
Abstract
BACKGROUND AND PURPOSE: The possible relationship of orbit deformities in neurofibromatosis type 1 (NF1) to plexiform neurofibromas (PNFs) have not been fully elucidated. Our purpose was to review orbital changes in patients with craniofacial NF1.
METHODS: We retrospectively reviewed CT and MR imaging abnormalities of the orbit in 31 patients (18 male, 13 female; mean age, 14 years; age range 1–40 years) with craniofacial NF1.
RESULTS: Orbital abnormalities were documented in 24 patients. Six had optic nerve gliomas with enlarged optic canals. Twenty had PNFs in the orbit or contiguous to the anterior skull. The posterior orbit was distorted by encroachment from an expanded middle cranial fossa in 13 patients, and 18 had enlargement of the orbital rim. Other changes included focal decalcification or remodeling of orbital walls adjacent to PNFs in 18 patients and enlargement of cranial foramina resulting from tumor infiltration of sensory nerves in 16. These orbital deformities were sometimes progressive and always associated with orbital infiltration by PNFs.
CONCLUSION: In our patients with craniofacial neurofibromatosis, bony orbital deformity occurred frequently and always with an optic nerve glioma or orbital PNF. PNFs were associated with orbital-bone changes in four patterns: expansion of the middle cranial fossa into the posterior orbit, enlargement of the orbital rim, bone erosion and decalcification by contiguous tumor, and enlargement of the cranial foramina. Orbital changes support the concept of secondary dysplasia, in which interaction of PNFs with the developing skull is a major component of the multifaceted craniofacial changes possible with NF1.
Classic radiologic descriptions of sphenoid dysplasia include egg-shaped enlargement of the anterior orbital rim, bony defects in the posterior orbit, and anteroposterior enlargement of the middle cranial fossa (1, 2). These changes were understood to take place in the absence of tumoral involvement of the orbit or skull (1, 3). We recently reviewed a series of patients with craniofacial involvement by neurofibromatosis type 1 (NF1) (4) and suggested the term secondary dysplasia to indicate that the character of sphenoid bone abnormalities implied an interaction between the developing skull and contiguous plexiform neurofibromas (PNFs) present in utero or during early childhood rather than an exclusively dysplastic phenomenon (3). Previous reports have described the radiologic effects of orbital PNF infiltration (5), buphthalmos (6), and sphenoid dysplasia (2). In this article, we evaluate orbital soft-tissue and bony changes to determine the potential roles of dysplastic and interactive phenomena.
Methods
We reviewed radiologic data in all 31 patients with the diagnosis of NF1 who had CT scans on record in the Diagnostic Imaging Department. Twenty of these patients had images from more than one neuroimaging study acquired over a period of years that could be analyzed for possible progressive orbital changes. Most orbital CT studies (initial and repeat) were performed under the same orbital scanning protocol in which 1.5-mm, contiguous, axial images were obtained in neuro-ocular incidence (which included lenses, optic nerve heads, and optic canals in each eye in one reference plane with the eye in neutral position). Most patients had additional coronal views. Reconstructions based on bone and soft-tissue algorithms were available for review. Eight patients also had orbital and brain MR images.
Pathologic soft-tissue masses seen radiologically (other than radiologically obvious optic nerve gliomas) were assumed to be PNFs, because all patients met the National Institutes of Health criteria for neurofibromatosis (7) and 20 had histologically proved PNFs. The location of soft-tissue tumors was clinically and radiologically catalogued and determined to include the subcutaneous tissues of the lid, face, and jaw; the orbit and globe; the cavernous sinus; and the pterygoid fossa. Bone changes were noted. These included alterations in the orbital rim and periorbital sinuses, destruction and decalcification of focal areas of the orbital walls, and enlargement of the cranial nerve foramina in the skull.
Results
The patient group consisted of 18 male and 13 female subjects with an average age of 14 years (range, 1–40 years). Many of these patients had undergone surgery involving soft-tissue or globe tumors, but no patient underwent irradiation or surgery involving bone reconstruction, as recorded in the chart or as assessed on radiologic studies.
