
Abstract
BACKGROUND: Mechanical thrombectomy using a double stent retriever technique has recently been described for the treatment of acute ischemic stroke, but its efficacy and safety are not well-established.
PURPOSE: The aim of this systematic review and meta-analysis was to evaluate reports of the use of a double stent retriever technique during the endovascular treatment of patients with ischemic stroke.
DATA SOURCES: The PubMed, EMBASE, Web of Science, and Scopus databases were searched to identify all studies (clinical trials, cohort series, and case reports) investigating the utility of a double stent retriever technique for the treatment of stroke. The study is reported in accordance with PRISMA 2020 guidelines and was prospectively registered in PROSPERO (CRD42023482691).
STUDY SELECTION: Seventeen studies involving a total of 128 patients with large-vessel occlusions predominantly in the anterior circulation (93.0%) were identified.
DATA ANALYSIS: Outcomes of interest were the prevalence of successful recanalization (modified TICI ≥2b) and a first-pass effect following the double stent retriever technique as well as complications such as iatrogenic dissections and SAH. Data were pooled using a random effects model.
DATA SYNTHESIS: The double stent retriever technique was used as a rescue strategy in occlusions refractory to conventional endovascular treatment in 68.7% (88/128) of patients and as a first-line strategy in 31.3% (40/128) of patients. The double stent retriever technique achieved an overall final modified TICI ≥2b in 92.6% cases, with a first-pass effect of 76.6%. The complication rate remained low, with 0.37% dissection and 1.56% SAH.
LIMITATIONS: Limitations of the study include the following: 1) a large number of case reports or small series, 2) a meta-analysis of proportions with no statistical comparison with a control group, and 3) the lack of access to patient-level data.
CONCLUSIONS: Our findings suggest that double stent retriever thrombectomy may be safe and associated with good recanalization outcomes, but prospective comparative studies are needed to determine which patients may benefit from this endovascular procedure.
ABBREVIATIONS:
- AICH
- asymptomatic intracranial hemorrhage
- AIS
- acute ischemic stroke
- DSR
- double stent retriever
- FPE
- first-pass effect
- MT
- mechanical thrombectomy
- mTICI
- modified TICI
- NOS
- Newcastle-Ottawa Scale
- SICH
- symptomatic intracranial hemorrhage
- SR
- stent retriever
- SSR
- single stent retriever
Mechanical thrombectomy (MT) using a double stent retriever (DSR) approach has been recently reported as a highly effective endovascular treatment for patients with acute ischemic stroke (AIS).1⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓-17 DSR MT was first introduced as a rescue technique when conventional single stent retriever (SSR) treatment failed.1⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓-14,16 More recently, it has been used as a first-line treatment for large intracranial vessel occlusion.17 However, there is no systematic review and meta-analysis of clinical cases treated with this approach, limiting the evaluation of its overall efficacy and safety. Our systematic review and meta-analysis aimed to evaluate articles reporting the use of DSR during endovascular treatment of patients with AIS to better assess the efficacy and safety of this endovascular approach.
MATERIALS AND METHODS
Search Strategy
The Cochrane Handbook for Systematic Reviews of Interventions (https://training.cochrane.org/handbook) and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA, http://www.prisma-statement.org/) guidelines were followed. The study protocol was prospectively registered in PROSPERO (CRD42023482691). Four online databases (PubMed, EMBASE, Web of Science, and Scopus) were searched using filters for English language articles published from their inception to October 31, 2023. Medical subject headings and keyword searches included the terms “brain” OR “cerebral” AND “stroke” AND “thrombectomy” OR “endovascular” AND “double stent” OR “y-stent.” To identify missing articles, we also conducted an extensive manual search of the reference lists of included articles, and pertinent available nonsystematic analyses were reviewed for other potential citations. Data from unpublished sources were not searched or included.
