
Abstract
SUMMARY: We present an unusual case of a complete first branchial cleft fistula communicating between the external auditory canal and the skin near the angle of the mandible. CT and fluoroscopic fistulography were used to establish the presence and course of the tract and to assist in surgical planning. The embryology and classification of first branchial cleft anomalies are discussed, with emphasis on the impact of imaging.
First branchial cleft anomalies represent a small subset of congenital malformations in the head and neck, composing fewer than 8% of all branchial cleft defects.1 The annual incidence of first branchial cleft anomalies has been reported as 1 per 1 000 000.2 These anomalies are believed to be the result of incomplete obliteration of the clefts that arise between the branchial arches during embryogenesis, producing a persistent anomalous structure.3 Considerable variation exists in the anatomic course of the final structure. This high degree of variability has prompted the use of several different classification schemes, by using anatomic position, number of openings, or type of tissue lining the tracts.1,4,5 Thus, imaging of a first branchial cleft anomaly is critical for proper classification and for surgical planning.
We report a case of a first branchial cleft fistula communicating between the external auditory canal (EAC) and skin near the angle of the mandible, emphasizing the impact of imaging on diagnosis and treatment.
Case Report
A healthy 61-year-old woman presented with drainage from the skin of her left neck. She stated that she always had a small pit in this location but that it had been free of drainage until recently. She attributed the drainage to the use of ear drops for treatment of otitis externa several weeks earlier, but the drainage had persisted after the treatment was completed. Physical examination revealed a 1-mm pit just below the angle of the left mandible. A small amount of thick white debris could be expressed from the site. There was a 5-mm cavity on the anteroinferior aspect of the EAC, just lateral to the bone-cartilage junction.
The patient first underwent fluoroscopic evaluation to determine the extent of the neck lesion. The pit on the side of the neck was cannulated with a 20-gauge angiocatheter. Diatrizoate meglumine (Renografin 60) was infused through the angiocatheter under fluoroscopic visualization.
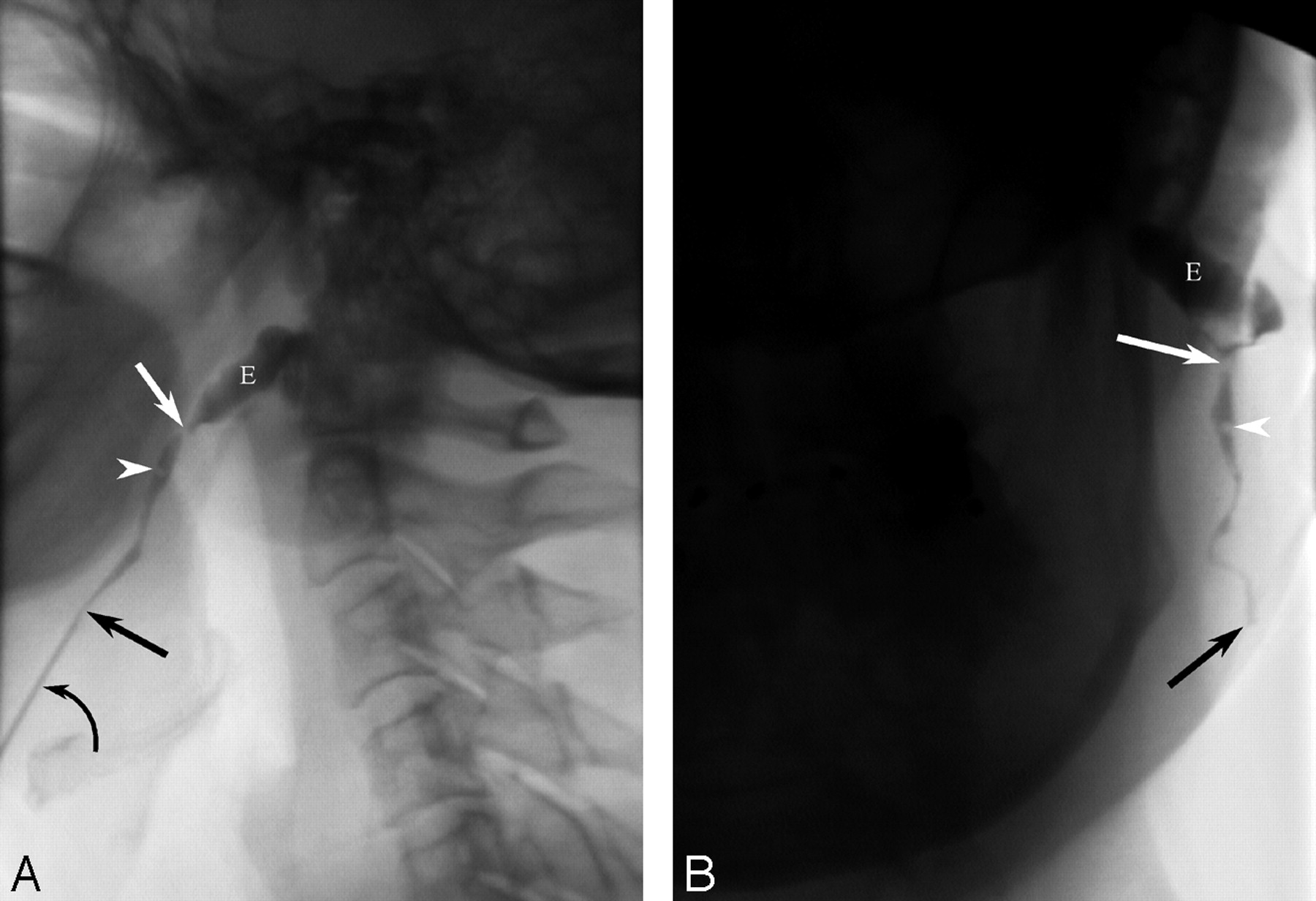
