
Abstract
BACKGROUND AND PURPOSE: Quantitative evaluation of midbrain atrophy may be useful in differentiating progressive supranulear palsy (PSP) from Parkinson disease (PD); however, this finding is not specific of PSP, and quantitative measurements are not always practical. We determined whether an abnormal superior midbrain profile (flat or concave aspect) is a more practical diagnostic parameter for PSP.
METHODS: MR imaging studies of 25 patients with PSP and 27 with PD were reviewed by means of five parameters: midbrain superior profile on midsagittal T1-weighted images, midbrain atrophy, tegmental abnormal T2 hyperintensity, abnormal T2 putaminal hypointensity or hyperintensity on axial proton density–weighted images. We also measured the anteroposterior diameter of the midbrain on axial T2-weighted sections at the level of the superior colliculus.
RESULTS: The finding of an abnormal superior profile of the midbrain had 68% sensitivity and 88.8% specificity. Midbrain atrophy had 68% sensitivity and 77.7% specificity. Tegmental T2 hyperintensity had 100% specificity but poor sensitivity (28%). Only 14.8% of patients with PD and 24% of those with PSP had abnormal putaminal T2 hypointensity; none had proton-density hyperintensity. With PSP, the average midbrain diameter was smaller than that with PD, but an important overlap was observed. Reader discordance was lower for the midbrain superior profile sign (eight of 52 cases); this was similar for tegmental hyperintensity (nine of 52 cases) and higher for midbrain atrophy (16 of 52 cases).
CONCLUSION: An abnormal superior profile of the midbrain facilitates the distinction of PSP from PD and may support the clinical differential diagnosis of parkinsonism.
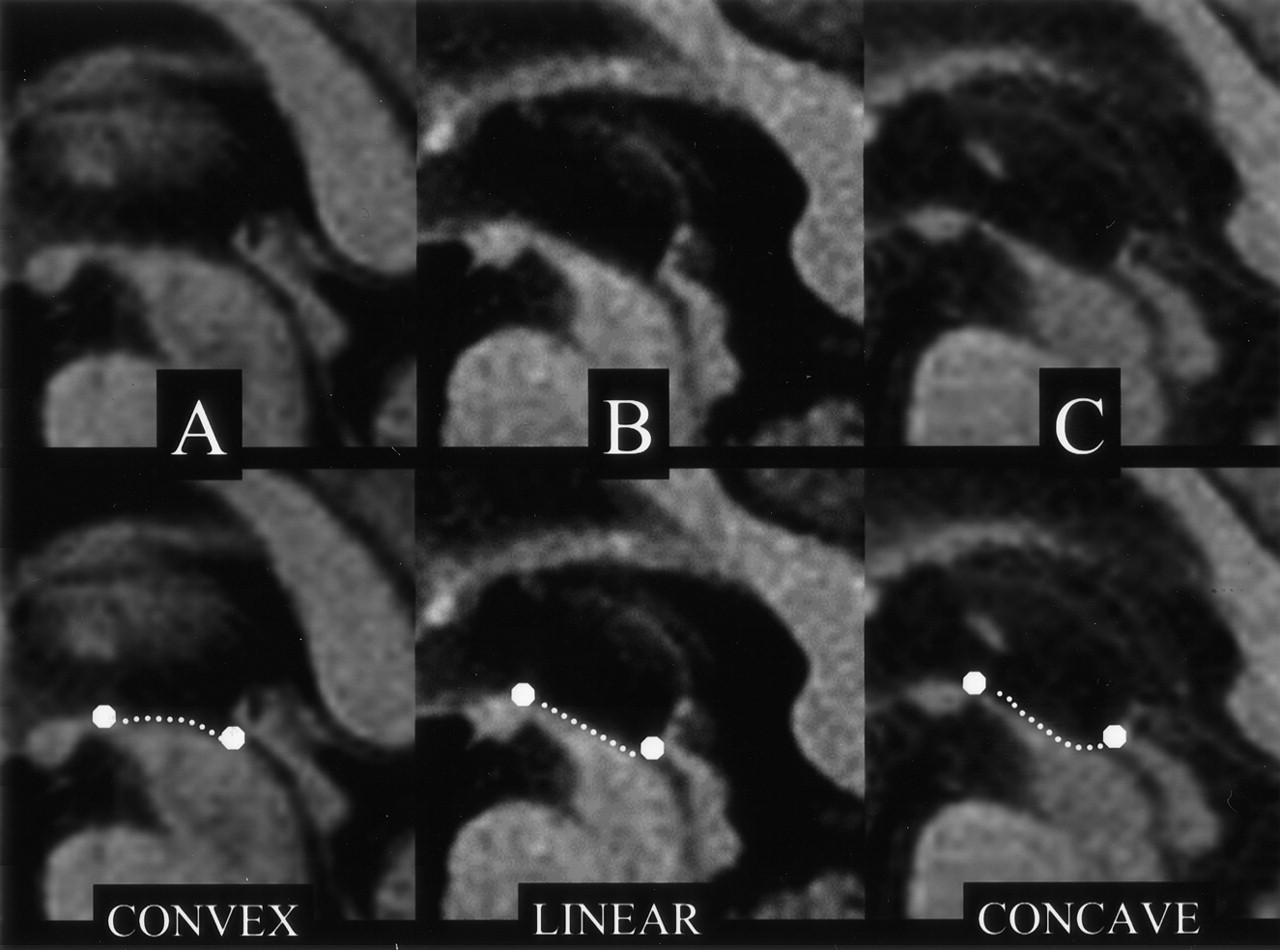
Progressive supranuclear palsy (PSP) is a neurodegenerative disease that results in severe disability. It is characterized by supranuclear vertical gaze palsy, pseudobulbar palsy, dystonic rigidity of the neck and upper extremities, and frequent falls (1). The main neuropathologic characteristics of PSP are neuronal degeneration and loss in the tegmentum of the midbrain, atrophy of the substantia nigra (SN), and changes in the red nucleus and