
Abstract
BACKGROUND: Endoscopic guided biopsy (EGB) is performed after an initial endoscopy for the investigation of patients with suspected nasopharyngeal carcinoma (NPC). The aim of the study was to determine whether MR imaging has the potential to replace invasive EGB in patients with a normal endoscopy.
PATIENTS AND METHODS: Data from 2 groups of patients was reviewed, group 1 with proved NPC for MR staging (n = 456) and group 2 with suspected NPC (n = 77). The sensitivity was calculated for group 1 and sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy for group 2.
RESULTS: In group 1, which included 118 of 456 (26%) with stage 1 disease, cancer was detected in all patients, giving a sensitivity of 100%. In group 2, MR imaging was negative for NPC in 70 (91%) patients, and no cancer has been detected on follow-up (follow-up range, 1–90 months; mean, 36 months). MR imaging was positive for NPC in 7 (9%) patients and NPC was confirmed by biopsy in 3 (4%). Two of these 3 patients had undergone negative endoscopy and biopsy before the MR imaging. NPC was not present in the remaining 4 patients, 2 of whom were found to have lymphoid hyperplasia. MR imaging had a sensitivity of 100%, specificity of 95%, NPV of 100%, PPV of 43%, and accuracy of 95%.
CONCLUSION: MR imaging has the potential to screen healthy patients who do not require EGB and direct the site of biopsy in small cancers that may be missed by endoscopy. On the basis of these results, a prospective study is planned.
In areas of the world in which nasopharyngeal carcinoma (NPC) is endemic, there is high clinical suspicion of the disease in patients who present with head and neck symptoms, as well as those with an abnormal result from an Epstein-Barr virus (EBV) serology test used to screen for the disease. Fortunately, most of these patients do not have NPC but, to exclude cancer, patients undergo endoscopy as the initial investigation often followed by endoscopic guided biopsy (EGB). The latter procedure is invasive, unpleasant, associated with a risk of hemorrhage, and usually requires a second outpatient visit. For high-risk patients, such as those with elevated blood serology, even when results of the initial endoscopy are normal, an EBG is performed to sample the nasopharynx. However, EGB can only sample a small fraction of the nasopharynx, so small mucosal or submucosal cancers may be missed. Therefore, it would be advantageous to find a less invasive investigation that could (1) screen out those healthy patients who do not require biopsy and (2) detect small tumors that would aid in directing the site of biopsies in those patients where the tumor cannot be seen on endoscopy. MR imaging is a noninvasive technique that has the potential to fulfill this role and is used routinely to stage proved cancers of the upper aerodigestive tract, including the nasopharynx,1–6 but it is not used routinely to detect cancer except in the group of patients with an unknown primary tumor, because it is generally accepted that MR imaging misses small mucosal lesions.7 However, we have gained the impression that high-resolution MR imaging performs better in detection of cancer in the nasopharynx than in other sites of the upper aerodigestive tract. The aim of this study was to review retrospectively the results of MR imaging to determine whether it has the potential to be an accurate test for detecting NPC, and especially to determine whether it can replace EGB in patients with normal results on endoscopy and MR imaging.
Methods
Patient Selection
This is a retrospective study of patients undergoing MR imaging of the head and neck between 1996 and 2005. Patients were divided into 2 groups. Group 1 consisted of patients in whom the MR imaging request form indicated that the scan was being performed for staging-proved NPC. Group 2 consisted of patients in whom the MR imaging request form indicated that the scan was being performed for the investigation of suspected NPC. Indications for such scans included persistently elevated EBV serology, persisting unexplained symptoms, such as middle ear effusions in adults, epistaxis, blood-stained saliva or rhinorrhea, and abnormal endoscopy findings with normal biopsy results.
MR Imaging Protocol
MR imaging was performed on a 1.5T MR unit (Gyroscan; Philips Medical Systems, Best, The Netherlands). In all patients, sequences included an axial fat-suppressed T2-weighted sequence (repetition time [TR]/echo time [TE], 2500 ms/100 ms; echo-train length, 15; field of view, 22 cm; section thickness, 4 mm with no intersection gap; and matrix size, 256 × 202), coronal turbo spin-echo (TR/TE, 2500 ms/100 ms; echo-train length, 14; field of view, 22 cm; section thickness, 4 mm with no intersection gap; matrix, 256 × 202), axial T1-weighted spin-echo (TR/TE, 500 ms/200 ms; field of view, 22 cm; section thickness, 4 mm with no intersection gap; matrix, 256 × 202) and contrast-enhanced T1-weighted spin-echo images with the use of a 512 × 512 matrix in the axial and coronal planes after a bolus injection of 0.1 mmol/kg gadopentate dimeglumine (Schering, Berlin, Germany).
