
Abstract
Summary: The major technical drawback of percutaneous vertebroplasty is the potential for neural compromise from leakage of polymethylmethaorylate into epidural or perivertebral veins. We have combined the procedure of intrathecal injection of contrast medium with vertebroplasty to better delineate spinal canal encroachment during injection when the posterior vertebral wall is compromised by myeloma.
Percutaneous vertebroplasty has been implemented for the treatment of aggressive vertebral angiomas and malignant spinal tumors since 1984; metastases and myelomas are the most frequent of the malignant osteolytic lesions of the spine (1–4). The major technical drawback of percutaneous vertebroplasty is the potential for neural compromise from leakage of polymethylmethacrylate (PMMA) into epidural or perivertebral veins (5). When tumor extends to the posterior vertebral wall, an increased risk of neural compromise exists as a result of direct PMMA leakage or posterior displacement of the tumor mass into the spinal canal or neural foramina.We report on a case of percutaneous vertebroplasty for compression fracture secondary to myeloma. In this case, we found destruction of the posterior vertebral wall and injected contrast medium intrathecally to monitor posterior tumor displacement before significant canal encroachment occurred.
Case Description and Technique
A 70-year-old man was referred to our institution for evaluation because of severe, debilitating back pain after optimal medical treatment for multiple myeloma with spine involvement. Treatment had included radiation therapy; oral, injected, and transdermal narcotics; steroid therapy; bracing; and local analgesic injections. Workup revealed an increase in his compression fracture of L2, which revealed approximately 35% loss of height (Fig 1). Despite destruction of the posterior vertebral wall and pedicle on the left side, there was no clinical or radiographic evidence of neural compromise. A trial of percutaneous vertebroplasty with intrathecal contrast medium was planned to evaluate for posterior displacement of the soft tumor mass into the spinal canal during PMMA (Parallax Medical, Mountainview, CA) injection.

