
Abstract
BACKGROUND AND PURPOSE: Imaging assessment of brain frailty in ischemic stroke has been extensively studied, while the correlation between brain frailty and Moyamoya disease remains obscure. This study aimed to investigate the imaging characteristics of brain frailty and its clinical applications in Moyamoya disease.
MATERIALS AND METHODS: This study included 60 patients with Moyamoya disease (107 hemispheres). All patients were divided into stroke and nonstroke groups based on clinical symptoms and imaging findings. The modified brain frailty score was adapted to consider 4 imaging signs: white matter hyperintensity, enlargement of perivascular space, old vascular lesions, and cerebral microbleed. The relative CBF of the MCA territory was quantified using pseudocontinuous arterial-spin labeling. Surgical outcome after revascularization surgery was defined by the Matsushima grade.
RESULTS: The relative CBF of the MCA territory decreased as the modified brain frailty score and periventricular white matter hyperintensity grades increased (ρ = −0.22, P = .02; ρ = −0.27, P = .005). Clinically, the modified brain frailty score could identify patients with Moyamoya disease with stroke (OR = 2.00, P = .02). Although the modified brain frailty score showed no predictive value for surgical outcome, basal ganglia enlargement of the perivascular space had a significant correlation with the postoperative Matsushima grade (OR = 1.29, P = .03).
CONCLUSIONS: The modified brain frailty score could reflect a cerebral perfusion deficit and clinical symptoms of Moyamoya disease, and its component basal ganglia enlargement of perivascular space may be a promising marker to predict surgical outcome and thus aid future clinical decision-making.
ABBREVIATIONS:
- CMB
- cerebral microbleed
- EDAS
- encephaloduroarteriosynangiosis
- EPVS
- enlargement of the perivascular space
- MMD
- Moyamoya disease
- PCA
- posterior cerebral artery
- pCASL
- pseudocontinuous arterial-spin labeling
- PVS
- perivascular space
- rCBFmca
- relative CBF of the MCA
- WMH
- white matter hyperintensity
SUMMARY SECTION
PREVIOUS LITERATURE
Brain frailty is a notion reflecting brain tissue vulnerability and decline of cerebral physiologic reserve following stressor events. Previous literature has proposed the utilization of neuroimaging markers to reflect brain frailty status, including white matter hyperintensity (WMH), enlargement of periventricular space (EPVS), vascular lesion, and cerebral microbleed. There is a growing focus on brain frailty in cerebrovascular disease. However, the evaluation of brain frailty and its clinical implications in Moyamoya disease (MMD) remains unknown.
KEY FINDINGS
This study found that cerebral perfusion decreased as modified brain frailty score and periventricular WMH grades increased. Clinically, the modified brain frailty score could identify Moyamoya disease patients with stroke. Basal ganglia EPVS presented significant correlation with postoperative Matsushima grade.
KNOWLEDGE ADVANCEMENT
The current study provided new knowledge regarding the overall estimation of brain frailty by using neuroimaging markers in Moyamoya disease. The modified brain frailty score could reflect the hemodynamic status, with its constituent, EPVS, exhibiting potential in predicting postoperative revascularization.
Moyamoya disease (MMD) is an uncommon cerebrovascular disease characterized by progressive occlusion of the terminal portion of the ICA and its main branches within the circle of Willis.1 Pathologically, MMD was also presumed to be related to disorders of the small vessels (perforating arterioles, capillaries, and probably venules) of the brain.2,3 Long-term impairment of both large arteries and small vessels could lead to chronic hypoperfusion, which would eventually cause brain parenchyma changes.
Brain frailty was widely used in patients with stroke to reflect brain resilience or vulnerability.4 It could be conceptualized as the consequences associated with accumulation of multiple chronic damage.5 In most neuroimaging studies, brain frailty shares similar imaging features with cerebral small-vessel disease, including white matter hyperintensity (WMH), old vascular lesions or lacunes, brain atrophy, enlargement of the perivascular space (EPVS), and cerebral microbleed (CMB).6,7 These features were associated independently with a poor outcome of stroke and represent markers of brain frailty.8 However, the role of brain frailty in MMD remains largely unknown. In this study, we introduced a modified brain frailty score for MMD based on the research by Duan et al.7 The modified brain frailty score involved imaging assessments of WMH, old vascular lesions, EPVS, and CMB.
This study aimed to evaluate the imaging characteristics of brain frailty in MMD and further investigate the clinical implications of brain frailty and its component imaging findings.
