
Abstract
SUMMARY: We present an unusual case of acquired secondary syphilis manifesting as osteomyelitis of the skull in a patient with a history of human immunodeficiency virus infection, evaluated by CT, volumetric CT reconstructions, and MR imaging.
Bone and joint involvement is a rare complication of primary and secondary syphilis. After declining annually from 1990 through 2000, the trend of primary and secondary syphilis in the United States has now reversed, increasing 12.4% in 2002.1 With this resurgence, syphilitic osteitis and osteomyelitis are likely to become more common presentations of early-stage syphilis. We describe a case of acquired syphilitic involvement of the calvaria in an immunodeficiency virus infection–positive (HIV+) patient with documented syphilis infection.
Case Report
A 40-year-old man with a history of HIV infection and non-Hodgkin lymphoma presented with a 2-month history of headache. On physical examination, a palpable 2-cm tender nodule was noted at the midline frontal vertex. The patient was afebrile and reported no trauma or weight loss.
Noncontrast head CT demonstrated 3 unusual lytic lesions within the frontal vertex, right frontal bone, and right parietal bone (Fig 1). The lesions exhibited a “worm-eaten” appearance of irregular bone destruction, best delineated on volume-rendered 3D reconstructions. There was adjacent abnormal scalp soft tissue along the outer table.

CT images of the vertex calvaria. A, Axial CT image (2.5-mm section thickness) demonstrates irregular bone destruction involving the calvaria. The outer cortex is predominantly involved. Irregular channel-like areas of bone destruction are best demonstrated in the vertex lesion (arrow). B, 3D volume-rendered image (using 2.5-mm reconstructed images) demonstrates the irregular worm-eaten nature of the destructive lesions, characteristic of syphilitic osteomyelitis. (arrows).
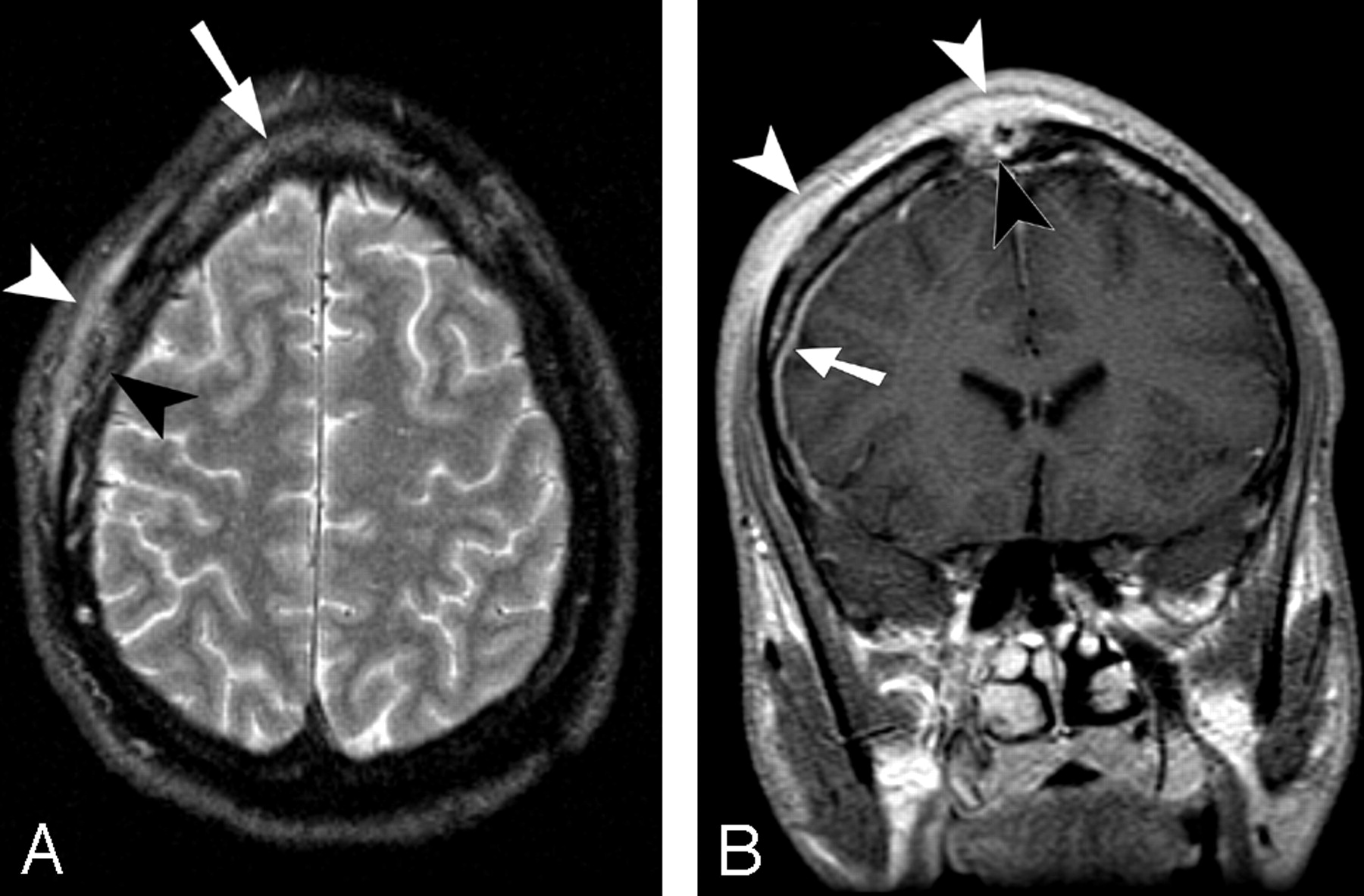
MR imaging of the brain was performed without and with the administration of gadolinium, by using a 1.5T system. Irregular zones of increased signal intensity on T2-weighted images and enhancement were identified in the calvaria, corresponding to the lytic lesions seen on CT. More diffuse areas of calvarial edema signal intensity were also seen adjacent to the destructive lesions. There was associated mild dural enhancement along the right convexity (Fig 2). No brain parenchymal abnormalities were identified.