CT scan at L2 level. Note destruction of posterior vertebral wall and pedicle.
The patient was placed in prone position on the angiography table and prepared and draped in sterile fashion. An adequate plane of anesthesia was obtained by using injectable Fentanyl (Abbott Laboratories, Abbott Park, IL) and versed (Roche Laboratories, Nutley, NJ) and local injection of 1% Lidocaine (Abbott Laboratories, Chicago, IL). A 25-gauge spinal needle was placed at the L3 level, and 15 cc of Isovue M-200 (Bracco RX, Inc., Princeton, NJ) was injected via the intrathecal sac; visualization of the thecal sac and nerve roots was achieved (Fig 2). A small incision was made over the left L2 pedicle, and an 11-gauge bone trocar was advanced under fluoroscopic guidance into the L2 vertebral body. Under fluoroscopic observation, PMMA was slowly injected with a hand injector. After approximately 6 cc of PMMA was applied, the thecal sac showed signs of scalloping but no evidence of extension of PMMA to the posterior cortical margin (Fig 3). Despite lack of optimal filling of the vertebral body, we thought this evidence of thecal sac compression represented posterior displacement of the tumor mass, and no more PMMA was injected.

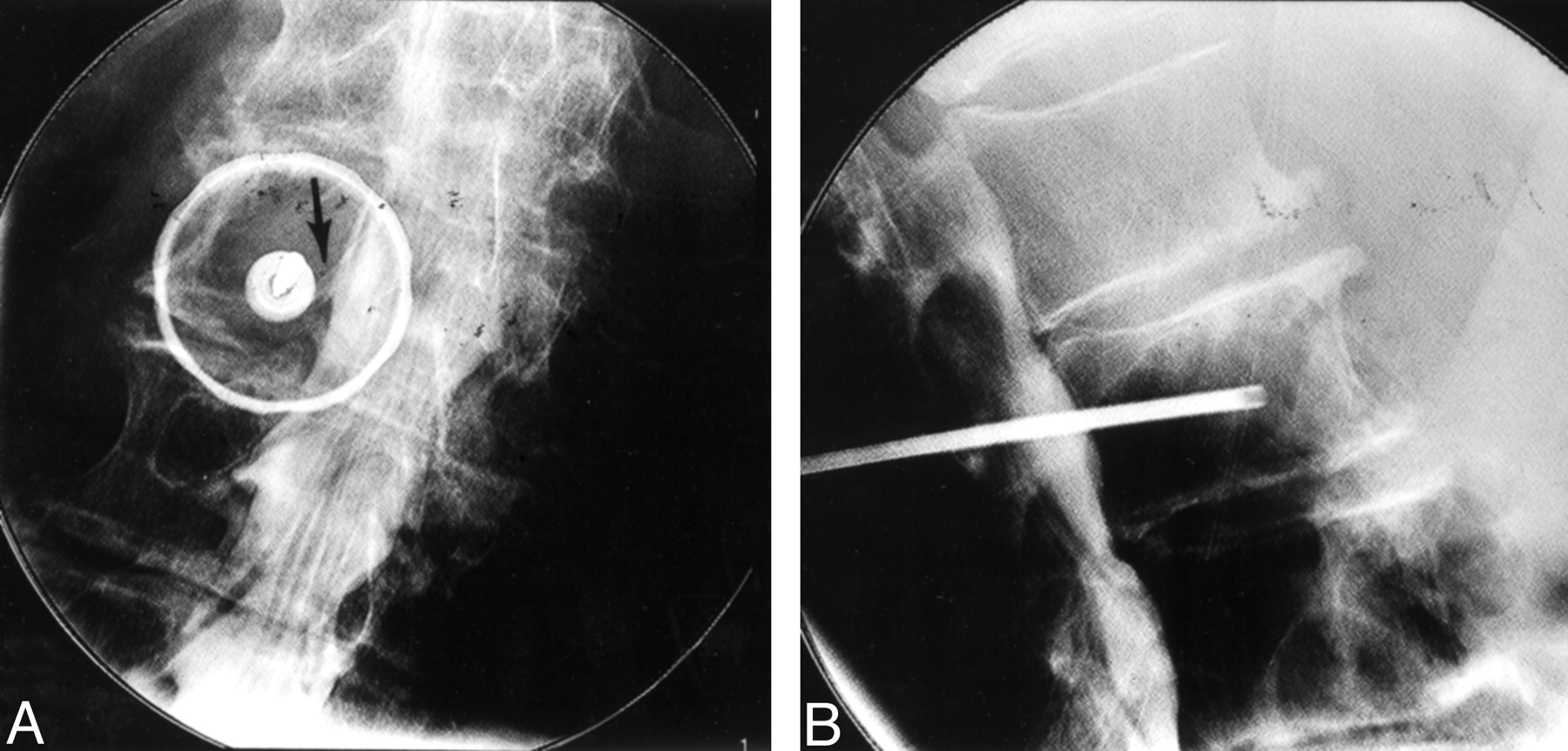
Fluoroscopic images of L2 after intrathecal injection of contrast material and placement of an 11-gauge trocar in the right pedicle.
A, Anteroposterior view. Contrast medium shows the proximity of the right nerve root sheath to the trocar and appropriate placement of the trocar.
B, Lateral view. Contrast medium shows minimal canal compromise by posterior tumor extension but no nerve root compromise.

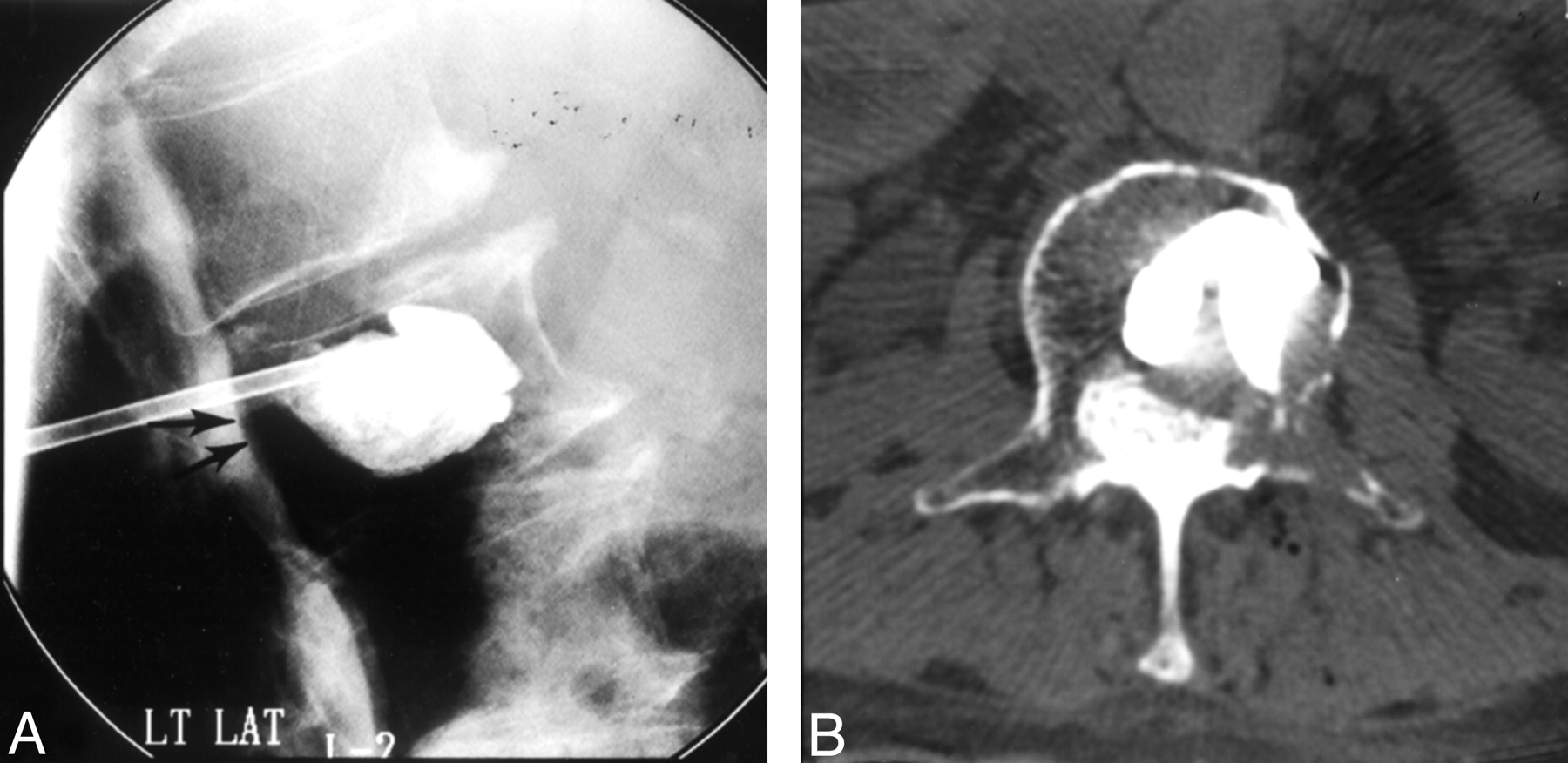
Fluoroscopic image at the L2 level after injection of PMMA (A) and CT scan at same level obtained after vertebroplasty (B).
A, Note subtle posterior displacement of thecal sac (arrows) and no extension of PMMA into the epidural venous plexus or posterior to vertebral margin.
B, Note the distance between the PMMA and posterior vertebral wall and the subsequent posterior epidural extension of the tumor that causes the scalloping visible in A.