Screening Process and Eligibility Criteria
Two investigators (J.H. and O.B.) performed the title and abstract selection, followed by a full-text selection phase including the studies remaining after the initial selection. In case of disagreement, a third investigator (P.M.) was consulted to reach a consensus. We included all original studies that met our criteria for population (patients with AIS), exposure (DSR MT), comparator (none), and outcome. The primary end point was successful intracranial recanalization at the end of MT, defined by a modified TICI (mTICI) score ≥2b, recanalization rate (mTICI score ≥2b) at the first pass of DSR (first-pass effect [FPE]), arterial dissections during DSR MT, rate of SAH at the end of the procedure, asymptomatic intracerebral hemorrhage (AICH), and symptomatic intracerebral hemorrhage (SICH) on control imaging 24–48 hours after the procedure, as defined by the European Cooperative Acute Stroke Study (ECASS) criteria.18 We were unable to include embolization to a new territory as a primary end point in our analysis because it was not reported in the studies reviewed, though it is an important outcome of MT and could represent a publication bias. We excluded studies evaluating DSR in vitro and conference abstracts. We had no restrictions on patient characteristics or stroke location.
We assessed the evidence of the nonrandomized studies included using the Newcastle-Ottawa Scale (NOS)19 to provide a quality assessment in the interpretation of meta-analysis results. Two investigators (J.H. and O.B.) rated the NOS for each study. In case of disagreement, a third investigator (P.M.) was consulted to reach a consensus.
Data Extraction
Data extracted included study characteristics, baseline demographic and clinical characteristics of patients treated by DSR, and outcomes of interest. Two authors (J.H. and O.B.) independently performed the data extraction, which was then reviewed by a third author (P.M.) for consensus.
Statistical Analysis
We pooled frequencies and means with corresponding 95% CIs. Generalized linear mixed models with logit transformation and random effects were used to pool data due to the relatively small sample sizes, the presence of zero events, and methodologic differences among studies.20,21 Heterogeneity was assessed using the Q statistic and the I2 test, in which P < .05 (2-tailed) or I2 values >50% were considered significant; similar to Kobeissi et al,22 funnel plots were used for the visualization of publication bias. We first analyzed all published articles and then repeated the same analyses only for consecutive cohorts with >5 patients. All data were analyzed using R, Version 4.2.2 (http://www.r-project.org/) and the meta package.
RESULTS
Search and Screening Results
The initial research resulted in 424 articles, of which 237 came from the PubMed search, 121 from EMBASE, and 66 from Scopus. After removing 178 duplicates, we retained 246 articles for further selection. We excluded a further 228 articles at the title- and abstract-selection stage, resulting in 18 articles for full-text review. One article was removed because the authors used a Merci device and not a stent retriever,23 leaving 17 articles that met our inclusion criteria with appropriate reporting of the outcomes of interest and comprising 128 patients treated by MT using a DSR technique. The results of our literature screening are summarized in the Online Supplemental Data.
Study Characteristics
Of the 17 articles published between 2009 and 2023, eleven were case reports with 1 or 2 patients only1⇓⇓⇓⇓⇓⇓⇓⇓⇓-11 and 6 were consecutive case series with 9–39 patients.12⇓⇓⇓⇓-17 Patient characteristics, including age, sex, initial NIHSS, and use of IV thrombolytics, are detailed in the Online Supplemental Data. Patients enrolled had predominantly anterior circulation occlusions (n = 119 [93.0%]) involving in the ICA (n = 59) and/or MCA (n = 76). Nine patients had posterior circulation occlusions (7.0%) involving in the basilar artery.