MATERIALS AND METHODS
Patient Characteristics
This observational study was approved by the institutional ethics committee and registered as a clinical trial (NCT03785171). Written informed consent was obtained from each patient or his or her legally authorized representative.
From September 2018 to June 2019, this cross-sectional, prospective study consecutively enrolled patients with MMD according to the Japanese guidelines published in 2012, excluding Moyamoya syndrome.9 All patients underwent MR imaging and were divided into stroke MMD (ischemic or hemorrhagic stroke confirmed by both clinical symptoms and imaging findings, including acute and chronic phases) and nonstroke MMD. In stroke MMD, the cerebral lesion found on imaging should be responsible for the clinical symptoms. Symptoms of nonstroke MMD were defined as episodic or nonspecific symptoms, such as TIA, headache, dizziness, and other symptoms without responsible structural lesions. The exclusion criteria were as follows: 1) patients 18 years of age or younger; 2) patients who previously underwent bypass surgery (direct or indirect revascularization); 3) hemispheres that showed a normal ICA and MCA without steno-occlusion; 4) patients with a history of systemic diseases such as terminal carcinoma and immune system diseases; and 5) poor imaging quality that prevented further imaging analysis.
Imaging Acquisition and Assessments
Imaging Acquisition.
All patients were scanned on a 3T Discovery 750 MR scanner (GE Healthcare) with an 8-channel phased array head coil. Detailed MR imaging parameters were as follows: 1) FLAIR: TR = 6000 ms, TE = 160 ms, section thickness = 6 mm; 2) pseudocontinuous arterial-spin labeling (pCASL): TR = 4844 ms, TE = 10.5 ms, labeling duration = 1500 ms, postlabeling delay = 2000 ms, section thickness = 4 mm; 3) DWI: TR = 6800 ms, TE = 90 ms, b=0 and 1000 s/mm2, section thickness = 5 mm; 4) TOF-MRA: TR = 34 ms, TE = minimum, section thickness = 1 mm; 5) T2-weighted imaging: TR = 5752 ms, TE = 93 ms, section thickness = 6 mm; 6) SWI: TR = 33.5 ms, TE = 37.9 ms, section thickness = 3 mm; 7) high-resolution T1-weighted structural imaging: TR = 6 ms, TE = 2.5 ms, section thickness = 1 mm.
DSA was performed after contrast injection in both ICAs, both external carotid arteries, and 1 or 2 vertebral arteries. Lateral and anterior-posterior views of each artery injection were collected.
Brain Frailty Assessment.
Brain frailty was assessed by 2 radiologists with 5 years of experience in neuroimaging who were blinded to the clinical information. The Fazekas scale was used to score the severity of periventricular WMH (0, absence; 1, “caps” or pencil-thin lining; 2, smooth “halo”; 3, irregular hyperintensities extending into deep white matter and deep WMH (0, absence; 1, punctate foci; 2, beginning confluence of foci; 3, large confluent areas).10 The severity of basal ganglia EPVS was rated according to the study by Potter et al:11 grade 0 (none), grade I (1–10), grade II (11–20), grade III (21–40), and grade IV (> 40). The presence of EPVS was carefully identified from lacunes.12 Old vascular lesions were defined as ischemic or hemorrhagic lesions of the brain parenchyma, including lacunar infarction. CMB was rated on SWI as hypointense lesions. In this study, brain atrophy was not considered a component of brain frailty because it is not common in patients with MMD.
The modified brain frailty score was calculated as the sum of each point, ranging from 0 to 4:13 One point was given when ≥1 vascular lesion was present, 1 point was given when ≥1 CMB was present, 1 point was assigned when periventricular WMH was Fazekas 3 and/or deep WMH was Fazekas 2–3, and 1 point was assigned when moderate-to-severe EPVS (grades II–IV) was present in the basal ganglia.
Estimation of CBF.