globus pallidus (2). The clinical diagnosis of PSP, particularly its differential diagnosis with Parkinson disease (PD), can be difficult, especially in early stages (3). However, the differential diagnosis between PSP and PD is important, because the prognosis of PSP is worse than that of PD. In the last 10 years, MR imaging investigations of PSP have shown abnormalities mainly involving the midbrain; such changes include atrophy, abnormal T2 hyperintensity in the tegmentum, and narrowing of the SN (4–7). However, the introduction of MR imaging into the routine workup of patients with suspected PSP or other parkisonian syndromes has been hampered by its low sensitivity and poor specificity and also by high variability, which can be heavily influenced by the neuroradiologist’s experience. Reports have shown that the quantitative evaluation of midbrain atrophy, based on its anteroposterior (AP) diameter calculation, is useful in the differential diagnosis of PSP and PD, because it is more reproducible and less affected by reader experience (8). However, atrophy of the midbrain is not specific to PSP, as it has been also reported in PD and other parkinsonian syndromes (9). Moreover, quantitative measurements are not always practical and easy to perform in everyday practice. Therefore, we evaluated the presence of abnormal superior profile of the midbrain in PSP and PD. This sign is based on the observation that, in PSP, the atrophic midbrain (besides reduced AP diameter) shows a characteristic alteration in the normal convex profile of its superior surface, which tends to assume a flat or concave aspect on midline sagittal T1-weighted sections (Fig 1). We hypothesized that a pathologic change in the normal convex profile is easier and more straightforward to evaluate and less prone to interobserver variability than other MR imaging findings. We tested this hypothesis in PSP and PD patient populations to determine the sensitivity and specificity of this sign.

Top row, Midsagittal T1-weighted spin-echo sections in PD (A) and PSP (B and C) show the midbrain region. Bottom row, Same images with outlined profiles of the upper midbrain, which appears convex in A, linear (flat) in B, and concave in C.