A, Axial fast spin-echo (FSE) T2-weighted image with fat saturation (TR, 3300 ms; TE, 86.4 ms; echo-train, 12). B, Coronal spin-echo T1-weighted image (TR, 400 ms; TE, 8.0 ms) after gadolinium administration (20 mL). Axial FSE T2-weighted image (A) demonstrates abnormal marrow edema in the frontal bone (arrow). There is subgaleal/periosteal inflammatory tissue adjacent to the right frontal destructive lesion, which exhibits increased signal intensity on T2-weighted image (A, white arrowhead). The bone destruction is irregular and predominantly involves the outer cortex (A, black arrowhead). The vertex lesion enhances intensely, involving nearly the entire thickness of the calvaria (B, black arrowhead). Mild dural enhancement is noted along the right convexity (B, arrow), consistent with inflammatory involvement. The adjacent subgaleal/periosteal inflammatory process enhances intensely (white arrowheads). No parenchymal signal-intensity abnormalities are identified.
Neoplastic and infectious causes were initially considered. Bone scintigraphy demonstrated multiple areas of increased uptake corresponding to the osseous lesions.
A right frontal parasagittal craniectomy and excision of the right frontal bone lesion were performed. Findings of pathology demonstrated cortical and trabecular bone, with an attenuated inflammatory infiltrate composed largely of lymphocytes and plasma cells. Warthin-Starry silver stain as well as gram, fungal, and acid-fast bacilli smears were negative for microorganisms. There was no evidence of a neoplastic process.
A reactive quantitative rapid plasma reagin (RPR) titer measured 1:128, and a fluorescent treponemal antibody absorption test was positive. The patient was treated with intravenous penicillin G, 4 million units every 4 hours for 6 weeks. Headaches resolved and the palpable lesion disappeared. The RPR titer dropped to 1:32 6 weeks after treatment. These findings clinically confirmed the diagnosis of syphilitic osteomyelitis.