Quantitative estimation of CBF of the MCA territory was performed using the Clinical Toolbox (https://www.nitrc.org/projects/clinicaltbx) for Statistical Parametric Mapping (SPM12; https://www.fil.ion.ucl.ac.uk/spm) on a Matlab platform (R2020a; MathWorks). First, the CBF map of pCASL was generated using the FuncTool from AW 4.5 Workstation (GE Healthcare). Second, CBF maps were coregistered to original T1 images. Third, high-resolution T1 structural images were normalized to the Montreal Neurological Institute space using the Clinical Toolbox. This toolbox normalizes the high-resolution T1 images to Montreal Neurological Institute space with a combination of lesion maps, minimizing the influence of cerebral lesions. Each lesion map was manually delineated on original T1 images with FLAIR images as references. Fourth, the coregistered CBF maps were normalized to Montreal Neurological Institute space using the formerly generated deformation field for T1 images. Fifth, the normalized CBF maps were spatially smoothed by a 6-mm full width at half maximum Gaussian kernel. Sixth, a brain mask of the MCA territory was projected to the CBF maps, which has been described elsewhere.14
Eighteen hemispheres showed large, chronic infarctions exceeding the threshold of 15 mm for lacunes (10 lesions on the left hemisphere, 8 on the right). Those lesions were subtracted from the mask before calculating the mean CBF. We also calculated the mean lesion map showing the spatial distribution of those lesions. Seventh, a study-specified VOI in the ipsilateral cerebellum was used to reflect the relative decrease of CBF of MCA territory according to study by Calviere et al.15 Finally, the mean CBF of the MCA territory of each hemisphere and the cerebellum was extracted. The CBF of the MCA territory was defined as CBFmca, while the CBF of the cerebellum was CBFcerebellum. The adjusted ratio of the CBF of the MCA territory against the ipsilateral cerebellum was defined as relative CBF of the MCA (rCBFmca).
Assessment of Matsushima Grade at Follow-Up.
Fifty patients underwent encephaloduroarteriosynangiosis (EDAS) surgery. At least 3 months after surgery, postoperative revascularization of 27 patients (44 hemispheres) was graded using the Matsushima grade on DSA:16 Grade I indicates revascularization of less than one-third of the MCA distribution, grade II represents revascularization of one-third to two-thirds of the MCA distribution, and grade III indicates revascularization of more than two-thirds of the MCA distribution. Surgical outcome was defined as favorable (Matsushima grade III) and poor (Matsushima grade I–II).
Statistical Analysis
The test for agreement was calculated to assess interrater reliability. The Kolmogorov-Smirnov test was used to assess data normality. Two-sample t tests for continuous data and χ2 tests or Fisher exact tests for categoric data were used for comparative analysis. The Spearman correlation analysis was used for correlational analysis. Ipsilateral posterior cerebral artery (PCA) involvement was considered a covariant because the leptomeningeal collateral from the PCA is a major source of blood supply in MMD.17 PCA involvement was defined as moderate-to-severe stenosis or occlusion. Logistic regression analysis was used to assess the modified brain frailty score and other variables (age, sex, PCA involvement, and vascular risk factors) in differentiating stroke from nonstroke MMD and to predict the postoperative Matsushima grade. Variables were selected in multivariate logistic regression analyses with a P < .10 threshold. P < .05 was considered statistically significant. All statistical analyses were performed using SPSS 26.0 (IBM).
RESULTS
Clinical and Imaging Characteristics
Sixty-seven patients with MMD were enrolled in this study, while 7 patients were excluded due to poor image quality or incomplete MR imaging sequences. As a result, 60 patients with MMD were finally analyzed, including 13 unilateral and 47 bilateral cases, for a total of 107 hemispheres. Of all patients who underwent EDAS surgery, 27 patients (44 hemispheres) underwent follow-up DSA assessment, with an average interval of 10.6 (SD, 4.8) months. The Online Supplemental Data provide a summary of included patients with MMD. Figure 1 shows the flow diagram of image-processing and patient enrollment in this study.

Flow diagram (A) and patient inclusion (B) in this study.
The interrater κ values for periventricular WMH, deep WMH, basal ganglia EPVS, vascular lesions, and CMB were 0.83, 0.83, 0.76, 0.92, and 0.80, respectively. Figure 2 presents a case of MMD. Figure 3 shows DSA images of postoperative Matsushima grades. The group-level lesion map shows that most large lesions were located at the frontotemporal and temporo-occipital watershed area (Fig 4). Between hemispheres with and without PCA involvement, the modified brain frailty score (χ2 = 14.49, P = .006), periventricular WMH (χ2 = 15.18, P = .002), and deep WMH (χ2 = 18.38, P < .001) showed significant differences, while the EPVS (χ2 = 0.18, P = .91), vascular lesions (χ2 = 1.50, P = .22), and CMB (χ2 = 4.68, P = .06) could not differentiate the 2 groups.