Methods
Patient Selection
From our Movement Disorders Clinic database, we identified 25 consecutive patients with PSP who had undergone 1.5-T MR imaging in our MR service with the same image acquisition protocol. All patients with PSP had presented with early-onset postural instability, gaze palsy, axial rigidity, bradykinesia, and no notable response to dopaminergic drugs. They all fulfilled the clinical diagnostic criteria for probable PSP proposed by Litvan et al (10). We then selected 27 patients with PD that was diagnosed according to Parkinson’s Disease Society Brain Bank criteria (11). This group had also undergone imaging with the same MR protocol. To further increase our confidence in the clinical diagnoses, all patients had to have been clinically followed up for at least 1.5 years after the MR imaging study, and the diagnosis had been confirmed in all of them. The two groups did not significantly differ in mean age or symptom duration at the time of MR imaging, but the mean Hoehn-Yahr stage was significantly higher for PSP patients because of the more severe and rapid course of their disease (Table 1).
Demographic and clinical data
MR Imaging Protocol
The MR imaging protocol was as follows: First, sagittal, 5-mm-thick, T1-weighted spin-echo images (TR/TE/NEX, 500/9/1; 240-mm FOV, 192 × 256 matrix) had been acquired. Then, axial, 3-mm-thick contiguous double-echo conventional spin-echo images (2000/20–80/2, 230-mm rectangular FOV, 192 × 256 matrix) centered on the midbrain and basal ganglia and oriented perpendicular to the main axis of the midbrain, and axial, 5-mm-thick, T2-weighted fast spin-echo (FSE) images (4600/90/1, 230-mm rectangular FOV, 192 × 256 matrix) were acquired to encompass the whole brain. These images were oriented according to the bicommissural line.
Data Analysis
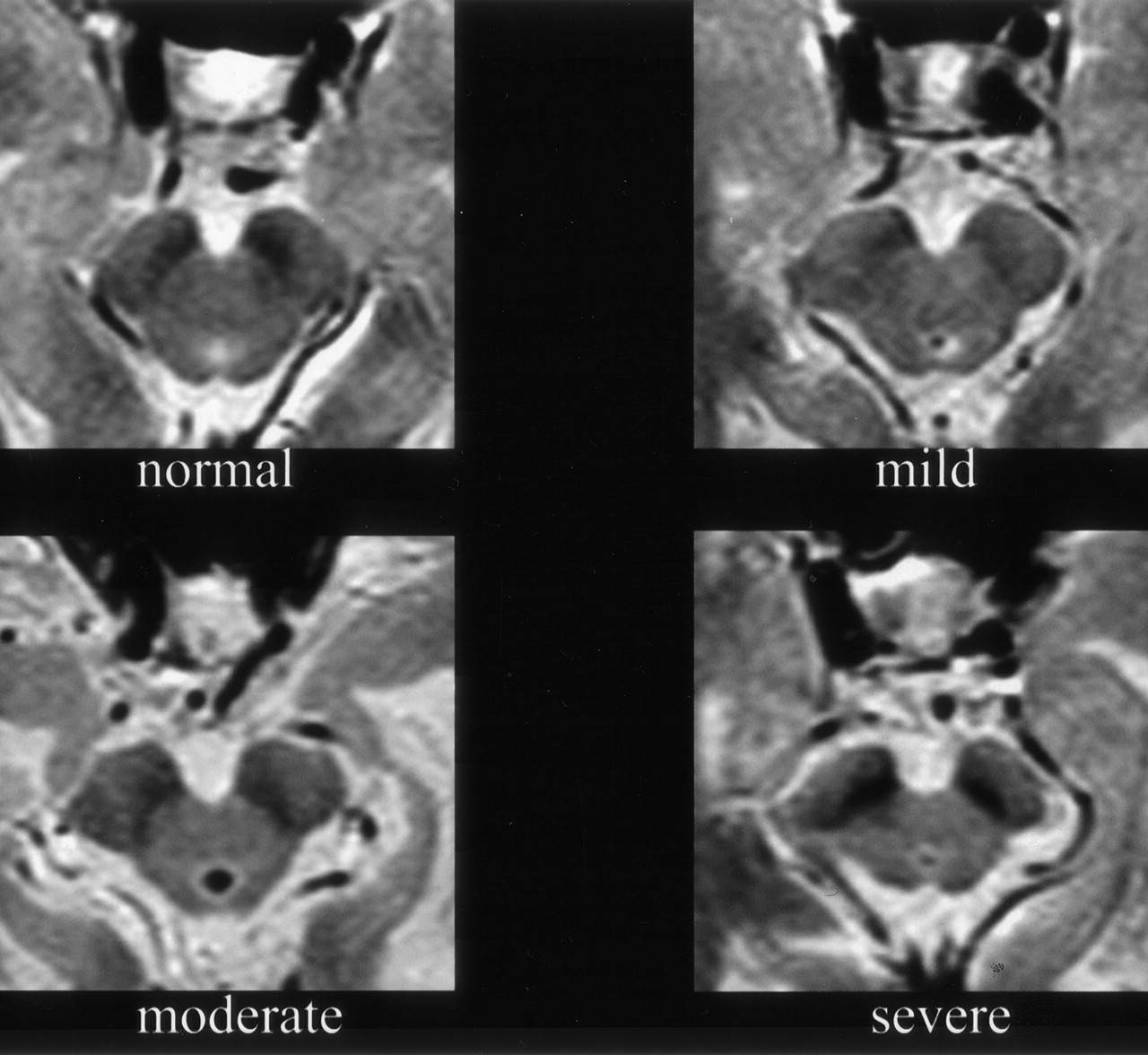