There was prompt filling of a tract that extended from the skin overlying the angle of the mandible into the cavity in the EAC (Fig 1). The tract had a variable diameter of approximately 2 mm. From the opening on the patient’s neck, the tract coursed superiorly for approximately 5 mm, then medially for approximately 5 mm, and then extended superoposterior to its junction with the EAC. A small filling defect was present in the upper aspect of the tract, possibly the result of scar tissue or a small polyp. The tract was mildly stenosed immediately before its connection to the EAC.

Fluoroscopic fistulogram of a first branchial cleft anomaly. Lateral (A) and frontal (B) projections demonstrate the course of the fistulous tract from the skin overlying the angle of the mandible (black arrow) to the external auditory canal (white arrow). The external auditory canal is filled with contrast (E). Note the small filling defect (arrowhead) in the midportion of the anomaly. The angiocatheter remains in position on the lateral projection (curved arrow).
The patient was taken to the CT scanner, and additional Renografin 60 was infused with the patient in the CT scanner. Select unenhanced axial images of the upper neck were obtained (Fig 2). The fistulous tract was seen to travel through the subcutaneous fat of the neck and through the superficial lobe of the parotid gland. From the imaging, the treating otolaryngologist informed the patient of the potential risk of facial nerve injury as a complication of surgical resection. The patient opted to defer surgery to avoid any possible injury to the facial nerve.

CT fistulogram. Axial CT images (kV = 120, mA = 120, thickness = 1.25 mm) without intravenous contrast are shown from superior (A) to inferior (F). Contrast material is seen within the first branchial cleft tract (arrow). The relationships of the tract to the parotid gland and the retromandibular vein (arrowhead) are well defined for ease of surgical planning. A, Contrast is seen spilling into the external auditory canal (E). B, Just below the external auditory canal, the tract passes into the parenchyma of the parotid gland. C, The tract traverses the gland, running superficial to the retromandibular vein. D, Streak artifact from dental amalgam degrades the image as the tract passes through the parotid capsule into the subcutaneous fat. E, The tract continues inferiorly within the subcutaneous fat. F, The tract exits the skin at the level of the mandibular angle.
