
Abstract
Summary: We report a case of a ganglioneuroma that was found incidentally on a CT of the abdomen in a 27-year-old woman with gastrointestinal symptoms. The tumor, though located in the posterior mediastinum, demonstrated an unusual feature of abundant adipose tissue on MR imaging. The mass was later resected, and adipose tissue intermixed within a ganglioneuroma was identified microscopically. Adipose tissue is a rare finding in a ganglioneuroma, but this radiographic feature may be useful in the evaluation of posterior mediastinal masses.
Ganglioneuroma is one of several tumors reported to occur in the posterior mediastinum (1–5). The list includes Schwannoma, neurofibroma, ganglioneuroblastoma, neuroblastoma (1–3), malignant peripheral nerve sheath tumor (1, 2), lymphoma (1, 3), primitive neuroectodermal tumor (2), pheochromocytoma (2, 3), paraganglioma, hemangioma, fibroma, fibrosarcoma, lipoma, liposarcoma (3), chordoma (6), desmoid tumor (7), and teratoma (8, 9). Many of these tumors demonstrate similar features on neuroimaging. We present a case of a posterior mediastinal mass with a large fatty component seen on MR imaging studies. This is a rare finding that distinguishes ganglioneuroma from other posterior mediastinal tumors (10).
Case Report
A 27-year-old woman was referred to our hospital for an evaluation of a right-sided posterior mediastinal mass that was incidentally discovered on a CT of the abdomen performed because of gastrointestinal symptoms. She had no significant past medical history except for asthma and denied any symptoms relating to this mass. Her examination was notable only for deep tendon reflexes that were more brisk in the lower extremities than in the upper extremities without any clonus.
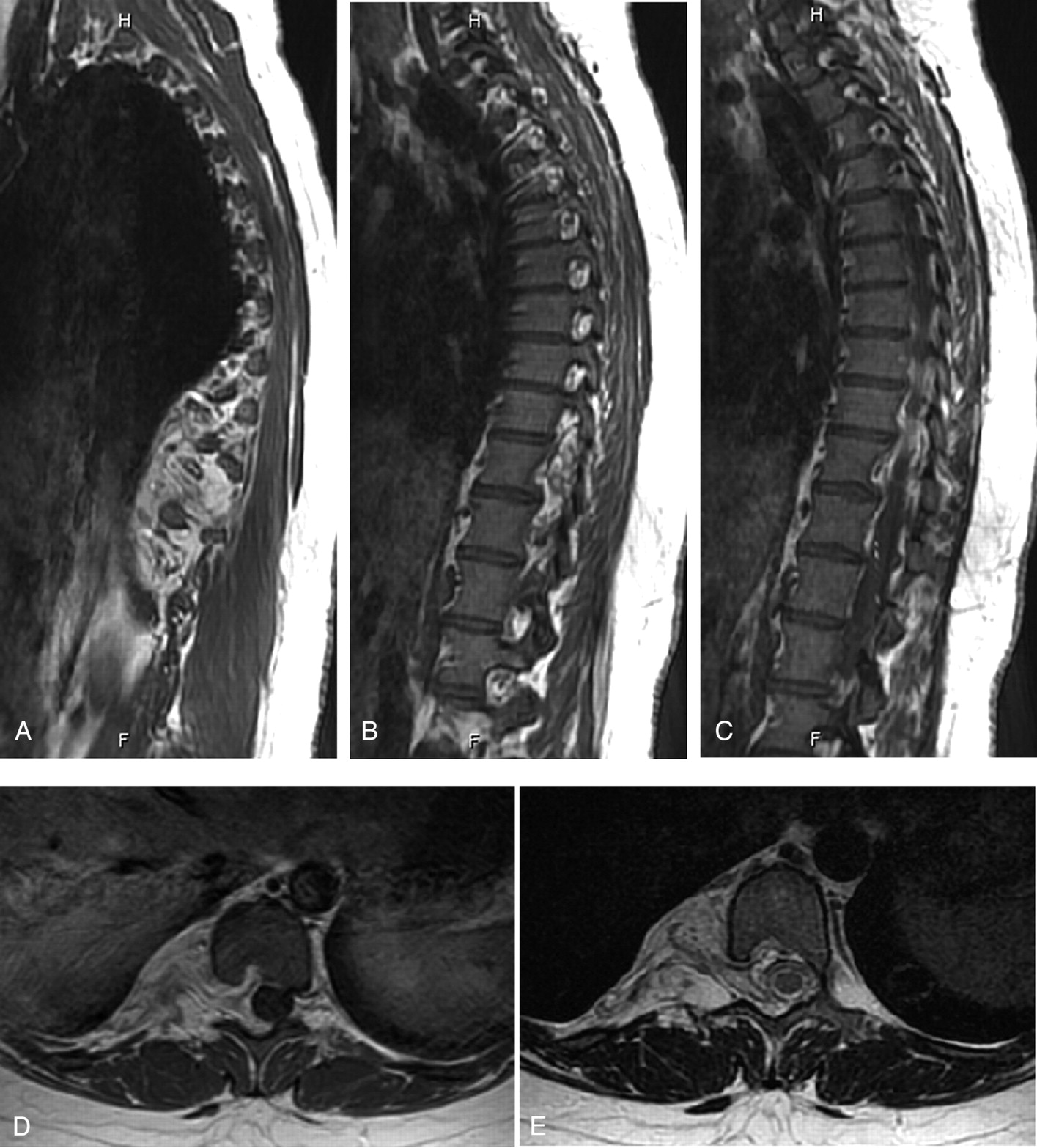
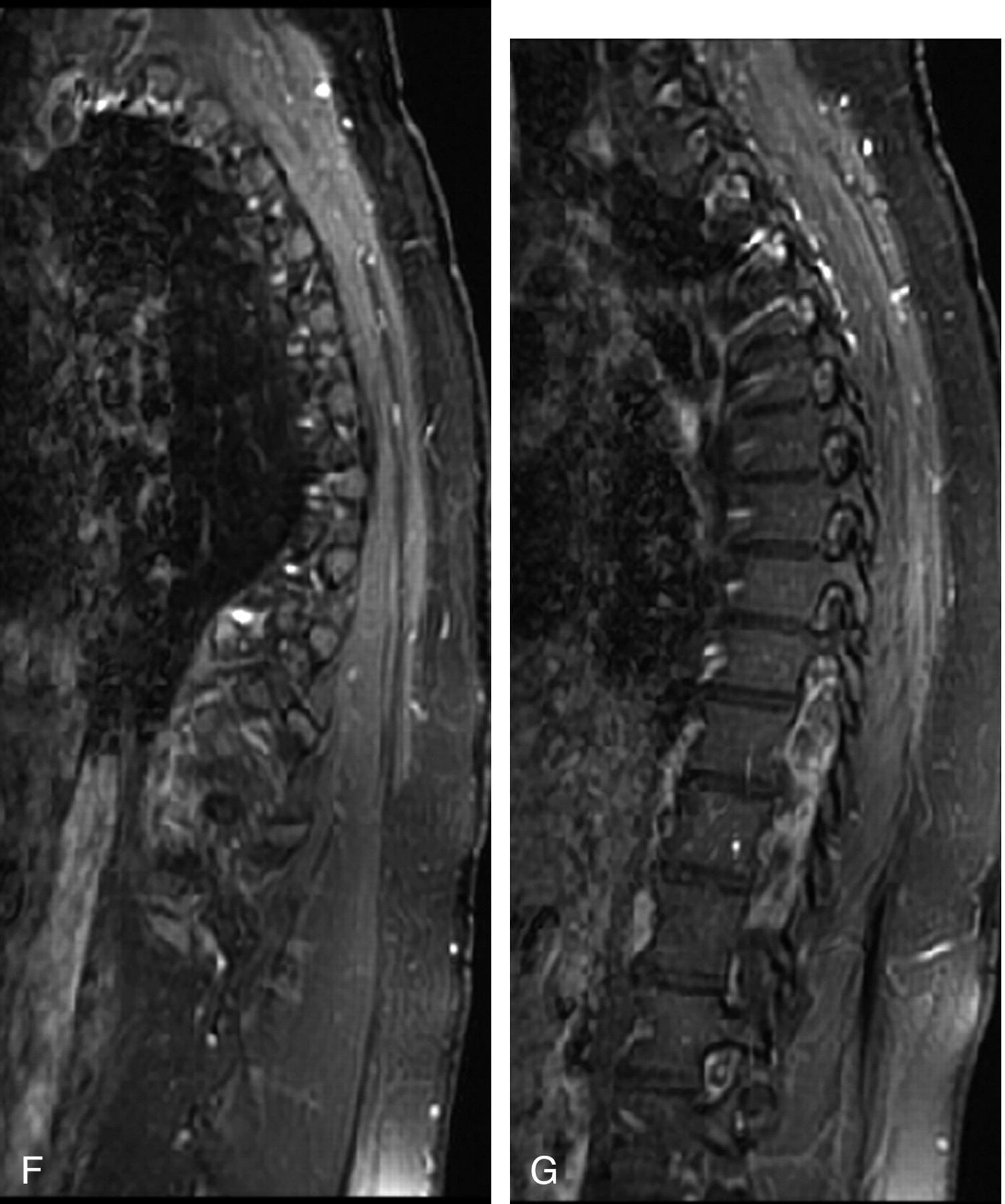
A noncontrast and postcontrast MR imaging of the thoracic spine demonstrated a right paravertebral mass that extended from T9 to T12. It appeared to enter and widen the right intervertebral foramina at all the intervening levels and effaced the right side of the spinal cord, displacing it slightly toward the left. On the T1 (TR 366/TE 14) and T2 fast spin-echo (TR 3400/TE 110)–weighted images, the mass showed predominant high signal intensity similar to adjacent subcutaneous fat (Fig 1A–E). There were areas of intermediate T1 and T2 signal intensity within the mass, and the postcontrast T1-weighted (TR 300/TE 14) images showed some enhancement in the areas of intermediate T1 signal intensity. The fat-suppressed postcontrast images showed low signal intensity within the paraspinal mass (Fig 1F, -G). There were interspersed areas of enhancement within the mass (Fig 1F, -G). Our differential diagnosis based on these radiologic features included a Schwannoma, a ganglioneuroma, and an angiolipoma. The latter 2 possibilities were gleaned from a review of case reports in the medical literature.


A–C, Sagittal T1-weighted images (TR 366/TE 14), from right to left, showing a right paraspinal mass with predominant high T1 signal intensity and interspersed areas of intermediate signal intensity. The mass extends through the intervertebral foramina, causing widening of the foramina.
D, Axial T1-weighted image (TR 366/TE 14) showing a right paraspinal mass that extends through the intervertebral foramina causing widening of the foramina and scalloping of the posterior margin of the vertebral body.
E, Axial T2-weighted fast spin-echo image (TR 3400/TE 110) showing mild effacement of the right lateral aspect of the thecal sac without any significant compression.
F and G, Sagittal fat-suppressed postcontrast T1-weighted images (TR 366/TE 14) show that the mass follows the signal intensity of the subcutaneous fat. There are interspersed areas of enhancement.