Data Analysis
In group 1, the MR imaging reports were reviewed to determine whether NPC could be identified. In those patients in whom NPC was identified, the stage of the primary tumor was recorded (Table 1). In those patients in whom the tumor could not be identified, the clinical records were reviewed. In group 2, an experienced head and neck radiologist reviewed the MR imaging scans. Each scan was scored from 1 to 5 (Table 2). For the purpose of the study, 1–3 was considered negative for NPC and 4–5 was considered positive. The clinical records were reviewed to determine the clinical indication for the MR imaging, the results of endoscopy and biopsy, and the length of the follow-up period in those patients in whom NPC was not identified.
T-stages as established by American Joint Committee on Cancer
MRI scoring system and MRI results for 77 patients with suspected NPC (group 2)
Statistical Analysis
The sensitivity (groups 1 and 2) and the specificity, negative predictive value (NPV), positive predictive value (PPV), and accuracy (group 2) of MR imaging for the detection of NPC were calculated by using the biopsy results as the reference standard.
Results
Group 1: NPC Proved at the Time of MR Imaging
The MR imaging data were available for analysis in 458 patients (323 men, 135 women; mean age, 51 years; range, 21–94 years). Nasopharyngeal carcinoma was detected in 456 of 458 patients. Review of the clinical notes in the 2 patients in whom NPC could not be detected revealed that the patients had undergone treatment with radiation therapy before the scan. Therefore, NPC was detected in 456 of 456 patients, producing a sensitivity of 100%. The T stage of these tumors is shown in Table 3, and a small T1-stage tumor is shown in Fig 1.

Axial T1-weighted MR image postcontrast of the nasopharynx of a patient with proved NPC (group 1) undergoing staging with a small cancer confined to the left side of the nasopharynx (arrows) (stage T1).
T-stage of 456 patients with proved nasopharyngeal carcinoma (group 1)
Group 2: NPC Suspected at the Time of MR Imaging
The MR imaging scans and clinical records were available in 77 patients (29 men, 48 women; mean age, 47 years; range, 18–84 years). Indications for MR imaging were abnormal EBV serology results in 17 of 77 (22%) or symptoms in the head and neck in 60 of 77 (78%), such as cervical lymphadenopathy, epistaxis, hearing loss, tinnitus, and nasal obstruction. MR imaging was negative (grade 1–3) in 70 of 77 (91%), and positive (grade 4–5) in 7 of 77(9%). Details are shown in Table 4. For the 70 patients with negative results after MR imaging (Fig 2), no cancer was identified (follow-up period, 1–90 months; mean, 36 months). For the 7 patients with a positive MR imaging, NPC has been confirmed by biopsy in 3 of 77 (4%). Two of these 3 patients had undergone at least one negative endoscopy and biopsy before the MR imaging (Fig 3, A, B). In the remaining 4, patients biopsies were negative for cancer. In 3 of these 4 patients, the changes were diffuse; in 2 of these, the biopsy revealed lymphoid hyperplasia (Fig 4, A, B). In 1 of the 4 patients with a false-positive result, the abnormality was focal, but the biopsy, performed after the MR imaging, together with follow-up for 16 months, showed no evidence of NPC. MR imaging had a sensitivity of 100%, specificity of 95%, NPV of 100%, PPV of 43%, and accuracy of 95%.

Axial T1-weighted contrast-enhanced MR image of a patient with suspected NPC (group 2) with a normal nasopharynx (arrows show normal enhancing mucosa).