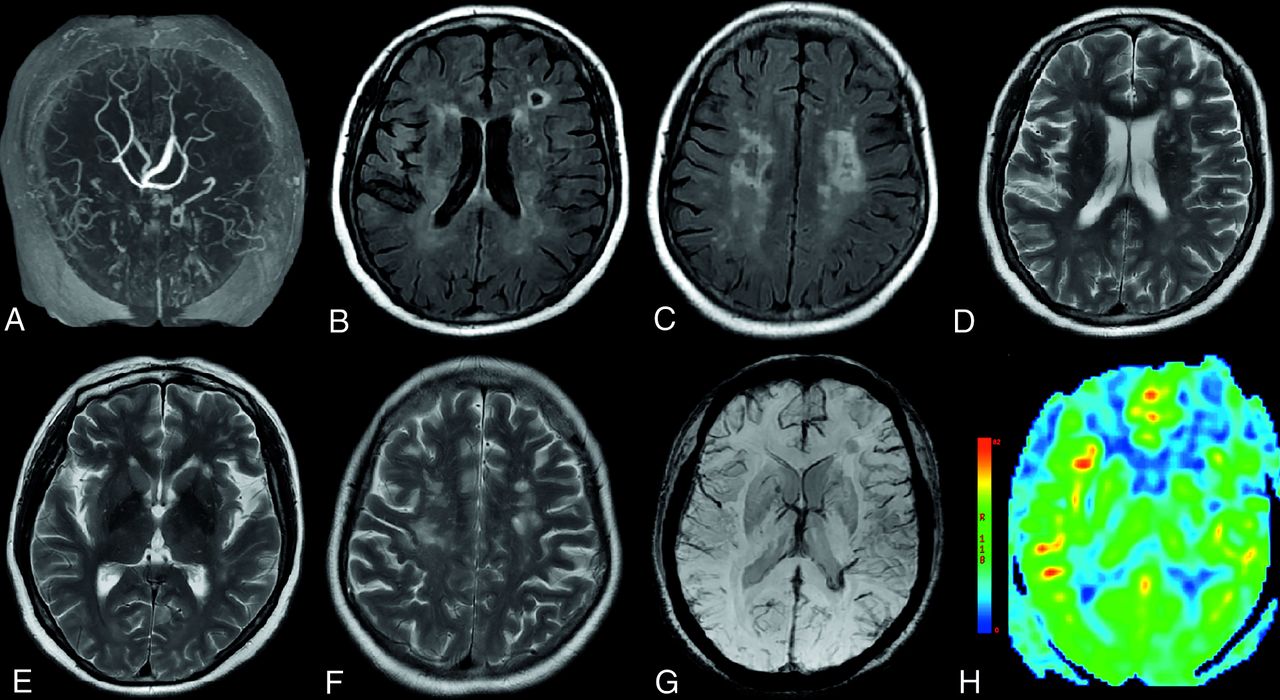
An illustrative case of a 46-year-old man with bilateral Moyamoya disease who presented with weakness of the right limb for 1 year. The modified brain frailty score was 2 for the left and 1 for the right hemisphere. MRA showed occlusion of the bilateral ICA (A). The periventricular and deep WMH was grade II for both sides on FLAIR images (B and C). Vascular lesions were found in the left frontal lobe on T2-weighted image (D). The EPVS in the basal ganglia was grade II for both sides on T2-weighted images (E and F). No microbleed was found on SWI (G). Both hemispheres showed perfusions deficits on CBF map (H).

DSA of the Matsushima grade I (A), grade II (B), and grade III (C). Grade I indicates revascularization of less than one-third of the MCA distribution, grade II represents revascularization of one-third to two-thirds of the MCA distribution, and grade III indicates revascularization of more than two-thirds of the MCA distribution.