The patient awoke from neuroleptic anesthesia without clinical evidence of neurologic compromise. Postoperative CT was performed and revealed posterior displacement of the tumor mass with encroachment on the thecal sac but no evidence of epidural extension of PMMA. The patient was discharged 2 hours after the procedure and reported notable reduction of back pain. He returned for follow-up 2 weeks later and reported a reduction of his back pain from a 10 on the visual assessment pain scale and scheduled narcotic use to a 3 with intermittent narcotic use. He had no evidence of neural compromise.
Discussion
The occurrence of neural compromise or epidural extension associated with percuatneous vertebroplasty varies and depends on the initial indications for vertebroplasty; however, in patients with spinal malignant tumors, the frequency is 10%. This compares with 2–5% of patients with vertebral angiomas and 1–3% of patients with osteoporotic lesions (1, 6–9). The increased risk is attributed to the destruction of vertebral cortex, which, according to Deramond and colleagues (2), occurs in more than 50% of patients. To date, there are few reports of spinal cord compression secondary to posterior displacement during vertebroplasty, but this likely represents a reluctance to perform the procedure in the face of posterior vertebral wall destruction. As this case demonstrates, the introduction of intrathecal contrast medium can allow for safe injection of PMMA with real-time visualization of the nerve roots and thecal sac and can demonstrate the posterior displacement of the soft-tissue tumor mass, which is not visible under conventional fluoroscopy. We have performed this procedure in six other patients with similar spinal tumors. In all six cases, the intrathecal contrast medium revealed scalloping of the thecal sac before optimal vertebral body filling, which resulted in early truncation of PMMA injection. In all of these cases, follow-up CT confirmed thecal sac encroachment that was seen at fluoroscopy. In our experience, there have been no deleterious consequences associated with intrathecal injection of contrast medium during percutaneous vertebroplasty.
- Received October 3, 2001.
- Accepted after revision July 1, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.