One patient had a normal CT scan. Six had only soft-tissue changes related to PNFs of the face without radiologic evidence of orbital or eye involvement. None of these patients had any bony orbital anomaly. The other 24 patients had involvement of the orbit, jaw, pterygoid fossa, cavernous sinus, or afferent visual system due to a soft-tissue tumor. Gliomas of the afferent visual system were present in six patients, four of whom had no orbital imaging abnormalities other than an enlarged optic canal. Bilateral soft-tissue tumors were present in three patients. Eighteen patients had radiologic changes in the sphenoid bone, and 13 of these had an associated bony orbital deformity.
The Table details how the orbital radiologic changes occurring in approximately two-thirds craniofacial NF1 patients follow a combination of four patterns:
Thirteen patients had expansion of the middle cranial fossa into the posterior orbit. All of these patients were proptotic, and 12 had radiologic evidence of ipsilateral deep orbit tumor infiltration or mass. Patients in whom the globe was deviated downward as well as forward all had superior orbit tumor (Fig 1A and B) or a bone defect in the roof of the orbit.
Eighteen patients had enlargement of the anterior orbital rim, all of whom had: a) buphthalmos, phthysis (Fig 2A) or enucleation due to buphthalmos; b) tumor infiltration of the extraconal space above the globe; c) a small ipsilateral maxillary sinus; or d) tumor involving the anterior orbit. Twelve of these patients also had encroachment of the middle cranial fossa into the posterior orbit (Fig 1B), but this was always accompanied by at least one other apparent cause of orbit rim expansion. The anterior orbit deformity was similar, but the degree of proptosis was less, in the absence of pathologic enlargement of the middle cranial fossa.
PNFs infiltrated the orbit in 19 patients. Radiologic evidence of PNFs in the orbit was always present ipsilateral to buphthalmos, but six patients had tumor infiltration of the orbit without buphthalmos. Tumor involved sensory nerves branches (Fig 3A), lacrimal gland, extraocular muscles, and orbital bones. The posterior orbit was commonly remodeled (Fig 2B) or decalcified or both, often in the presence of both an expanded middle cranial fossa and contiguous intraorbital tumor.
Sixteen patients had expanded foramina in the orbit (including the superior and inferior orbital fissures) (Fig 2B) and skull base (foramina ovale, rotundum, lacerum, and spinosum) (Fig 4) due to tumor enlargement of branches of the trigeminal nerve. Fifteen patients had obvious tumor extension into the cavernous sinus with remodeling of the sphenoid body (Fig 3B). Two patients had unilateral enlargement of the optic canal with radiologic evidence of optic nerve sheath PNF infiltration (Fig 4).

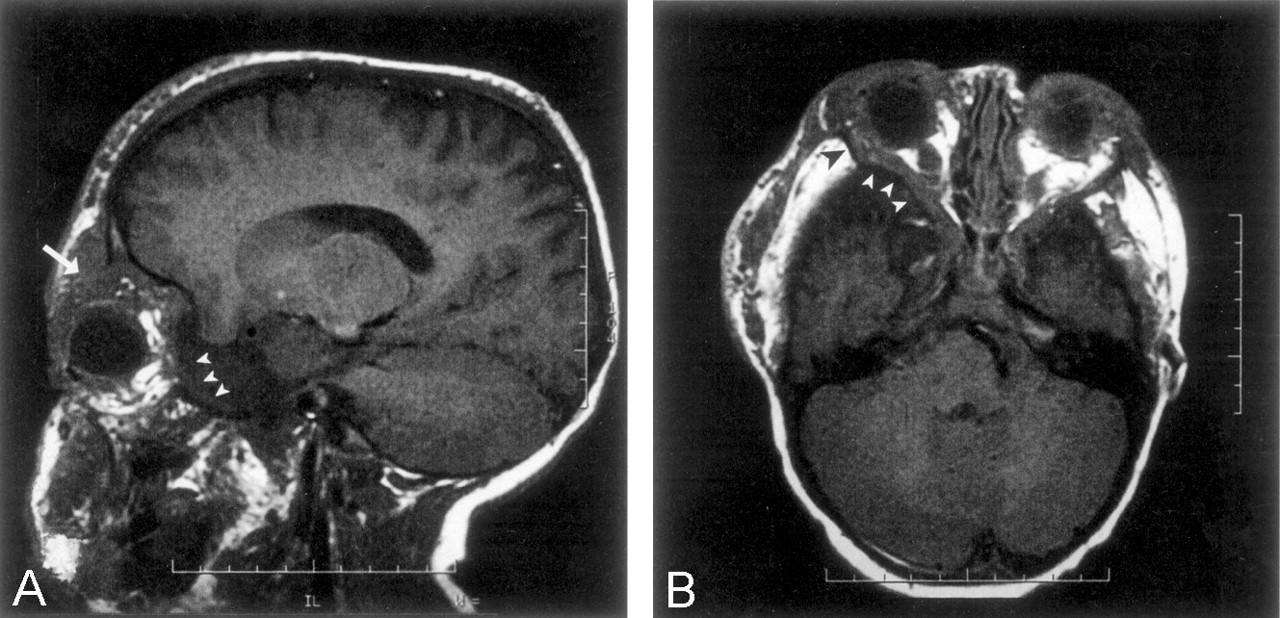
T1-weighted MR images.
