
Abstract
Summary: We report a case of iatrogenic aneurysm rupture during coil embolization in a 55-year-old woman. Surgical intervention resulted in a good clinical outcome. To our knowledge, this technique for the salvage of catheter-induced aneurysm perforation has not been previously reported.
Aneurysm rupture during coil embolization has been reported to occur in approximately 2–3% of cases (1–3). The clinical consequences of iatrogenic aneurysm perforations are often severe, with mortality rates approaching 50% (3). We report a case in which surgical intervention after microcatheter perforation resulted in a good clinical outcome, with the purpose of describing a technique for the salvage of catheter-induced aneurysm perforation, which, to our knowledge, has not been reported.
Case Report
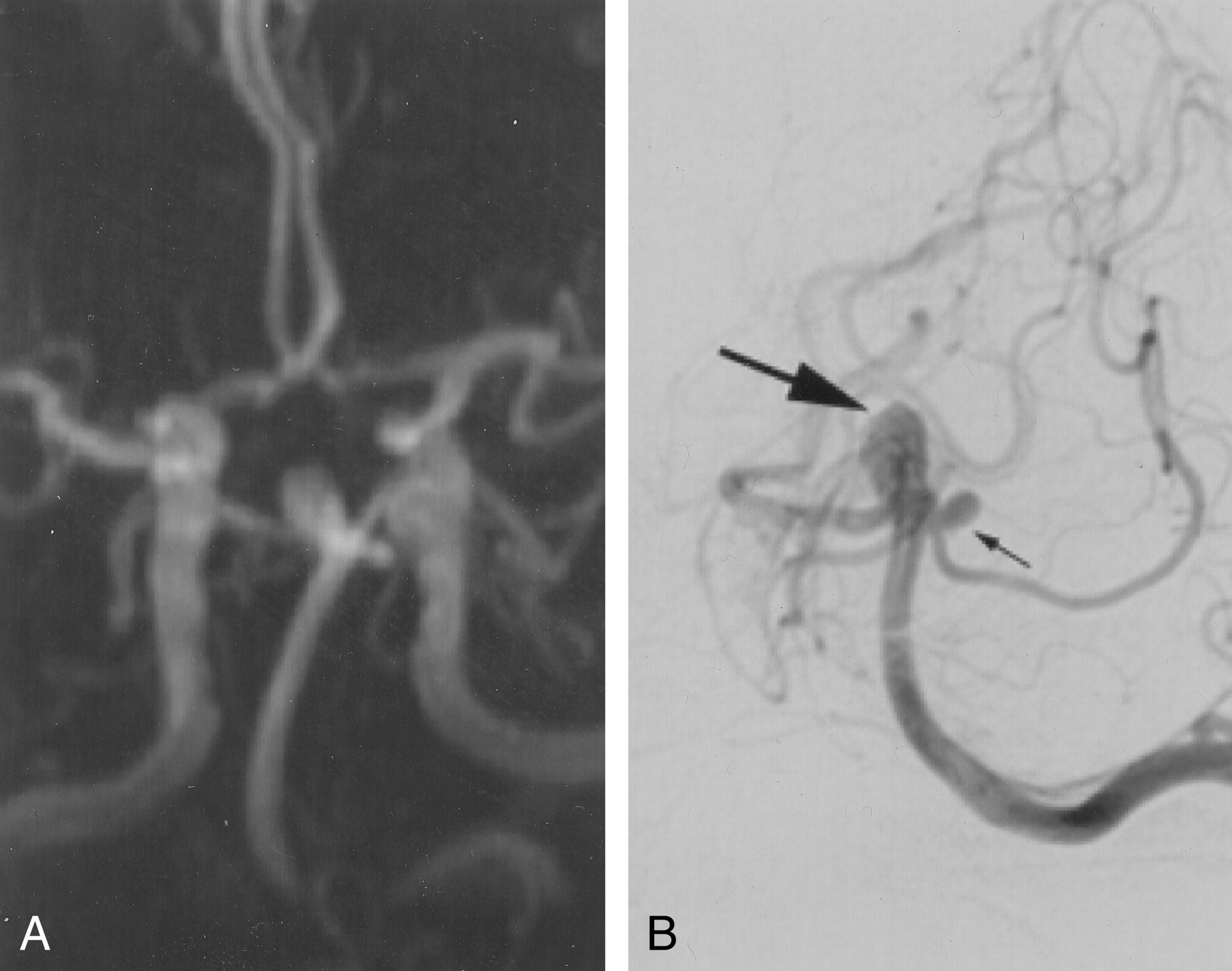
A 55-year-old woman was referred for MR imaging as part of a workup for worsening headaches. Images showed an 8 × 6-mm basilar tip aneurysm and a left superior cerebellar artery aneurysm measuring 3 × 4 mm (Fig 1A). No evidence of subarachnoid hemorrhage was present. The aneurysms were further evaluated with catheter angiography (Fig 1B).