Procedure Characteristics
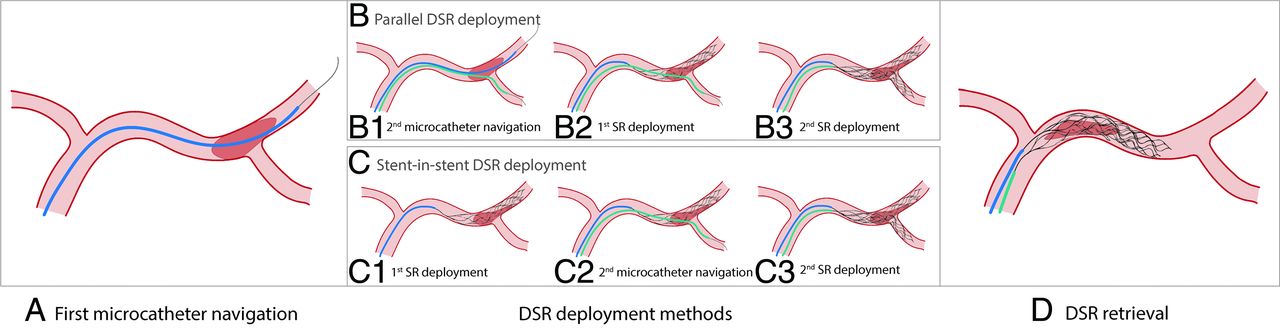
Forty MTs with DSR were performed as first-line treatment (31.3%), and 88, as rescue treatment (68.7%). One hundred thirteen (88.3%) MTs with DSR were performed with parallel stent deployment, in which 2 microcatheters were placed in branches distal to the clot before stent deployment. Fifteen (11.7%) MTs were performed using a stent-in-stent deployment technique, in which a first microcatheter is advanced distal to the clot and a stent retriever (SR) is deployed through it, followed by navigation of a second microcatheter through this first SR to allow deployment of the second SR. Details of the 2 stent-deployment techniques and practical tips found in the literature are shown in Fig 1.

Illustration of the parallel and stent-in-stent DSR techniques. A, Navigation of the first microcatheter over a microwire distal to the clot (step common to both DSR techniques), as in conventional thrombectomy using an SSR. Deployment of the stent retrievers (3 different steps between the parallel and stent-in-stent DSR techniques). B, In the parallel DSR technique, B1, A second microcatheter is navigated distal to the clot on a microwire, ideally in an arterial branch different from the first microcatheter. B2, The first SR is deployed distally and through the clot. As with the MT SSR, the clot should be in the proximal part of the SR. B3, The second SR is deployed, ideally with the clot also in the proximal part of the SR. C, In the stent-in-stent technique, C1, The first SR is deployed distally and through the clot, ideally with a clot in the proximal part of the SR. C2, A second microcatheter is navigated distal to the clot over a microwire through the mesh of the first stent, ideally into an arterial branch different from the one used for the first microcatheter. C3, The second SR is deployed, ideally with the clot also in the proximal part of the SR. D, Removal of the 2 SRs together (common to both DSR techniques). Both SRs are removed at the same time and at the same slow speed. To ensure that the removal of both SRs begins at the same time, it is important to tension both stents before retrieval. It may also be useful to place a single torque on the pushwires of both stents once they have been tensioned, to remove the stents at an identical and harmonious speed.
Quality of Evidence
The quality of the evidence from the studies included in our systematic review and meta-analysis evaluated using the NOS was poor, relying on many case reports (Online Supplemental Data). This issue could raise concerns about publication bias in studies evaluating the use of the DSR. Therefore, in addition to the analysis of all included articles, we repeated the meta-analysis by including only larger consecutive cohorts (6 cohorts, 116 patients in total) of patients treated with DSR.
DSR Efficacy
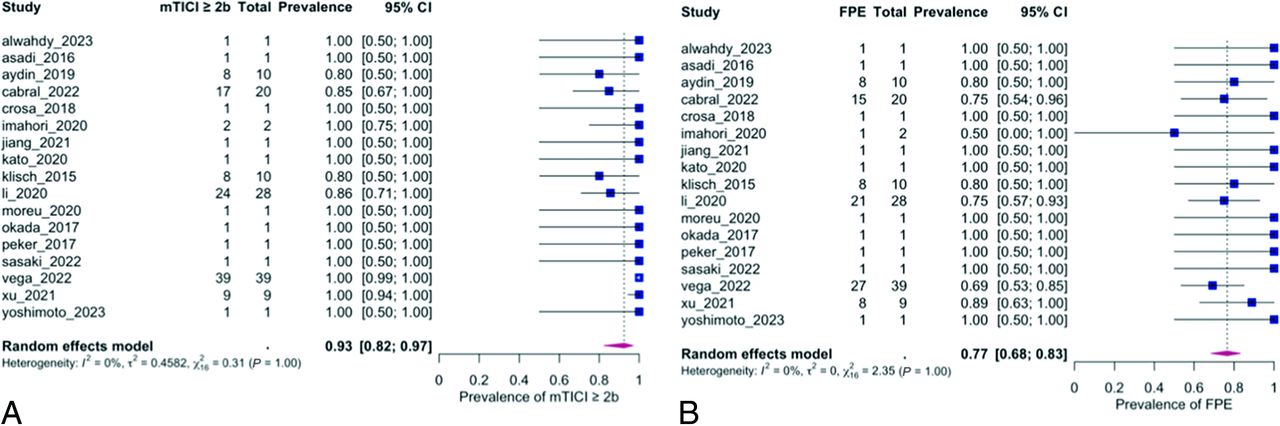
The meta-analysis of all studies showed a high rate of successful recanalization (mTICI ≥2b) at the end of MT with a DSR, with a prevalence of 92.6% (95% CI, 82.4%–97.0%) (Fig 2A and Table). When combined, these studies also reported an FPE (at the first pass of DSR) of 76.6% (95% CI, 68.5%–83.1%) (Fig 2B and Table). There was no heterogeneity among the pooled studies for the final successful recanalization (mTICI ≥2b) (I2 = 26.4%, P = 1.0) or for FPE (I2 = 0%, P = 1.0) (Table).