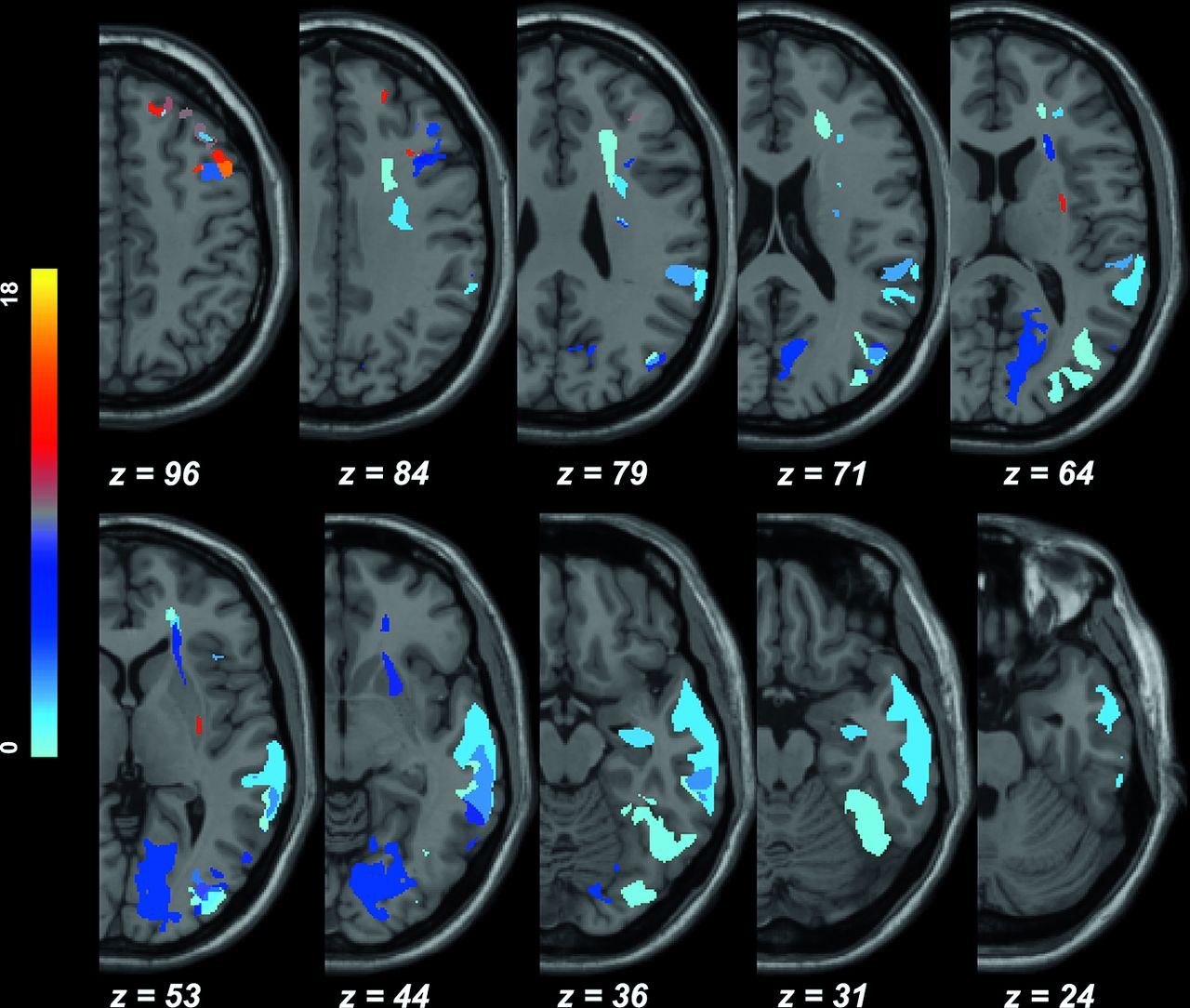
Lesion map (n = 18). Most large lesions were located at the frontotemporal and temporo-occipital watershed areas. Z refers to the section location, and a voxel with a brighter color indicates a larger number of hemispheres involved that lesioned voxel.