Angiograms obtained in a 55-year-old woman with worsening headaches.
A, Three-dimensional time-of-flight MR angiogram demonstrates an aneurysm in the basilar tip that measures approximately 8 × 6 mm.
B, Conventional digital subtraction angiogram obtained with a left vertebral artery injection better shows how the left superior cerebellar artery originates from the aneurysm neck.
The patient underwent surgical exploration during which the basilar tip aneurysm was treated with a clip. At surgery, the smaller aneurysm arising from the base of the superior cerebellar artery was noted to have an area of weakness in the wall that required treatment. However, clips were not placed because a perforating vessel from the basilar artery was adherent to the aneurysm dome and could not be safely dissected from the dome.
The patient’s postoperative course was uneventful except for an incomplete third nerve palsy. Four days after surgery, the patient was referred for coil embolization of the superior cerebellar artery aneurysm. A 6F Envoy guiding catheter (Cordis, Miami, FL) was used to select the left vertebral artery. An Excel 14 microcatheter (Target Therapeutics, Fremont, CA) was advanced over a Fastdasher 14 microguidewire (Target Therapeutics) into the basilar artery. Wire access into the superior cerebellar artery aneurysm was easily achieved; achieving catheter access was challenging because of the following reasons: 1) difficulty in profiling the aneurysm neck caused by the overlying clip at the base of the basilar tip, 2) substantial tortuosity in proximal vessels, and 3) a turn of more than 90° approaching the aneurysm. Once the microcatheter was in the expected location of the aneurysm, gentle injection demonstrated extravasation into the subarachnoid space (Fig 2). Immediate injection through the guiding catheter in the left vertebral artery revealed no extravasation of contrast agent; this result indicated that the microcatheter sealed the hole in the aneurysm (Fig 3). The microcatheter appeared to egress through the artery at the junction of the aneurysm neck with the basilar artery. Because the perforation was in the aneurysm neck rather than in the dome, we were