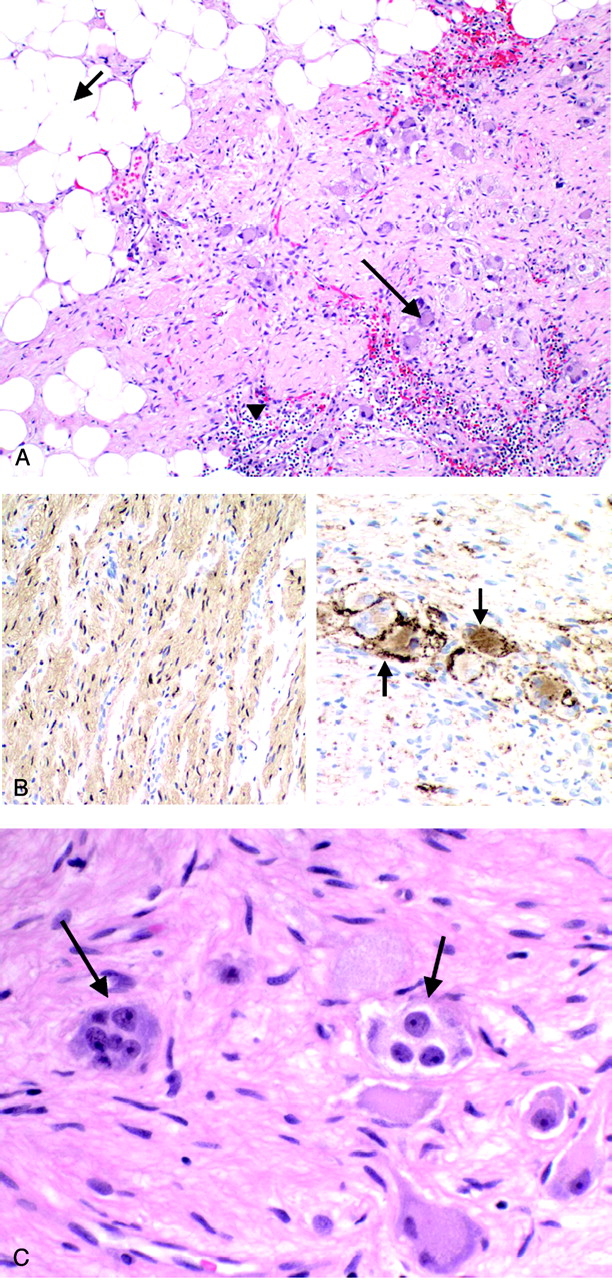
Resection of the mass entailed a thoracotomy and laminectomy from T9 to T12. The mass was adherent to the chest wall and traversed the T9, T10, and T11 intervertebral foramina. The tumor was grossly composed of areas of pale pink fibrous tissue with intermingled fatty tissue. Microscopically, ganglion cells—many multinucleated—were scattered in a background of spindle cells. Synaptophysin antibody immunostained the ganglion cells. The spindle cells were S100 immunoreactive, which confirmed that they were Schwann cells. Intermixed were clusters of mature adipocytes (Fig 2A–C). Perivascular clusters of CD45 immunoreactive lymphocytes were present. No primitive neuroectodermal cells were seen. The pathologic diagnosis was ganglioneuroma containing foci of adipose tissue.

A, Microscopic picture demonstrating adipose tissue (short arrow), Schwann cells, lymphocytes (arrowhead), and ganglion cells (long arrow); original magnification 10×.
B, On the left, S100 immunostain demonstrates that the tissue is composed predominantly of Schwann cells. On the right, Synaptophysin immunostain confirms the presence of ganglion cells (arrows); original magnification 20×.
C, High-power picture of multinucleated ganglion cells (arrows); original magnification 40×.
Discussion
Ganglioneuromas are one of a few tumors that arise from neural crest cells. This category of neoplasms also includes peripheral nerve sheath tumors, melanomas, and neuroendocrine cell tumors (2). More specifically, ganglioneuromas arise from the autonomic ganglion cells of the peripheral nervous system, usually the sympathetic ganglion. They represent the benign end of the spectrum for the ganglion cell lineage, whereas ganglioneuroblastomas and neuroblastomas comprise the malignant end of this spectrum. It is not surprising that ganglioneuromas may arise anywhere along the peripheral autonomic ganglion sites. They most commonly occur within the posterior mediastinum and retroperitoneum and less commonly in the adrenal medulla, parapharyngeal region, visceral ganglia, or cranial nerve ganglia (4, 5). They have been reported rarely in the tongue, mandible, bladder, uterus, ovary, spermatic cord, testes, prostate, and skin and bone (5). These tumors occasionally are associated with active hormone secretion, including vasoactive intestinal polypeptide, catecholamines, and testosterone (4, 5).