Correlations of the Modified Brain Frailty Score and Cerebral Perfusion
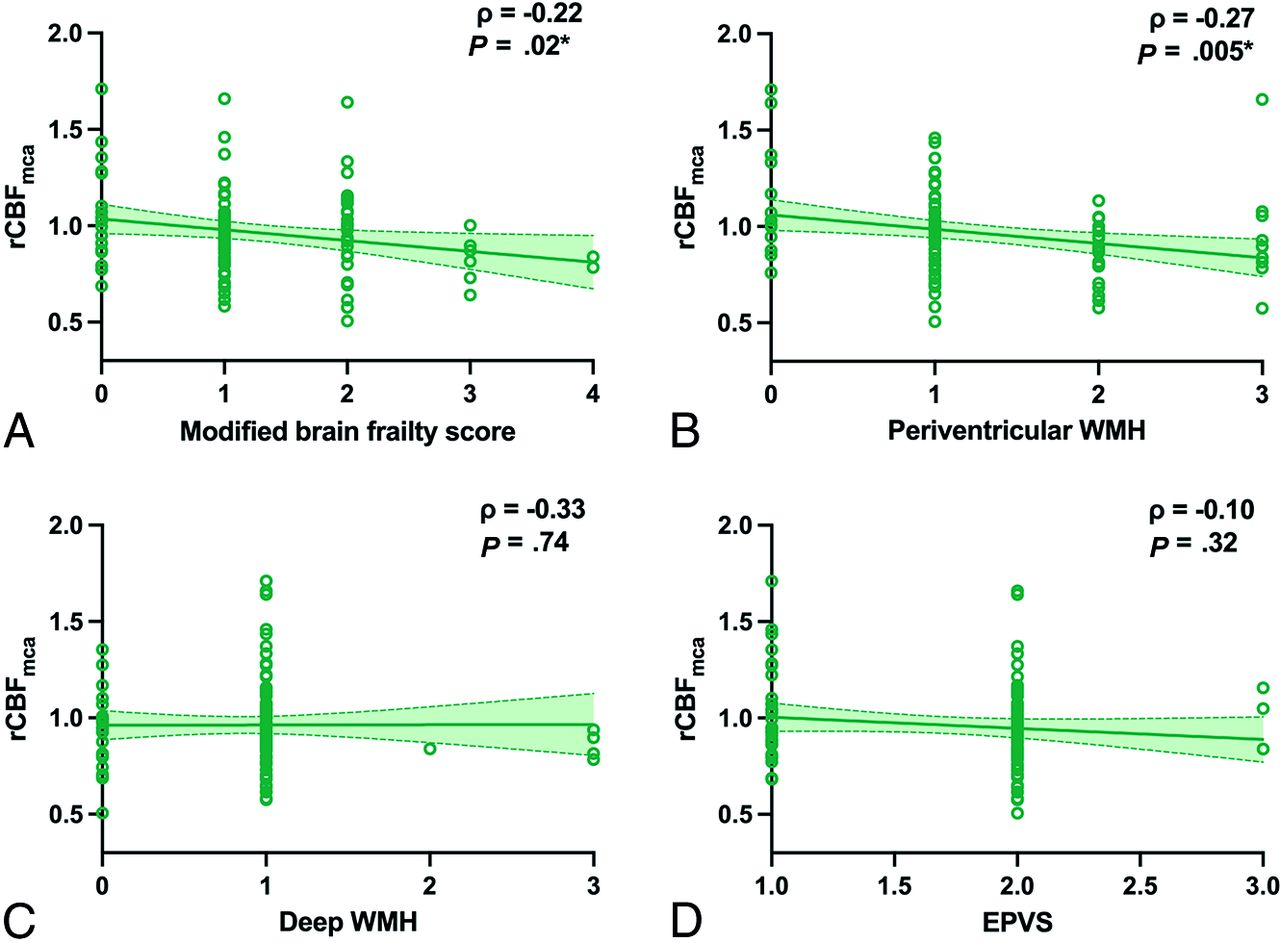
Results of correlations among the modified brain frailty score, WMH, and EPVS with cerebral perfusion are shown in Fig 5. There were significant correlations between the modified brain frailty score (ρ = −0.22, P = .02) and periventricular WMH with rCBFmca (ρ = −0.27, P = .005). No significant differences were found between hemispheres with and without CMB (t = 0.75, P = .46), as well as vascular lesions (t = 1.55, P = .12).

Scatterplots of the correlations between rCBFmca and the modified brain frailty score (A), periventricular WMH (B), deep WMH (C), and EPVS (D) (n = 107).
Differentiation of Stroke from Nonstroke MMD
There were 58 (54%) hemispheres in the stroke MMD group and 49 (46%) hemispheres in the nonstroke MMD group. The modified brain frailty score, sex, PCA involvement, and dyslipidemia met the threshold for multivariate logistic regression. Logistic regression analysis revealed that the modified brain frailty score and PCA involvement could differentiate stroke MMD from nonstroke MMD (OR = 2.00, P = .02; OR = 5.52, P = .02). The results are presented in Table 1. As for the separate features of brain frailty, periventricular WMH (χ2 = 14.45, P = .002), deep WMH (χ2 = 8.27, P = .04), and vascular lesions showed significant differences (χ2 = 10.37, P = .001) between the 2 groups. EPVS (χ2 = 2.21, P = .33) and CMB (χ2 = 1.38, P = .24) could not differentiate stroke and nonstroke MMD.
Differentiation of stroke MMD from nonstroke MMD (n = 107)
Subgroup Analysis in Stroke and Nonstroke MMD
To better understand whether the presence of brain parenchyma damage would affect the relationship between the modified brain frailty score and cerebral perfusion, we performed subgroup analysis in stroke and nonstroke MMD.