A, Parasagittal image shows a temporal arachnoid cyst on the left that pushes the orbital contents, including the globe, forward (arrowheads), while a tumor mass in the superior quadrant of the orbit pushes the globe downward (arrow).
B, Axial image of the same patient with a temporal arachnoid cyst on the left (white arrowheads) shows shortening of the lateral wall of the orbit (black arrowhead) and flattening of the orbital angle. Also note the abnormal concave posterior aspect of the lateral orbital wall and the large wing of the sphenoid.

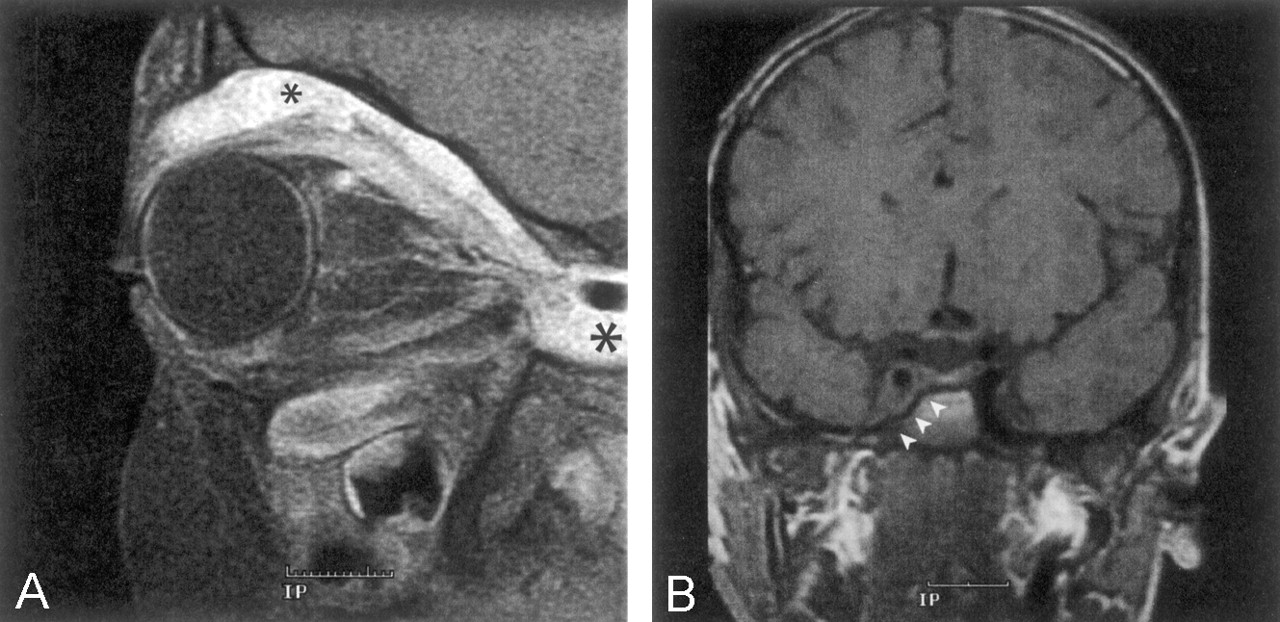
Coronal CT scans.
A, Image of the classic egg-shaped, orbital enlargement and deformity. Note the phthisical eye (asterisk) and tumoral infiltration of superior rectus muscle (arrow) and orbital septum (arrowheads). The left paranasal sinuses are underdeveloped. The nasal septum and crista galli are deviated.