Two senior neuroradiologists (A.R., E.B.) who were blinded to the clinical data analyzed the MR images independently and consecutively. They evaluated six parameters, as follows: 1) The superior profile of the midbrain on the midsagittal T1-weighted image was assessed. This was considered normal when it was convex, as represented by an imaginary curve connecting a point immediately posterior to the mammillary body and one located at the upper orifice of the aqueduct (Fig 1). The profile was considered abnormal when it was flat or concave, as identified by using the same imaginary line or curve (Fig 1). 2) Midbrain global atrophy was assessed on axial, 3-mm-thick, T2-weighted images and graded as normal (no atrophy), mild, moderate, or severe (Fig 2). Detection of the entire perimesencephalic cistern (without interruption of CSF signal intensity) on at least one side was considered a sign of mild atrophy. To discriminate between mild and moderate atrophy, progressive enlargement of the interpeduncular cistern was considered. To acquaint themselves with this parameter, the two raters performed brief trial cases randomly selected from our Movement Disorders Clinic archive. 3) They assessed the presence of abnormal hyperintensity in the mesencephalic tegmentum on 3-mm-thick, T2-weighted images (Fig 3). 4) The 3-mm-thick, T2-weighted images were reviewed for hypointensity in the posterolateral putamen greater or equal to that in the globus pallidus. 5) Proton density–weighted, 3-mm-thick images were evaluated for hyperintensity in the posterolateral putamen greater than that of the central thalamus. The last two parameters (4 and 5) were evaluated according to the method illustrated by Righini et al (12). 6) The AP diameter of the midbrain at the level of the superior colliculus was measured on T2-weighted, 3-mm-thick, axial spin-echo section by tracing a line on the MR console (Fig 4). In case of disagreement between the two raters on parameters 1–5, the images were reevaluated together until a consensus was reached.

Axial, 3-mm-thick, T2-weighted spin-echo sections show different degrees of midbrain atrophy.