In stroke MMD, there was significant correlation between the modified brain frailty score with rCBFmca (ρ = −0.28, P = .04). No significant correlations were found between periventricular WMH (ρ = −0.23, P = .09), deep WMH (ρ = −0.02, P = .91), and EPVS (ρ = −0.11, P = .42) with rCBFmca. No significant differences were found between hemispheres with and without CMB (t = 1.28, P = .20), as well as vascular lesions (t = 1.13, P = .26).
In nonstroke MMD, there was significant correlation between the periventricular WMH with rCBFmca (ρ = −0.29, P = .04). No significant correlations were found among the modified brain frailty score (ρ = −0.05, P = .74), deep WMH (ρ = −0.15, P = .31), and EPVS (ρ = −0.02, P = .89) with rCBFmca. No significant differences were found between hemispheres with and without CMB (t = −0.86, P = .40), as well as vascular lesions (t = 0.43, P = .67).
Prediction of Matsushima Grade
After EDAS surgery, 12 (27%) hemispheres showed favorable outcome (Matsushima grade III), and 32 (73%) showed poor outcome (Matsushima grades 0–II). The modified brain frailty score did not differ between the 2 groups (χ2 = 1.36, P = .71), similar to its component imaging findings of periventricular WMH, deep WMH, vascular lesions, and CMB (χ2 = 5.74, P = .12; Fisher Z = 2.74, P = .25; Fisher Z = 1.45, P = .49; Fisher Z = 0.54, P = .47). Nevertheless, basal ganglia EPVS showed a significant difference (Fisher Z = 12.20, P = .001). In addition, age, PCA involvement and a history of smoking also met the threshold for multivariate analysis. PCA involvement and basal ganglia EPVS could independently predict the postoperative Matsushima grade (OR = 0.56, P = .01; OR = 1.29, P = .03) (Table 2).
Prediction of postoperative Matsushima grade (n = 44)
DISCUSSION
In this study, we found that patients with MMD with a higher modified brain frailty score showed lower cerebral perfusion. Moreover, the modified brain frailty score was higher in patients with MMD with stroke. Although the frailty score showed no predictive value for postoperative revascularization, the basal ganglia EPVS was a promising indicator.
The correlation between the individual imaging components of brain frailty and perfusion in MMD has been reported by many studies. Sun et al18 found that lacunes, EPVS, and WMHs were associated with abnormal CBF in the cortex and basal ganglia. Komatsu et al19 found that WMH was reversible and CBF increased after revascularization surgery, indicating that the improvement in CBF was partially related to the improvement of the WMH. The current study found that the overall estimation of brain frailty could also reflect the hemodynamic status. However, the causal relationship between the frailty score and perfusion remained elusive, warranting further longitudinal studies. Furthermore, MR imaging perfusion techniques like pCASL or CTP are not available in some institutions, making the modified brain frailty score a useful indirect and practical marker of abnormal hemodynamics in MMD.
The relationship between imaging signs of brain frailty and CBF in atherosclerotic ischemic stroke has produced mixed results.20,21 One reason may be that stroke studies tend to include a large portion of elderly patients, who may have long-term coexisting metabolic abnormalities and lifestyle diversities that can influence the progression of brain frailty and the decline of cerebral perfusion. In contrast, patients with MMD usually present with symptoms at a younger age, with fewer confounding factors, making it an appropriate model for chronic hypoperfusion.