Discussion
The branchial arches are the embryologic precursors of the ear and the muscles, blood vessels, bones, cartilage, and mucosal lining of the face, neck, and pharynx. They exist transiently as 6 paired neck structures during the fourth through seventh weeks of embryonic development. These 6 arches are separated by 5 clefts externally and 5 pouches internally. By the seventh week of development, the arches fuse and the clefts are obliterated. The structures derived from the first branchial cleft are the cavum conchae, the EAC, and the external layer of the tympanic membrane.6 First branchial cleft anomalies result from incomplete fusion of the ventral portions of the first and second arches.2,6 During development, closure of the clefts is concurrent with the emergence of the developing parotid gland and migration of the facial nerve, which originates from the second branchial arch; thus, first branchial cleft anomalies are typically closely related to these structures.6
Numerous schemes for classification of first branchial cleft lesions have been suggested. Most commonly, lesions have been characterized by the degree of closure of the cleft that has occurred in the following manner: a fistula (open communication between skin and a mucosal surface), a sinus (a single opening onto skin or mucosa), or a cyst (no communication with skin or mucosa). With this system, fistulas occur slightly more commonly (52%) than sinuses (48%).1 Cysts are least common, and there is debate as to their true embryonic origin.7
Other classification schemes focus on the tissue type lining the tract: Type I contains ectoderm, whereas type II has both ectoderm and mesoderm.4,5 Still other schemes rely on the location of the anomaly: Type I is adjacent to the EAC, whereas type II is at the angle of the mandible.
First branchial cleft anomalies are also described by the anatomic location of the opening and the course of the tract. Common sites of external opening of fistulas and sinuses are the EAC (40%), upper neck (32.5%), concha (20%), and posterior auricular area (7.5%).1 The course of fistulous tracts relative to the facial nerve can be superficial (41%), deep (37%), or between the branches (22%).1 This is in contrast to sinus tracts, which favor a superficial course (76%).1 The close relationship of first branchial cleft anomalies to the facial nerve results in frequent complications from surgical treatment.
Patients with first branchial cleft anomalies most commonly present with swelling in the cervical (35%), parotid (35%), or periauricular (24%) regions.3,8 Lesions often demonstrate purulent drainage from infection or epithelial desquamation. First branchial cleft anomalies are seen approximately twice as often in women (69%) as in men (31%).1 Fistulas occur more frequently on the left side (64%); sinuses show no side preference.1 These malformations are frequently misdiagnosed as benign parotid tumors or innocent superficial sinuses or cysts; this error contributes to a long clinical course and delays in diagnosis and treatment.2,4 Adding to the difficulty of diagnosis is the lack of association between these anomalies and other facial malformations.3
Surgical excision of the entire tract and, in some cases, resection of a small amount of skin and cartilage within the EAC, are the treatments of choice and usually result in permanent cure.8 Recurrence occurs if the malformation is not excised along its entire course.1 Thus, it is critical for the surgeon to understand the extent of the lesion and the course of any fistulas or sinus tracts. Treatment typically requires parotidectomy with facial nerve exposure. Even when the facial nerve is identified and monitored, facial nerve injury is a recognized complication (18% temporary, 1% permanent).1 Treatment may also be complicated by chronic infection and ineffective prior surgical excision.8
The high variability in the course of these lesions and the necessity of complete excision during treatment makes radiographic visualization crucial to directing treatment. Despite this, there are few reports of radiographic analyses of first branchial cleft anomalies.2,9 Our case, in which CT and fluoroscopy demonstrated a superficially located fistulous tract between the EAC and angle of the mandible, exemplifies the utility of radiographic studies in establishing the diagnosis and planning treatment for first branchial cleft anomalies.
Conclusions
First branchial cleft anomalies are rare congenital malformations that are often misdiagnosed and mismanaged. Although they are most commonly encountered in children, they may also present in adults. CT and fluoroscopic studies can be instrumental in minimizing surgical complications by establishing a definitive diagnosis and directing treatment.
References
- Received September 12, 2005.
- Accepted after revision October 26, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}