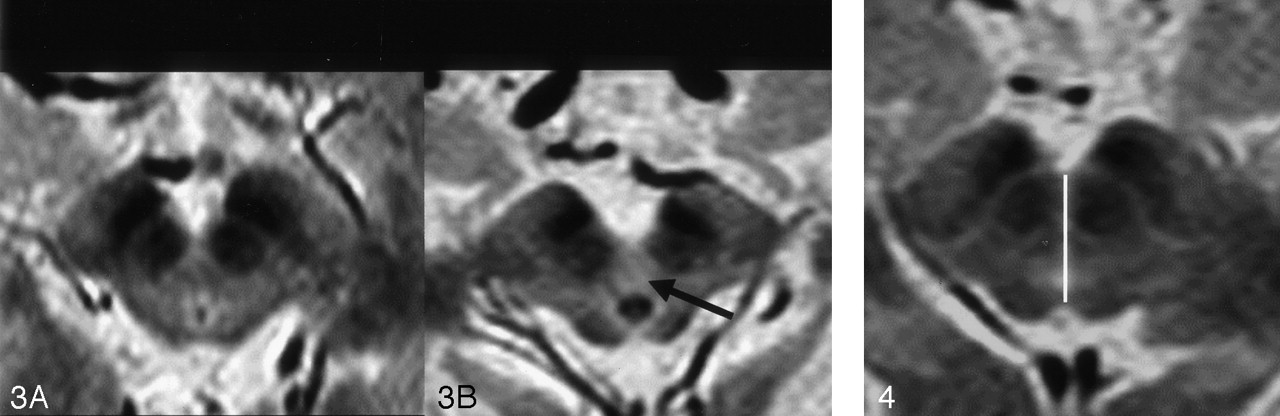
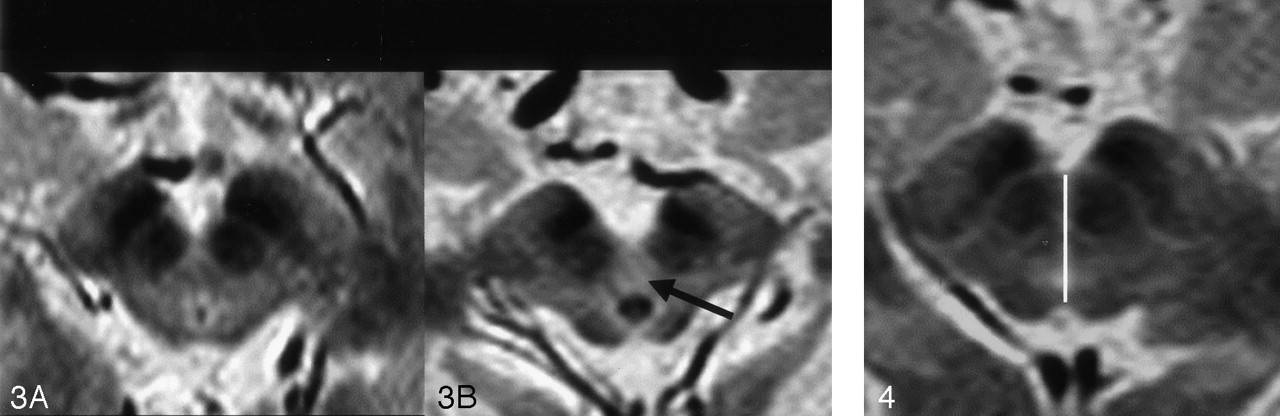
Axial, 3-mm-thick, T2-weighted spin-echo sections show no abnormal tegmental hyperintensity (A) and abnormal tegmental hyperintensity (B, arrow).
Statistical analysis was performed by using a nonparametric statistic (Spearman rank correlation) to evaluate correlations between the severity of the superior profile of the midbrain alteration (concave being considered more abnormal than linear) and the AP midbrain diameter reduction, as well as the degree of global atrophy of the midbrain. Group comparisons between PD and PSP were carried out by using an unpaired t test.