B, Image of the posterior orbit shows that the tumors in the pterygoid fossa (asterisk) infiltrates the left orbital apex, enlarging the inferior orbital fissure and distorting the posterior orbit.

A, Sagittal T1-weighted, contrast-enhanced, fat-suppressed MR image shows infiltration of the superior extraconal space (small asterisk), superior rectus muscle, and levator palpebrae muscle by PNFs. Posterior extension of the tumor into the cavernous sinus is marked by the large asterisk. Intraconal sensory nerves are contrast enhanced and thickened because of tumor infiltration. Ipsilateral maxillary sinus is small compared with that on the contralateral side.
B, Coronal T1-weighted MR image of the same patient shows extension of the tumor into the cavernous sinus, with discrete remodeling of the sphenoid body (arrowheads).

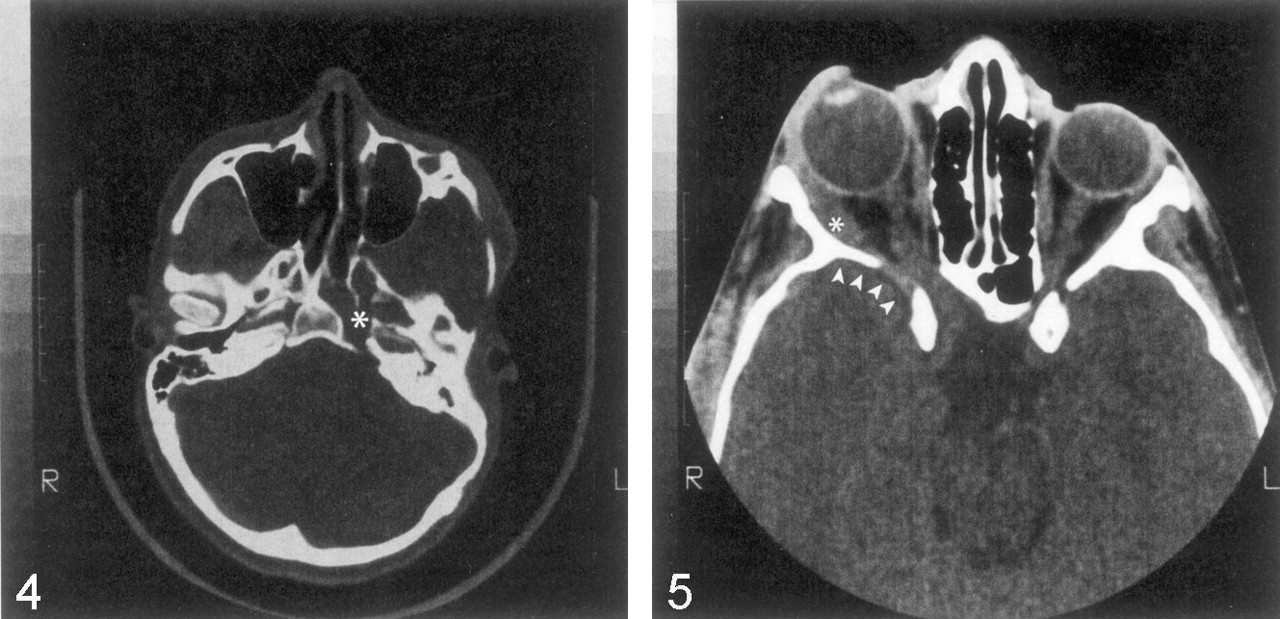
Axial CT image of the skull base shows expanded cranial foramina (foramen ovale, rotundum, and lacerum) on the left (asterisk) due to tumor enlargement of branches of the trigeminal nerve.

Axial CT image through the orbits shows unilateral enlargement of the right optic canal due to tumor infiltration of the optic nerve sheath without an optic nerve glioma. The ipsilateral globe is buphthalmic, and the lateral rectus (asterisk) is enlarged as a result of tumoral infiltration. The greater wing of the sphenoid is partially decalcified and bowed forward (arrowheads), without an obvious arachnoid cyst.
Patients with NF1
Three patients had bilateral facial neurofibromas, and each of these patients also had bilateral orbital and skull imaging changes. Repeat neuroimaging, when available, documented progression of the imaging abnormalities in each of the four patterns described before. Four patients had progressive enlargement of the middle cranial fossa (4).