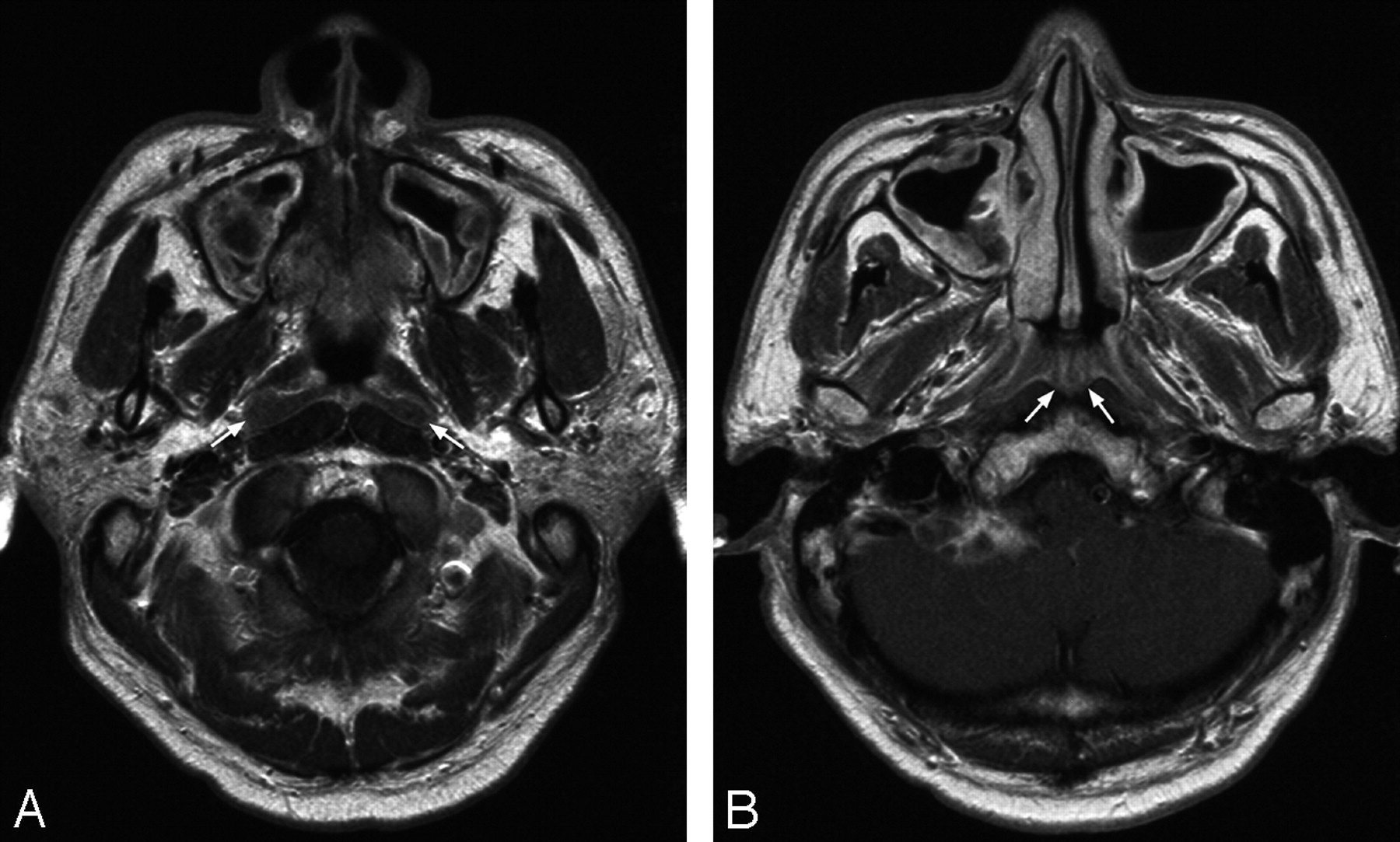
Axial T1-weighted contrast-enhanced MR image of the nasopharynx in 2 patients with suspected NPC (group 2) where cancer was initially missed by endoscopy and biopsy but identified by MR imaging. Patient with a small cancer in the left fossa of Rosenmuller (arrows) (stage T1) (A) and patient with a small cancer over the torus tubarius (arrows) (stage T1) (B).

Axial T1-weighted contrast-enhanced MR image of the nasopharynx in a patient with suspected NPC (group 2) where MR imaging incorrectly diagnosed cancer that was later shown by biopsy to be lymphoid hyperplasia. A, Section at the level of the fossa of Rosenmuller shows mucosal abnormality in the fossa bilaterally (arrows), giving the false-positive result on MR imaging for cancer.
B, Section at the level of the roof shows the “striped” appearance of normal lymphoid tissue in the adenoids (arrows).