Results
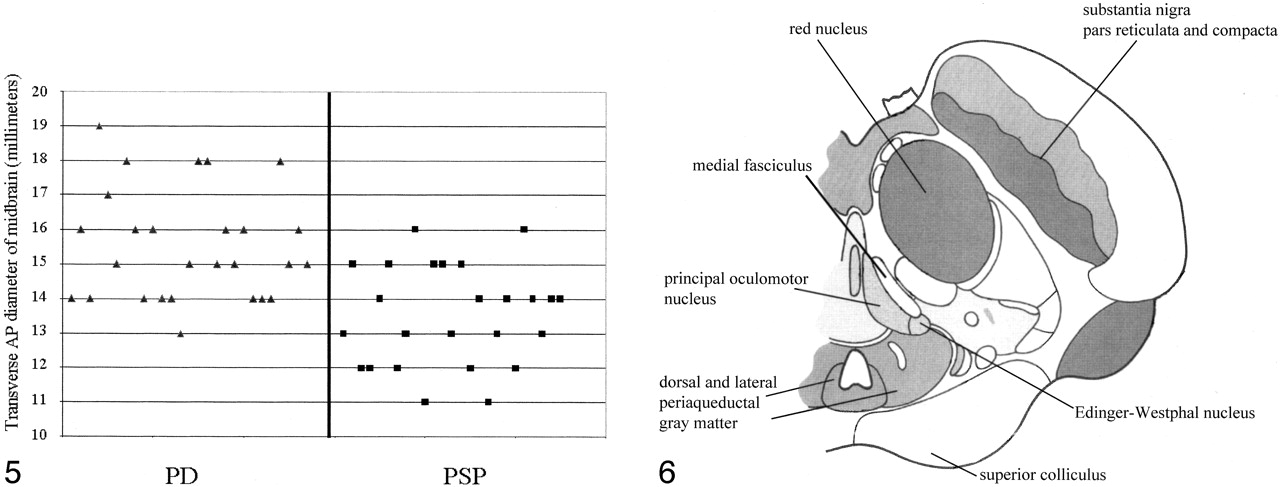
Table 2 shows the results for parameters 1–5. The presence of abnormal superior profile of the midbrain had 68% sensitivity and 88.8% specificity. The presence of global atrophy of the midbrain had 68% sensitivity and 77.7% specificity. The presence of abnormal tegmental T2 hyperintensity had a sensitivity of 28% and a specificity of 100%. Only 14.8% of patients with PD and 24% of those with PSP had abnormal T2 hypointensity in the posterolateral putamen, and none had abnormal putaminal proton-density hyperintensity. The PSP population had an average AP midbrain diameter smaller than that of the PD cohort (13.5 ± 1.4 mm vs 15.5 ± 1.6 mm; P < .0001, unpaired t test), but there was an important overlap between the two populations. The observed threshold value of 12 mm distinguished only seven of 25 subjects with PSP (Fig 5). Discordance between the two readers was lower for the superior profile of the midbrain sign (eight of 52 cases), similar for the tegmental T2 hyperintensity (nine of 52 cases), and higher for global atrophy of midbrain (16 of 52 cases). We did not find a significant correlation between alteration in the superior profile of the midbrain and reduction in the AP diameter (P = .4). There was a significant correlation between alteration in the superior midbrain profile and the global atrophy of the midbrain (P = .009).

Axial, 3-mm-thick, T2-weighted spin-echo section depicts the method used to measure the AP diameter of the midbrain at the level of the superior colliculus.

Graph illustrates the distribution of midbrain transverse AP diameters for the PSP and PD populations. A threshold value of 12 mm included only seven of 25 patients with PSP.