The decrease in cerebral perfusion was correlated with the increase of periventricular WMH grades, rather than deep WMH. A commonly accepted concept is that periventricular and deep WMH have different pathophysiologies, in that periventricular WMH is more relevant to perfusion abnormality, while deep WMH is more related to progressive demyelination.12,22,23 The association between cerebral perfusion and periventricular WMH was consistent with the established pathophysiology of MMD, which is characterized by a chronic perfusion deficit. Another possible explanation may be the anatomic location of periventricular WMH, which is primarily in the watershed region, making it more sensitive to chronic hypoperfusion and subsequent damage.24,25
Some patients with MMD could be asymptomatic and have nonspecific symptoms, such as headache or dizziness.9 Moreover, unlike ischemic or hemorrhagic strokes, many patients with MMD present with TIA with no apparent structural lesions.26 The main difference between patients with stroke and those with TIA or nonspecific symptoms is cerebral structural damage. In this study, it was found that patients with MMD with stroke had higher modified brain frailty scores compared with those without stroke symptoms. This result may be attributed to the shared underlying mechanism of brain frailty and stroke, which is cerebral hypoperfusion.27,28 Chronic hypoperfusion can lead to the development of brain frailty, and a failure of blood supply can ultimately result in stroke onset. From the group-level lesion map, most large lesions are located at the frontal, temporal, and occipital areas. Another evident feature of the lesion location was that large infarctions were mainly located in the cortical area compared with patients with conventional strokes due to arteriosclerosis diseases. This finding may, in part, be related to the selective vulnerability of the cortical gray matter to ischemia in patients with MMD, who may have experienced hypoperfusion since childhood.29
In the subgroup analysis, we found that the modified brain frailty score was correlated with rCBFmca in stroke MMD, while periventricular WMH was associated with rCBFmca in nonstroke MMD. This result may suggest that extra attention should be paid to periventricular WMH before brain parenchyma damage occurs. In addition, the overall estimation of brain frailty may be more helpful to reflect perfusion status in patients with MMD, who have already had ischemic or hemorrhagic stroke. We assumed that the reason behind this finding was the overall impact of periventricular WMH, deep WMH, and vascular lesions on brain structural changes, not periventricular WMH itself.
Brain frailty and its several imaging features could not predict surgical outcomes. However, basal ganglia EPVS showed a marginally significant correlation with postoperative revascularization. The perivascular space (PVS) runs parallel to perforating vessels. Former literature suggested that the PVS forms a network to help clearance of waste products and exchange of various signaling molecules between the CSF and interstitial fluid.30 Presumably, the enlargement of the PVS might impair the ability of this clearance pathway, which might damage the angiogenesis and arteriogenesis that take place in chronic ischemia. Similarly, abnormalities of EPVS could also affect angiogenesis after EDAS, leading to fewer newly formed transdural collaterals. However, the above hypothesis of EPVS still needs to be validated by future research that focuses on specific molecular mechanisms.
PCA involvement was also found to predict postoperative revascularization. The posterior circulation provides the main retrograde leptomeningeal collateral flow in MMD.31,32 In this study, we found that the modified brain frailty score, periventricular WMH, and deep WMH were different between hemispheres with and without PCA involvement. This finding may imply that compared with other frailty imaging features, WMH may be more sensitive to the blood supply insufficiency, mainly determined by the posterior circulation. Most interesting, results showed that patients with an intact PCA tend to have lower Matsushima grades. A possible explanation may be the change in the source of the blood supply after surgery. EDAS provides new blood supply from the external carotid artery system to compensate for the perfusion deficit of anterior circulation, which may conflict with preoperatively formed collaterals from the PCA. As a result, patients with well-established leptomeningeal collaterals before surgery might present with less favorable transdural revascularization on angiography. Further verification is needed through prospective studies with longer follow-ups.
Our study has several limitations. First, a drawback was the difficulty in adjusting arterial transit time using pCASL with a single post-labeling delay in MMD, in which slow collateral flows often occur. Perfusion studies of MMD could benefit from multidelay arterial spin-labeling in the future. Second, the difference in the correlation between brain frailty and perfusion in ischemic and hemorrhagic MMD was not assessed due to a limited number of patients with hemorrhagic MMD. Third, because of the limited number of hemispheres with postoperatively evaluated Matsushima grades (44 hemispheres), future studies with larger sample sizes are needed to estimate the relationship between brain frailty and surgical outcomes. Fourth, former studies suggested that individual imaging markers of brain frailty reflect intracerebral arteriole distensibility.33 Cerebrovascular reactivity may be a more sensitive measure of hemodynamic changes than CBF.
CONCLUSIONS
This study found a correlation between a higher modified brain frailty score with decreasing cerebral perfusion in MMD, suggesting the use of the modified brain frailty score as an indirect and comprehensive marker of hemodynamic abnormality. Additionally, patients with MMD with stroke symptoms showed more severe brain frailty. Finally, basal ganglia EPVS could be used to predict postoperative revascularization. The findings were considered credible to extend to other diseases with chronic cerebral hypoperfusion. Future studies should investigate the underlying mechanisms of brain frailty in MMD and validate the use of the modified brain frailty score in larger cohorts.
Footnotes
This work was supported by the National Natural Science Foundation of China (No. 82327803, No.81825012, No. 82151309 to X. Lou and No. 82271952 to J.H. Lyu).
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 7, 2023.
- Accepted after revision February 9, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.