Efficacy of DSR MT. A, Successful recanalization (mTICI ≥ 2b). B, FPE.
| Prevalence (95% CI) | Heterogeneity I2 | Wld (P Value) | |
|---|---|---|---|
| Estimated prevalence for all studies (n = 17) | |||
| FPE | 76.56% [68.46–83.10] | 0% | 2.35 (P = 1.0) |
| mTICI ≥ 2b | 92.60% [82.43–97.01] | 26.42% | 0.31 (P = 1.0) |
| Dissection | 0.37% [0–44.50] | 65.90% | 0.0 (P = 1.0) |
| SAH | 1.56% [0.39–6.03] | 0% | 0.97 (P = 1.0) |
| AICH | 8.05% [3.14–19.14] | 33.58% | 0.55 (P = 1.0) |
| SICH | 5.47% [2.63–11.03] | 0% | 0.86 (P = 1.0) |
| Estimated prevalence for large studies only (n= 6) | |||
| FPE | 75.0% [66.34–82.04] | 0% | 1.79 (P = .877) |
| mTICI ≥ 2b | 91.05% [80.04–96.27] | 44.39% | 0.31 (P = .998) |
| Dissection | 0.42% [0–58.34] | 75.96% | 0.0 (P = 1.0) |
| SAH | 1.72% [0.43–6.63] | 0% | 0.97 (P = .965) |
| AICH | 8.37% [3.13–20.55] | 50.0% | 0.55 (P = .990) |
| SICH | 6.03% [2.90–12.12] | 0% | 0.85 (P = .973) |
Note:—Wld indicates Wald-type test statistic of the test for (residual) heterogeneity.
Estimated prevalence of successful recanalization (mTICI ≥2b) and FPE following DSR, as well as complications due to dissection, SAH, AICH, and SICH
In the subanalysis including only the larger consecutive cohorts, the mTICI score 2b–3 had a frequency of 91.1% (95% CI, 80.0%–96.3%) and a FPE of 75.0% (95% 66.3%–82.0%) (Table and Fig 3). Although still moderate, study heterogeneity is higher for mTICI (I2 = 44.4%; P = .998), while it remained very low for FPE (I2 = 0%, P = .887). Funnel plots for these efficacy indicators are shown in the Online Supplemental Data.

Efficacy of DSR MT in large cohorts only (n = 6): A, Successful recanalization (mTICI ≥ 2b). B, FPE.