Results of MRI in 77 patients with suspected NPC (group 2)
Discussion
The study was designed to determine whether MR imaging is accurate in detecting NPC. The main impetus behind the study is the increasing number of normal patients undergoing EGB. One of the main reasons for this increase was the introduction of an EBV blood test screening for those at high risk of NPC because of a family history of the disease. There are several serologic tests related to EBV that are used to screen for NPC. The most widely used are the IgA antibody titers to EBV capsid antigen IgA (EBV IgA-VCA), which has a sensitivity of 81%–93% and a specificity of 80%–96%.8–10 The result of EBV IgA-VCA is often combined with the result of IgA antibody titers to EBV early antigen (EBV IgA-EA), which, though it has a lower sensitivity, has a higher specificity. However, when applied to screening populations, rather than tertiary referral centers, these tests have a high false-positive rate. In 1 such study by Ng et al,11 in which patients with a family history of NPC were screened, 9% of all patients had a positive test but only 11% of these had NPC. This means that 8% of all patients screened had a false-positive blood test. EBV DNA seems to increase the accuracy of the blood test9,12,13; as yet, it has been mainly assessed in tertiary referral centers rather than screening populations.
Unfortunately, approximately 6% of NPC is believed to lie in a submucosal region and cannot be seen by the endoscope. As a result, patients with a high degree of suspicion of NPC, including those with abnormal EBV serology, undergo EGB biopsy to sample the nasopharynx in an attempt to identify occult cancer. MR imaging is a noninvasive and has the potential to screen healthy patients, sparing them from undergoing EGB. To do this, MR imaging has to be very sensitive, especially because NPC is highly responsive to treatment with a good prognosis when identified at an early stage.
In group 1, which included patients with T1 stage disease, MR imaging had a sensitivity of 100%. These results are encouraging and confirm our impression that MR imaging is better at detecting cancer in the nasopharynx than at other sites of the upper aerodigestive tract. However, there is a very strong bias in this group because the diagnosis of NPC was already known. In addition, it is possible that patients with very small T1 tumors were not referred for MR imaging staging so that even patients with T1 stage disease had a bias toward larger cancers.
Therefore, we reviewed the results of MR imaging in patients with suspected NPC only. Once again, the results were encouraging with a sensitivity of 100%. So far, no patients with a normal MR imaging results have been found to have NPC. In addition, MR imaging was able to detect cancers in 3 patients (4% of cases). In 2 of these patients, the tumors were very small and had not been detected by endoscopy or EGB. We feel that MR imaging has the potential not only to screen those healthy patients who do not need EGB but also to detect small tumors that are not detectable on current investigations.
For MR imaging to decrease the number of patients undergoing EGB, it also has to have a high specificity. Other cancers of the nasopharynx are uncommon, and the main differential diagnosis of NPC is normal lymphoid tissue. This tissue is usually concentrated in the adenoids in the roof of the nasopharynx and is very prominent in childhood and adolescence but decreases with age. MR imaging usually is able to distinguish lymphoid tissue in the adenoids from a mass because of the “stripes” that are identified on the T2-weighted and T1-weighted sequences with contrast enhancement. As a result, the specificity of MR imaging was high (95%) because lymphoid tissue in the adenoids was not mistaken for NPC. In 2 cases, there was abundant lymphoid tissue that not only involved the adenoids in the roof of the nasopharynx but also extended down the walls into the fossa of Rosenmuller bilaterally, giving the false impression of a carcinoma. This contributed to the low PPV of MR imaging, but because the overall number of patients with false-positive results was low MR, imaging could substantially reduce the number of patients who undergo EGB.
The current study has obvious limitations because of its retrospective nature and the bias in the 2 groups, the first toward those with cancer and the second to those without. It is still unknown whether MR imaging will be sensitive to very small tumors. However, the high overall sensitivity and specificity in this study, including the detection of early tumors that were missed with endoscopy, is encouraging. MR imaging has the potential to be used in patients with suspected NPC to replace EGB in patients with normal MR imaging and endoscopy or direct the site of EGB in patients with small cancers detected only by MR imaging. On the basis of these results, we are planning a prospective study to determine the accuracy of MR imaging in the detection of NPC.
References
- Received August 29, 2005.
- Accepted after revision October 31, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Early Detection of Cancer: Evaluation of MR Imaging Grading Systems in Patients with Suspected Nasopharyngeal Carcinoma
- Optimal Mass Transport Kinetic Modeling for Head and Neck DCE-MRI: Initial Analysis
- MR Imaging Criteria for the Detection of Nasopharyngeal Carcinoma: Discrimination of Early-Stage Primary Tumors from Benign Hyperplasia
- Detection of Nasopharyngeal Carcinoma by MR Imaging: Diagnostic Accuracy of MRI Compared with Endoscopy and Endoscopic Biopsy Based on Long-Term Follow-Up
- Diagnostic Accuracy of Sonography Versus Magnetic Resonance Imaging for Primary Nasopharyngeal Carcinoma
- Imaging of the pharynx and larynx
- Imaging of the pharynx and larynx