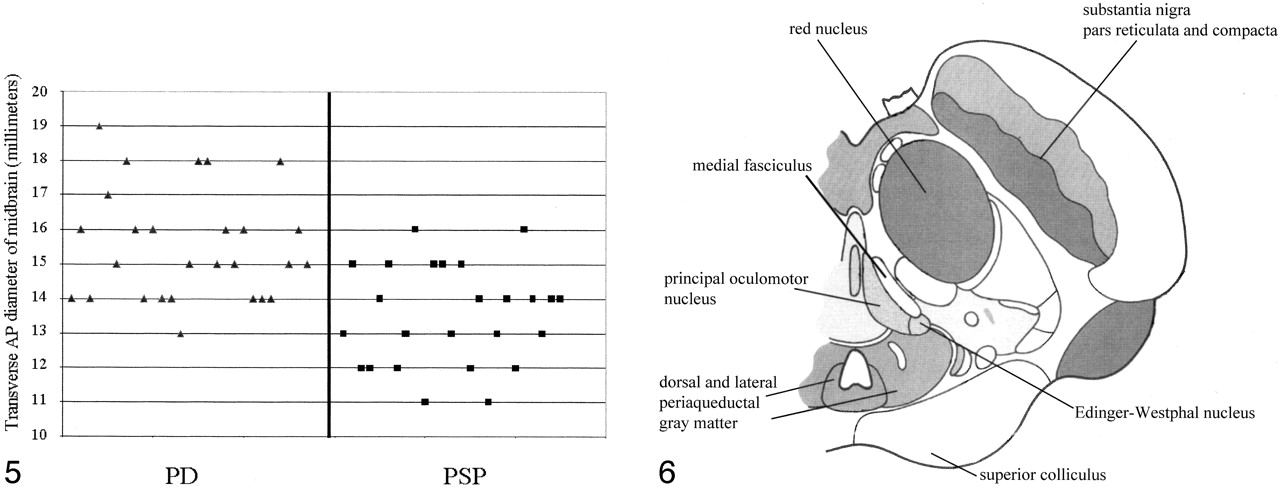
Diagrammatic representation of an axial section of the midbrain at the level of superior colliculus (modified from figure 54 of Duvernoy HM, The Human Brain Stem and Cerebellum, 1995, with permission of Springer-Verlag, Wien). Some of the structures affected in PSP have been reported. Other structures of the dorsal and cranial part of the midbrain affected in PSP (ie, nucleus interstitialis of Cajal and pretectal area) are located on the contiguous cranial section.
Results of the assessment of parameters 1–5
Discussion
We found that the presence of an abnormal superior midbrain profile had the same sensitivity, but higher specificity, than the global atrophy parameter. Moreover, it was less sensitive to interobserver variability. Although tegmental T2 hyperintensity had the highest specificity, it provided low sensitivity, which makes it of little use in evaluating suspected PSP. Therefore, we believe that the superior midbrain profile is the most robust MR imaging sign for identifying PSP in a routine clinical setting.
An important characteristic of the superior midbrain profile is that the observers were more confident in evaluating its alterations (less interobserver variability), probably because of the monodimensional nature of the parameter. In other words, even without specific experimental references in the vision neuropsychology literature, it is conceivable that differences between a straight line and a curve (in our case, the profile of the superior midbrain) are more immediate and easier to visually detect than those associated with absolute variations of an area (in our case, the midbrain contour on axial sections); this is especially true when a single case is considered as is usual in radiologic practice.
Our results support previous findings indicating a significantly decreased average midbrain AP diameter in PSP (8, 13). Although previous authors found a clear cutoff value separating PSP from PD, we found an important overlap, and the observed threshold value of 12 mm included too few PSP subjects to be of practical use (Fig 5). This discrepancy can be explained by differences in the measurement methods: we traced our measurement on axial, 3-mm-thick, T2-weighted sections perpendicular to the main axis of the midbrain, and all images were acquired with the same protocol. In contrast, Warmuth-Metz et al (8) and Schrag et al (13) traced the AP diameter on axial 5–7-mm-thick sections obtained with different MR units. Therefore, our measurement might be accurate given the better spatial resolution and the smaller technical variability between imaging sessions. Indeed, some degree of midbrain atrophy may also be present in PD. In particular, a significant reduction in thickness of the SN, which affects the AP diameter of the midbrain, has been detected in MR imaging studies of patients with PD compared with those in healthy control subjects (14, 15). This observation is consistent with the reduction in midbrain AP diameter found in several of our patients with PD.