Discussion
Syphilis is a chronic systemic infectious disease caused by the spirochete Treponema pallidum. In acquired syphilitic infection, the organism has an incubation period lasting about 3 weeks, after which the disease exhibits 4 classically described clinical stages. In the primary stage, infection is characterized by a nonpainful skin lesion (chancre) that is usually associated with regional lymphadenopathy and initial bacteremia. A secondary bacteremic or disseminated stage is associated with generalized mucocutaneous lesions, lymphadenopathy, and a variable array of clinical findings. Latent syphilis, having no clinical manifestations, is detected only by reactive serologic tests. A late or tertiary stage occurs in up to one third of untreated patients 10–30 years later, with typical involvement of the ascending aorta and central nervous and skeletal systems.2
The diagnosis of syphilitic osteitis is usually suspected because of the presence of either mucocutaneous findings or generalized lymphadenopathy, both lacking in our patient. Conventional radiographs typically show round osteolytic areas with demineralization or sclerosis of the outer table and diploe, with less involvement of the inner table.3,4
Destructive bone lesions are rare complications of early-stage syphilis. In the largest case series, Reynolds and Wasserman5 identified only 15 patients with destructive bone lesions in 10,000 cases of early syphilis from 1919 to 1940. However, because the clinical presentation is often nonspecific, the diagnosis can be overlooked in the absence of other syphilitic symptoms. Thompson and Preston3 performed skull radiographs on 80 patients with secondary syphilis and found 7 with osteolytic lesions, only 4 of whom had headache.
In our patient, CT demonstrated an irregular destructive process, preferentially involving the outer table, with an unusual worm-eaten appearance. This morphology is characteristic of calvarial syphilitic involvement on conventional radiographic, gross pathologic, and paleopathologic assessment.3,4,6–8
The response of the bone to spirochete infection in early-acquired syphilis depends on the organism virulence, host inflammatory response, and region of bone (periosteum, cortex, medullary cavity) involved.9 In early-acquired syphilis, the secondary spirochetemia that results after primary infection can lead to infection and involvement of the deeper vascular areas of the periosteum. with production of perivascular inflammatory infiltrates and highly cellular granulation tissue. The inflammatory process extends into the Haversian canals, with resultant osteitis and osteomyelitis.9 The medullary canals enlarge with increasing osteolysis. With continued inflammation and bone lysis, an irregular macerated appearance of the bone results, as demonstrated in our patient. New bone formation can occur, sometimes in a prominent manner, typically along the periphery of the lesion.3,6,7
MR imaging demonstrates the marrow space involvement, the periosteal process, and degree of intracranial extension more completely than CT. Only 1 report of MR imaging findings in acquired syphilitic osteitis of the calvaria has been published in the clinical literature.10 In the single MR image published in that clinical report, the lesion had similar characteristics to the MR imaging findings in our patient, with a focal enhancing calvarial lesion and adjacent enhancing soft-tissue abnormality in the scalp.
The presence of organisms on biopsy material is variably seen and is less common in late-stage disease. One report notes that spirochete visualization by dark field microscopy is present in only 50% of biopsied cases of bone involvement in early-stage syphilis.11
The effect of coexistent HIV infection on the natural course of syphilis is not well understood. Johns et al12 suggested an accelerated progression of late complications such as neurosyphilis. Yet in a retrospective study of 700 patients with early syphilis, Hutchinson et al13 demonstrated no increase in neurologic complications in those patients with HIV infection. Conceivably, the clinical presentation of syphilis may be more aggressive or atypical in patients with concurrent HIV infection, given the impairment of cell-mediated immunity. Confounding medical conditions, such as the history of non-Hodgkin lymphoma in our patient, and lack of other syphilitic manifestations may make the diagnosis even more challenging.
Although symptomatic relief after therapy is typically rapid, the osseous lesions in early-phase syphilis resolve more slowly and can persist for up to 7–11 months.5,6 With proper therapy, there can be complete conventional radiographic and imaging resolution of lesions, with little residual abnormality.5,10
Lytic calvarial lesions can have a broad differential diagnosis. The possibility of syphilis should be considered in at-risk patients, given the recent increase in disease rates. The unusual irregular worm-eaten morphology of osseous destruction is characteristic and can be well visualized by volume-rendered CT representations. A nonreactive serum RPR is sufficient to exclude the diagnosis. Early recognition will result in prompt therapy of this treatable condition.
References
- Received January 10, 2006.
- Accepted after revision January 30, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Osteomyelite syphilitique chez un patient presentant des cephalees et des lesions lytiques
- Syphilitic osteomyelitis in a patient with headache and lytic lesions
- Calvarial disease in secondary syphilis presenting as headache
- Teaching NeuroImages: Skull and dural lesions in neurosyphilis
- Syphilis: an unusual manifestation?