Discussion
This report reviews orbital imaging changes in 31 patients with craniofacial NF1 who were evaluated at a tertiary-care ophthalmic institution over more than 15 years. Classically, sphenoid dysplasia has been considered the major factor influencing orbital changes (2), but recent investigators have questioned the dysplastic nature of sphenoid bone lesions in NF1 (4, 8). Jacquemin and colleagues (4) found sphenoid bone changes only in the presence of tumor in the superficial temporal fossa or deep orbit, in contrast to the classic opinion that skull changes occur independent of contiguous tumor (3). They proposed the concept of secondary dysplasia to incorporate the possibility that interaction with PNFs early in life might be essential to the development of sphenoid abnormalities in NF1.
The current review confirms previous observations that solitary optic nerve gliomas cause only enlargement of the optic canal (2) and that soft-tissue alterations in the globe, extraocular muscles, orbital nerves, and other orbital structures reflect PNF infiltration (5). We found that these soft-tissue alterations were both necessary and sufficient to explain the bony orbit deformities classically attributed to dysplasia. All four patterns of bony deformity in NF1 imply a similar type of interaction between PNFs and the developing orbital bone early in life, as identified in the sphenoid bone (4).
Encroachment of the greater sphenoid wing into the ipsilateral posterior orbit was the most striking orbit deformity, resulting in shortening of the lateral wall of the orbit and flattening of the orbital angle. In our patients, the normal concave anterior aspect of the lateral orbital wall was replaced by a concave posterior shape, which possibly reflected the pressure on the developing orbit from the enlarging middle cranial fossa. All 13 patients with these changes had PNFs in the ipsilateral superficial temporal fossa. This observation implies a possible interaction between the developing skull and PNFs early in life. In four patients, the anomaly was progressive over time, suggesting an acquired phenomenon (4). In fact, this type of orbital distortion also occurs in other settings in which development of the sphenoid bone is disturbed (1, 9, 10), and this distortion could be related to premature closure of the suture. The concept of congenital sphenoid dysplasia in NF1, conversely, does not explain why this type of orbital disturbance is often unilateral, why it always occurs ipsilateral to orbital and extracranial tumor, and why it progresses over time (8).
In every patient with encroachment of the posterior orbit by an enlarged middle cranial fossa, the volume of the orbit was decreased, with proptosis of the globe. In most of these patients, the eye was also displaced downward, but this change always occurred in the setting of PNF infiltration of the superior orbit, and it was often associated with thickening of superior recti and levator palpebrae muscles. The combination of anterior displacement of the globe due to encroachment by the middle cranial fossa and downward displacement due to a mass superior to the globe resulted in the classic egg-shaped orbital deformity. A similar anterior orbital deformity occurred in absence of a pathologically enlarged middle cranial fossa, but the degree of proptosis was less severe in those cases. Thus, several processes may act together to precipitate changes in the bony orbit and the position of the globe that previously were described simply as the result of sphenoid dysplasia.
Every patient with buphthalmos or its sequelae had an enlarged orbital rim. In NF1, congenital glaucoma might result from either maldevelopment of or PNF infiltration into the anterior chamber angle (5). In either case, blockage of the drainage of the aqueous humor results in increased intraocular pressure and marked enlargement of the globe (buphthalmos) in both the anteroposterior and transverse dimensions. The increased transverse diameter of a buphthalmic eye may act like an intraconal mass and cause symmetric, geometric, orbital enlargement, as do other orbital masses that occur early in life (2, 11).
Patients with expanded orbital rims had hypoplasia of the ipsilateral maxillary sinus, always with PNF in the pterygoid fossa. Tumor in the pterygoid fossa may prevent normal expansion of the maxillary sinus, although in our patients this seemed to affect the anteroposterior dimension of the maxillary sinus more than the craniocaudal axis. Similarly, when PNFs extended into the cavernous sinus, scalloping of the sphenoid body and often hypoplasia of the sphenoid sinus were apparent adjacent to the tumor. Since many patients in our review had other possible causes of orbital deformity as well, the contribution of maxillary and sphenoid sinus hypoplasia to the orbital abnormality remained ambiguous. Only two patients with an expanded orbital rim had neither buphthalmos nor a small maxillary sinus, and these patients had substantial tumor mass in the anterolateral orbit that likely caused remodeling of the rim.