unsure that coil embolization of the aneurysm cavity could seal the hole effectively. Even so, we attempted to gain access into the aneurysm with a second microcatheter for Guglielmi detachable coil (GDC) placement. The contralateral femoral artery was punctured. A 5F Envoy guiding catheter was placed in the left subclavian artery. Microguidewire access into the aneurysm was again achieved. However, multiple attempts to navigate a second microcatheter into the aneurysm cavity were unsuccessful.

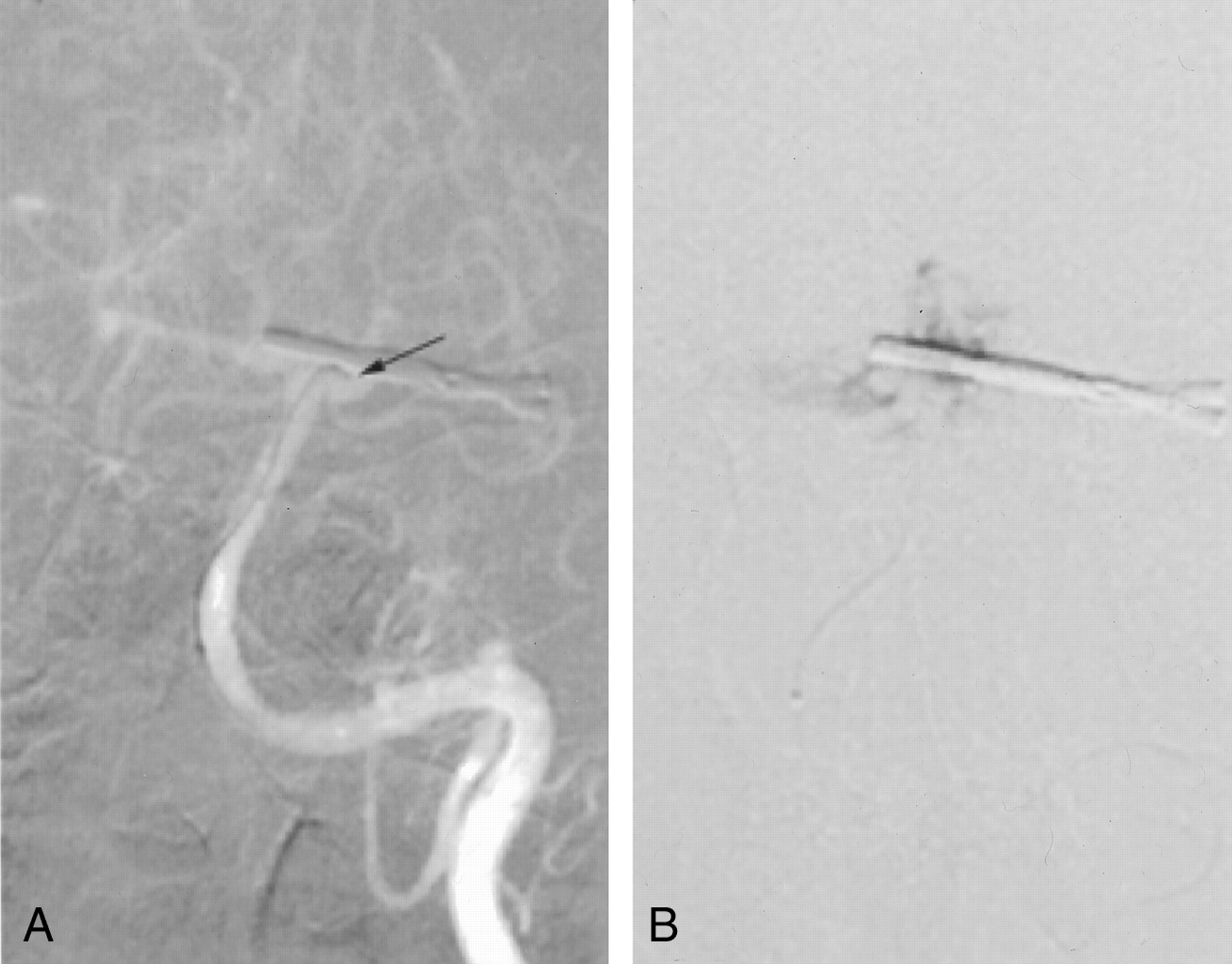
Roadmap images.
A, Anteroposterior (AP) oblique projection shows that, in this plane, the microcatheter tip (arrow) overlies the aneurysm.
B, However, gentle injection of the microcatheter in this location causes the contrast material to fill the subarachnoid space and not the aneurysm.

AP (left) and lateral (right) angiographic images obtained with an injection through the guiding catheter in the left vertebral artery demonstrate filling of the aneurysm with contrast material. No contrast agent extravasation is depicted; this result indicates that the microcatheter is sealing the hole in the aneurysm wall.
The catheter system, with continuous flushing in the guiding catheter, was secured to the patient, and the patient was moved to the operating room. A lumbar drain was placed with the patient in the lateral decubitus position without flexion of the head. The prior craniotomy site was then re-explored. After retraction of the temporal lobe, the superior cerebellar artery aneurysm was identified, with the microcatheter protruding through the aneurysm wall in proximity to the neck. No evidence of hemorrhage from the aneurysm was present. An aneurysm clip in the open position was placed across the neck of the aneurysm as the microcatheter was withdrawn. Brisk instantaneous hemorrhage was noted as the microcatheter was retracted through the perforation; the hemorrhage ceased upon closure of the clip (Fig 4). The clip covered the previously noted perforating vessel that was adherent to the aneurysm dome. Postoperative CT demonstrated no evidence of infarction or new hemorrhage. The patient recovered well and was discharged home 4 days later.