DSR Safety
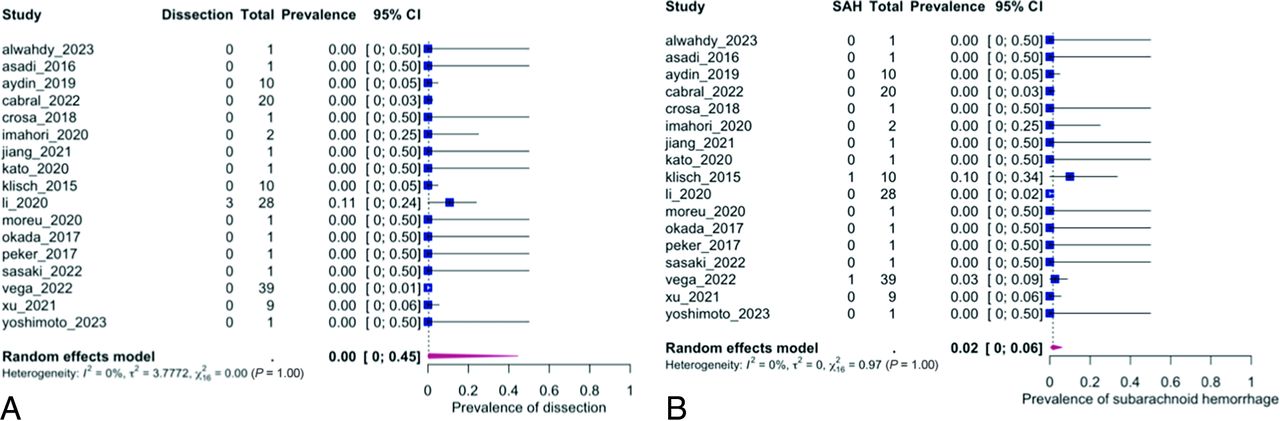
The pooled analysis of all studies showed a low rate of dissection with the use of DSRs, estimated at 0.4% (95% CI, 0%–44.5%) (Fig 4A and Table), but with heterogeneity among studies (I2 = 65.9%, P = 1.0). SAH rates also remained low at an estimated 1.6% (95% CI, 0.4%–6.0%) (Fig 4B), with no heterogeneity in the data (I2 = 0%, P = 1.0). Finally, AICH and SICH rates were also low, with an estimated 8.1% (95% CI, 3.1%–19.1%) and 5.5% (95% CI 2.6%–11.0%), respectively (Fig 5). However, study heterogeneity was greater for AICH (I2 = 33.6%, P = 1.0) than for SICH (I2 = 0%, P = 1.0) (Table). These results for the frequencies of dissection, SAH, AICH, and SICH are very similar in the subanalysis of large consecutive cohorts only, though with greater heterogeneity for dissection and AICH (Table and Fig 6). Funnel plots for these safety variables are shown in the Online Supplemental Data.

Safety of DSR MT dissections (A) and SAH (B).

Symptomatic and asymptomatic intracranial hemorrhage. A, AICH in all studies. B, SICH in all studies. C, AICH in large cohorts only. D, SICH in large cohorts only. ICH indicates intracranial hemorrhage.

Safety of DSR MT in large-cohort studies only (n = 6): dissections (A) and SAH (B).
DISCUSSION
This systematic review and meta-analysis synthesized cohorts and clinical cases of patients treated with a DSR MT technique reported in the literature, including 128 patients with large intracranial vessel occlusion predominantly in the anterior circulation (93.0%). The results suggest that MT using a DSR technique may be safe and associated with high efficacy.
DSR Efficacy
Successful recanalization (mTICI ≥ 2b) was achieved in 92.6% of cases, which is close to that reported in recent clinical trials of MT with SSR.24 DSR was used as a rescue strategy in 88 cases (68.7%) and as a first-line treatment in the remaining 40 cases (31.3%). Considering that 68.7% of these DSR MTs were performed as a rescue strategy in occlusions refractory to conventional endovascular treatment with SSR, the efficacy of DSR MT appears very high. Furthermore, the FPE rate when using a DSR was 76.6%, which is very high compared with the recent literature. Indeed, recent cohort articles or post hoc analyses of clinical trials report FPE rates between 22.8% and 31%,25⇓-27 and a recent meta-analysis found an FPE rate of 40.3% with conventional MT.28 Therefore, DSR MT may be a promising strategy in the therapeutic armamentarium for the endovascular treatment of AIS in occlusions that are difficult to treat with SSR, but it may also be an interesting first-line strategy in selected situations.