Areas of the bony orbit, particularly the posterior orbit and lateral wall, were sometimes radiologically decalcified or remodeled. This type of bony change always occurred contiguous to PNFs, implying an important interaction between tumor and bone. A similar interaction between PNF and bone was present in other parts of the skull, including the temporal bone and even the occipital bone (4). The bone contour was left intact in most locations because the tumor did not cause gross destruction of the skull or an obvious disruption of skull development. However, in some locations, particularly in the lateral orbital wall, the anatomic structure was destroyed and replaced by the tumor itself. This finding contradicts previous reports where no tumor was found adjacent to areas of skull destruction (3), but it agrees with observations made in other parts of the body (1).
Enlargement of orbital foramina was the fourth type of bony change. Enlargement of the superior and inferior orbital fissures always occurred with radiologic evidence of orbital tumor, which represented PNFs infiltrating the branches of the trigeminal nerve (5, 12). PNF infiltration of other trigeminal branches likely caused enlargement of cranial base foramina, and PNFs extending in a proximal direction occasionally formed a mass in the cavernous sinus that remodeled the body of the sphenoid. Foraminal enlargement and infiltration of the cavernous sinus had no correlation with, and should not be confused with, the radiologic appearance of classic sphenoid dysplasia. PNF infiltration also involved the optic nerve sheath, probably by extension along meningeal branches of the long ciliary nerves (5). Two of our patients had radiologic evidence of involvement of the sheath of the optic nerve that caused secondary enlargement of the optic canal. To our knowledge, this phenomenon has not been described previously and should be considered in the differential diagnosis of enlargement of the optic canal in the setting of NF1.
Orbital deformity was progressive over time. A combination of progressive posterior orbital encroachment (4), an increase in the orbital soft-tissue mass (11), or progressive buphthalmic globe expansion (13) provided an adequate explanation for continuing orbital changes. These bony changes can be explained by processes directly or indirectly related to the presence of tumor.
Conclusion
PNFs present early in life probably play a more important role in the abnormal development of the orbit and skull than has been classically accepted (4). These tumors appear in utero or during early childhood in some patients and, therefore, they are present to interact with the skull, orbital structures, and globe while they are still developing. The tumors affect nearby bone and invade almost all of the orbital structures, including the globe, extraocular muscles, optic nerve sheath, and branches of the sensory nerves. The presence of PNFs explains why the problems of craniofacial NF1 are so often unilateral, why they occur ipsilateral to the extracranial tumor, and why they are progressive over time. Patients with NF1 have well-documented dysplastic histologic changes involving the bone, meninges, and brain, and interaction between PNFs and some components of these tissue abnormalities during skull development remains possible. Therefore, the term secondary dysplasia seems more appropriate to describe the sum of the skull and orbital abnormalities in NF1 mentioned in this report and elsewhere. This term acknowledges a traditional concept while admitting that current neuroimaging suggests a more multifaceted and interactive pathogenesis.
References
- Received December 16, 2002.
- Accepted after revision March 25, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Posterior-Anterior Cephalometric Study of Neurofibromatosis Type 1 Patients With Facial Plexiform Neurofibroma: Analysis of Skeletal Symmetry Concerning Midfacial and Skull Base Reference Points (Zygomatic Arch, Mastoid, and Juga)
- Sphenoid Bone Pneumatisation on Lateral Cephalograms of Patients With Neurofibromatosis Type 1
- Periapical Cemento-osseous Dysplasia Is Rarely Diagnosed on Orthopantomograms of Patients with Neurofibromatosis Type 1 and Is Not a Gender-specific Feature of the Disease
- Optic Pathway Glioma and Cerebral Focal Abnormal Signal Intensity in Patients with Neurofibromatosis Type 1: Characteristics, Treatment Choices and Follow-up in 134 Affected Individuals and a Brief Review of the Literature
- Analysis of Orbital Plain Radiographs for Orbital Deformities in Neurofibromatosis Type 1 Patients, with Special Reference to Alterations of the Orbital Rim as Indicators of Adjacent Plexiform Neurofibroma
- Reconstruction of the Sphenoid Wing in a Case of Neurofibromatosis Type 1 and Complex Unilateral Orbital Dysplasia with Pulsating Exophthalmos
- Dysplasia of the Orbit and Adjacent Bone Associated with Plexiform Neurofibroma and Ocular Disease in 42 NF-1 Patients