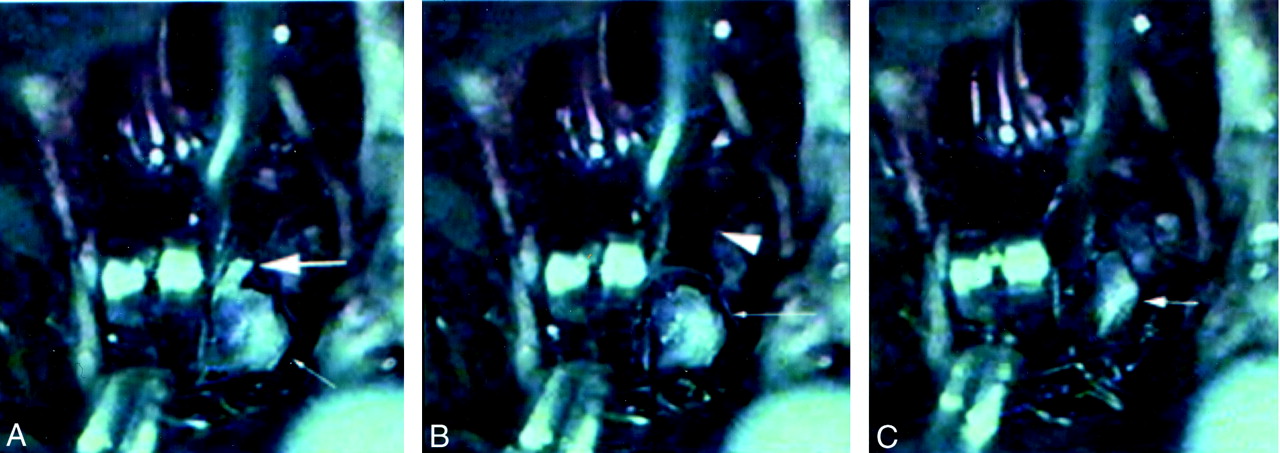
Sequence of pictures from an intraoperative videotape.
A, An aneurysm clip is held in the open position across the neck of the aneurysm (small arrow). The microcatheter protrudes through the aneurysm neck (large arrow).
B, The microcatheter is withdrawn from the aneurysm (arrow); this results in a brief spurt of hemorrhage from the hole in the aneurysm neck (arrowhead).
C, The aneurysm clip is released, with resultant decompression of the aneurysm (arrow).
Discussion
This case demonstrates a technique for the salvage of catheter-induced aneurysm perforation during coil embolization procedures, which, to our knowledge, had not been reported. We have shown that, even in the setting of a recent craniotomy for clip placement in an adjacent aneurysm, surgical rescue of iatrogenic aneurysm perforation is feasible. We demonstrated that the catheter remained in place during patient transfer, patient repositioning, and placement of a lumbar drain. The catheter and point of perforation could be directly visualized, and the aneurysm could be clipped as the microcatheter was removed with gentle traction.
Surgical intervention became necessary because access to the aneurysm with a second microcatheter could not be obtained. Surgical intervention may have been the preferred method of treatment in this case for two important reasons. First, the point of perforation was at the junction between the aneurysm neck and the basilar artery. This particular location, in our opinion, rendered success unlikely with the use of previously reported endovascular salvage techniques to seal the perforation (4). Most likely, coil embolization in the aneurysm dome would not have sealed the perforation at the aneurysm neck. The second important reason for surgical intervention is that the perforation was caused by a microcatheter rather than a microguidewire or coil. The resultant size of the rent in the artery is substantially larger with use of the former rather than with the latter. We thought that an unprotected catheter-induced perforation would be unlikely to seal spontaneously before devastating hemorrhage occurred.
Aneurysm perforation is a rare complication of GDC coiling, occurring in 2–3% of cases (1–3, 5). Guidewires, microcatheters, or coils may perforate aneurysms. Because microguidewires are extremely small (0.014 inch), perforation may result in a very small puncture in the aneurysm wall. This perforation may close before excessive hemorrhage occurs. Because microcatheters are larger and have a blunt tip, perforations caused by these may result in tearing of the aneurysm wall. Also, they are generally more severe. The overall mortality rate related to periprocedural aneurysm rupture is 25–50% (3, 5). Factors associated with aneurysm perforation are a small aneurysm size and recent aneurysm rupture (2, 3).
Endovascular strategies that have been advocated for the treatment of aneurysm perforation include immediate reversal of anticoagulation with protamine sulfate followed by rapid aneurysm packing with GDCs (2, 5, 6). Others have discussed potential endovascular salvage strategies with microcatheter perforation. Willinsky and terBrugge (4) reported a case in which the initial microcatheter perforated through the aneurysm wall. This microcatheter was left in place, and a second microcatheter was used to place the coil in the aneurysm. The initial microcatheter was withdrawn as a coil was deployed partially in the subarachnoid space and partially in the aneurysm. We attempted to use this strategy, but we were unable to gain access into the aneurysm with a second microcatheter.
Conclusion
This case demonstrates the use of a second salvage technique in microcatheter perforation. As in the case described by Willinsky and terBrugge, recognition of aneurysm perforation is imperative. If microcatheter perforation of the aneurysm had gone unnoticed, eventual repositioning of the microcatheter would have been likely. This repositioning would have resulted in substantial subarachnoid hemorrhage, with a high probability of patient mortality.
- Received March 1, 2001.
- Accepted after revision March 23, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}