DSR Safety
One concern with the use of DSR is the potential increased complication rate due to the addition of a second SR, which may exert greater force during clot retrieval. In our meta-analysis, the rate of dissection, SAH, and intracranial hemorrhage (AICH and SICH) with DSR is comparable with the rates in the recent literature using conventional types of MT.29,30 The estimated rates of dissection and SAH in our meta-analysis were 0.4% and 1.6%, respectively. However, the heterogeneity of the data was significant for dissection (I2 of 65.9%). In addition, the use of long- and large-diameter SRs was associated with a higher complication rate in 1 clinical cohort included in our meta-analysis.14 The rate of intracranial hemorrhage on follow-up imaging was also comparable with that reported in the literature, with an estimated 8.1% of AICH and 5.5% of SICH. The fear of a higher rate of complications with the use of a DSR MT, therefore, would appear to be eased by our meta-analysis, which found complication rates similar to those reported in the recent literature.
DSR Mechanism of Action
Although in vitro studies were excluded from our meta-analysis because they did not directly involve patients treated for AIS, they may provide insight into the mechanism of action underlying the efficacy of DSR. Indeed, only in vitro studies performed under videographic guidance allow visualization of the interaction between the clot and the SRs during the MT maneuver. Two recent in vitro studies have investigated the efficacy of DSR and confirmed a higher rate of recanalization and a reduction in distal emboli compared with MT by SSR.31,32 Analysis of MT by DSR in these studies provides a better understanding of the mechanisms underlying the improved efficacy of DSR. First, the surface area for interaction between the SR and the clot is increased due to the addition of a second stent, creating a wider “fishing net” effect that ensures a lower risk of clot fragmentation during retrieval. Second, the mechanism of clot capture by the DSR appears to be different from that of an SSR due to a “pincer effect,” which traps the clot between the 2 SRs. Thus, whereas SSRs integrate into soft clots and drag hard clots in a rolling phenomenon, the addition of a second SR modifies the clot-capture mechanism in 2 ways (i.e., a wider fishing net and a pincer effect), irrespective of clot consistency. Finally, in bifurcation occlusions (e.g., M1–M2), where the exact location of the clot is uncertain, targeting 2 different branches increases the likelihood that the SR will completely cover the thrombus. Thus, although targeting the correct or incorrect M2 branch using SSR remains a probabilistic concept, using DSR could reduce the occurrence of partial clot coverage. One of the 2 in vitro studies also reported a higher clot-retraction force with DSR than with SSR using 2 open-cell SRs.32 However, the retrieval force remained within the range observed with other stent types and designs (open and closed cell). This finding suggests that the choice of 2 SRs may have an impact on MT safety.
Limitations
Our meta-analysis has some major limitations. First, the quality of evidence is poor and relies on many case reports or small series. While the case series and reports show that this approach is certainly feasible and potentially very useful in certain circumstances, the numbers of patient in most articles is small, and there is a potential publication bias. Indeed, only one-third of included articles were medium-sized consecutive case series. However, a subanalysis of these consecutive case series showed results close to those obtained by analyzing all articles in our meta-analysis. Second, our meta-analysis did not have a comparison group that was treated with SSR because none of the studies included such a group. Third, we were unable to access patient-level data for all studies included, limiting the analyses we could perform. In addition, there are no core laboratory adjudication of the results and no external validation of the reported results. Fourth, the technical approaches to MT are not standardized, both in terms of how a conventional thrombectomy failure is considered (number of passes, devices used, intracranial stent placement, or other rescue techniques, and so forth) and in terms of how the DSR is used.
Finally, there are other rescue options that can be considered when first-line thrombectomy fails. Furthermore, the cost-effectiveness of DSR as a first-line or rescue option has not been reported in the literature. We, therefore, support the recommendation of a multicenter randomized clinical trial (e.g., NCT05632458) to compare DSR with conventional approaches in terms of safety, efficacy, and cost-effectiveness.
CONCLUSIONS
In this meta-analysis of retrospective clinical data from 128 patients treated by MT using DSR, we observed an excellent FPE (76.6%) and successful final recanalization rates (92.6%). In addition, we observed a low complication rate similar to that reported in the literature using conventional endovascular techniques. Future prospective and comparative studies and subsequent patient-level meta-analyses should be conducted to further evaluate the use of DSR as an established strategy for the endovascular treatment of AIS.
Footnotes
This work has been supported by the Swiss National Science Foundation grant no 320030_188942 2.
The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received December 29, 2023.
- Accepted after revision March 20, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}