processes for implementation and highlights the importance of planning and iteratively refining processes while engaging all stakeholders. Survey results show that both clinicians and MR imaging technologists understood the diagnostic value of the VWI program. Engagement and understanding are associated with the Adoption and Implementation and Maintenance domains. Because the imaging program represents centralized knowledge and expertise, it can also drive innovation, efficiency, and excellence by addressing the patient care, education, and research missions of an academic medical center.
| Domain | Goals | Measures |
|---|---|---|
| Phase 1: Reach domain | Patient and disease representativeness | Systematic reviews of the literature |
| Phase 2: Reach domain | Patient access and facility resources | |
| Phase 3: Effectiveness domain | Establishing radiology VWI expertise | |
| Phase 4: Effectiveness domain | Interdisciplinary teams focused on patient care and education | Survey: VWI adds diagnostic value for patient care (clinicians and MR imaging technologists) |
| Clinical volume: annual trends in clinical VWI examinations | ||
| Academic-education metrics: coauthored publications and abstracts | ||
| Phase 5: Adoption and Implementation domains | Establishing workflow, effective communication, and best practices | Survey: ease of ordering a clinical VWI (clinicians) |
| Survey: ease of selecting a specific VWI protocol and ease of scanning a patient for VWI (MR imaging technologists) | ||
| Phase 6: Maintenance domain | Integration and Scale | Survey: value of online tip sheets and training materials (MR imaging technologists) |
| Academic-research metrics: grants submitted |
Six phases contextualized to the RE-AIM framework
Footnotes
J.W. Song is supported by the American Heart Association (938082).
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 22, 2023.
- Accepted after revision January 12, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.