We speculate that the progressive flattening and excavation of the superior profile is related to a marked focal parenchymal loss in this area, which coexists with more general global atrophy of the entire midbrain. Indeed, histologic studies of the midbrain in PSP revealed severe neuronal loss in the periaqueductal gray matter, Edinger-Westphal nucleus, nucleus interstitialis of Cajal, pretectal area, cuneiform nucleus, and rostral interstitial nucleus of the medial fasciculus (16). Moreover, the medial fasciculus itself undergoes substantial atrophy. These structures are mainly located in the cranial and dorsal part of the midbrain, and their atrophy may explain the local volume reduction and the loss of the normal convex profile (Fig 6).
We did not find a significant correlation between the progressive loss of the normal convex superior profile of the midbrain (from convex to linear and finally concave) and the reduction in AP diameter. We cannot provide a clear explanation for this finding. In PSP, an important reduction in SN thickness and atrophy of the red nuclei have been reported (16, 17); these structures are located in the ventral and central parts of the midbrain, respectively. It is possible that atrophy of the SN and red nuclei mainly contributes to the reduction in the AP diameter of the midbrain, whereas the abnormal superior profile is associated with atrophy of the medial fasciculus and the other minor mesencephalic nuclei previously mentioned; these are located in the upper portion of the midbrain. Probably, the same patient with PSP develops degeneration of the SN, red nucleus, and the other minor mesencephalic nuclei with different degrees of severity. To better assess differences in the degree of atrophy in various parts of the midbrain, a 3D imaging dataset might be useful for automatically segmenting them and for measuring the volume of the affected structures. In our retrospective protocol, we did not perform 3D sequences, and this kind of sophisticated analysis was not possible.
We found a significant correlation between alterations in the superior midbrain profile and global atrophy of the midbrain. Because both values were obtained by means of visual assessment, they are likely to be perceived in a similar fashion by the readers.
We did not consider other kinds of parkinsonism in the differential diagnosis of PSP, such as the striatonigral (parkinsonian) type of multiple system atrophy (MSA-P). Previous studies (12, 18) have revealed that, in MSA-P, MR imaging signs of putaminal degeneration and gliosis (eg, T2 or proton-density hyperintense bands in the posterolateral putamen) are detected in up to 83% of cases, and they are highly specific for this disease. Righini et al (12) compared PD and MSA-P populations and found that the proton density–hyperintense band in the posterolateral putamen was 100% specific, being present only in MSA-P. T2 putaminal hypointensity was clearly less specific, as it was visible in a percentage of patients with PD, similar to the one we report in our PD population. Using the same imaging protocol reported by Righini et al (12), we found no abnormal proton-density hyperintensity in the putamen among any of our patients with PSP or PD. During the 1.5 years of follow-up, none of our patients fulfilled the clinical criteria for MSA-P proposed by Quinn (19) and revised by Gilman et al (20). Therefore, the possibility that some patients with MSA-P were included in the cohort is unlikely. Although PD, MSA-P, and PSP can share common clinical features at an early stage, they are completely different disorders neuropathologically.
Finally, we did not include a healthy control group. However, this study aimed at identifying MR imaging signs that may help the neurologist to differentiate PSP from PD in the clinical setting. Therefore, we believed that a control group was unnecessary.
In conclusion, we found an abnormal midbrain superior profile distinguishes PSP from PD and may be useful in the clinical differential diagnosis of parkinsonism.
References
- Received April 3, 2002.
- Accepted after revision February 24, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Atypical Parkinsonian Syndromes: Structural, Functional, and Molecular Imaging Features
- Neuroimaging of Rapidly Progressive Dementias, Part 1: Neurodegenerative Etiologies
- Differentiation between idiopathic and atypical parkinsonian syndromes using three-dimensional magnetic resonance spectroscopic imaging
- The midbrain to pons ratio: A simple and specific MRI sign of progressive supranuclear palsy