These tumors are grossly well-circumscribed, solid, encapsulated masses (4, 5, 11, 12) and may demonstrate calcifications (4, 10) or a whorled pattern on cut section (5). The hallmark microscopic feature of ganglioneuromas is the presence of mature ganglion cells and the absence of immature neuroblasts. The ganglion cells can be identified by their abundant eosinophilic cytoplasm, large nuclei, and prominent nucleoli. Other elements are usually seen and include Schwann cells, perineural satellite cells, axons, and collagen fibers (4, 5). Varying degrees of myxoid stroma and an interlacing pattern of Schwann cells and collagen fibers have also been reported (5, 11). These latter 2 histopathologic features seem to correlate well with imaging findings (11). Fat, which was found in our case, is an uncommon finding but has been reported elsewhere (10, 11).
Ganglioneuromas appear radiologically as well-defined, oblong masses that are located anterior and lateral to the spine. They typically span 3–5 vertebral levels (1). On CT imaging, these tumors may be homogeneous or heterogeneous masses with low to intermediate attenuation (13). Calcification has been reported in approximately 20% of cases (5, 13) and is usually punctate as opposed to the coarse pattern seen with ganglioneuroblastomas and neuroblastomas (1, 13). Following contrast administration, the tumors demonstrate mild to moderate enhancement (13).
On MR imaging, ganglioneuromas appear as homogeneous masses with low and, less commonly, intermediate signal intensity on T1-weighted images (11, 13). In contrast, on T2-weighted images, the signal intensity is usually heterogeneous and either intermediate to high or markedly high (11–13). In a series of 10 patients published by Zhang et al (11), the microscopic presence of abundant myxoid stroma was found to correlate with very high signal intensity on T2-weighted images. Also reported in this study and other sources is the finding of a whorled appearance on T1-weighted and, more commonly, T2-weighted images within the tumor that corresponds to the microscopic interlacing patterns of Schwann cells and collagen fibers (5, 11). There may be no, mild, or heterogeneous enhancement (11, 13). Ring enhancement may correspond to the capsule of the tumor (11).
Our case was unusual because the tumor demonstrated areas of high signal intensity on both T1- and T2-weighted images. Furthermore, there was low signal intensity of the mass on the fat-suppressed postcontrast images. These findings suggested the presence of a fat-containing tumor before the resection of the mass. Microscopically, the presence of adipose tissue was confirmed along with the typical features of a ganglioneuroma.
The list of fat-containing tumors found in the posterior mediastinum is shorter than the list of posterior mediastinal tumors given in the introduction. In our review of the English literature, neoplasms that have been reported within the posterior mediastinum and characterized by adipose tissue are teratomas (8, 9), parathyroid lipoadenoma (14), and other lipomatous mesenchymal tumors, including lipomas, liposarcomas (3), myelolipoma (15), and angiolipoma (16). Schwannomas, which have a similar appearance to ganglioneuromas on MR imaging, including low signal intensity on T1-weighted images and high signal intensity on T2-weighted images (1), have also been reported to contain fat (17). Other non-neoplastic masses in the posterior mediastinum with adipose tissue elements include fatty transformation of extramedullary hematopoiesis and panniculitis (10).
Ganglioneuromas (1, 5) and Schwannomas (1) are known to widen the neural foramina and extend into the spinal canal. Lipoblastomas (18) and angiolipomas (16) have also been reported to enter the spinal canal. Therefore, we conclude that the presence of fat in a posterior mediastinal mass that widens the neural foramina and enters the spinal canal narrows the differential diagnosis to a ganglioneuroma, Schwannoma, or lipomatous mesenchymal tumor.
References
- Received January 22, 2005.
- Accepted after revision April 11, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}