
Abstract
SUMMARY: It is of utmost importance to avoid errors and subsequent complications when performing neurointerventional procedures, particularly when treating low-risk conditions such as unruptured intracranial aneurysms. We used endovascular treatment of unruptured intracranial aneurysms as an example and took a survey-based approach in which we reached out to 233 neurointerventionalists. They were asked what they think are the most important points staff should teach their trainees to avoid errors and subsequent complications in endovascular treatment of unruptured intracranial aneurysms. One hundred twenty-one respondents (51.9%) provided answers in the form of free text responses, which were thematically clustered in an affinity diagram and summarized in this Practice Perspectives. The article is primarily intended for neurointerventional radiology fellows and junior staff and will hopefully provide them the opportunity to learn from the mistakes of their more experienced colleagues.
A smart man makes a mistake, learns from it, and never makes that mistake again. But a wise man finds a smart man and learns from him how to avoid the mistake altogether.
Roy H. Williams
As neurointerventional fellows, we are bound to make mistakes. Human errors in neurointervention occur in up to 12% of cases,1 and they are, to some degree, unavoidable, but mentorship can prevent some of them from happening. The weighing of treatment risks and benefits is of particular importance for low-risk conditions such as unruptured intracranial aneurysms, in which complications weigh heavily on the neurointerventionalist. Thoughtful mentors will share their experiences and, most important, their errors and failures with us so that we can learn from their mistakes. What do experienced neurointerventionalists wish they had been told as fellows? We used endovascular treatment of unruptured intracranial aneurysms as an example and took a survey-based approach in which we reached out to 233 neurointerventionalists to answer this question (mostly senior staff; for detailed demographics and countries of survey participants see Online Tables 1 and 2). Participants were asked the most important points staff should teach their trainees to avoid complications in endovascular treatment of unruptured intracranial aneurysms. One hundred twenty-one respondents (51.9%) provided answers in the form of free text responses, which were thematically clustered in an “Affinity Diagram” (Online Appendix). This format was deliberately chosen to avoid narrowing the responses down to certain topics by suggesting topics or providing examples. The free text answers were then screened, and it was determined whether they contained ≥1 thematically distinct message. If the latter was the case, the response was split accordingly. Responses were then manually clustered by identifying common themes. Thematically similar responses were clustered together. Those clusters with the largest number of responses were extracted and formed the basis for the article. They are shown in the Table and summarized below (for key recommendations, see also the Figure).
Summary of the most common response clusters with exemplary responses

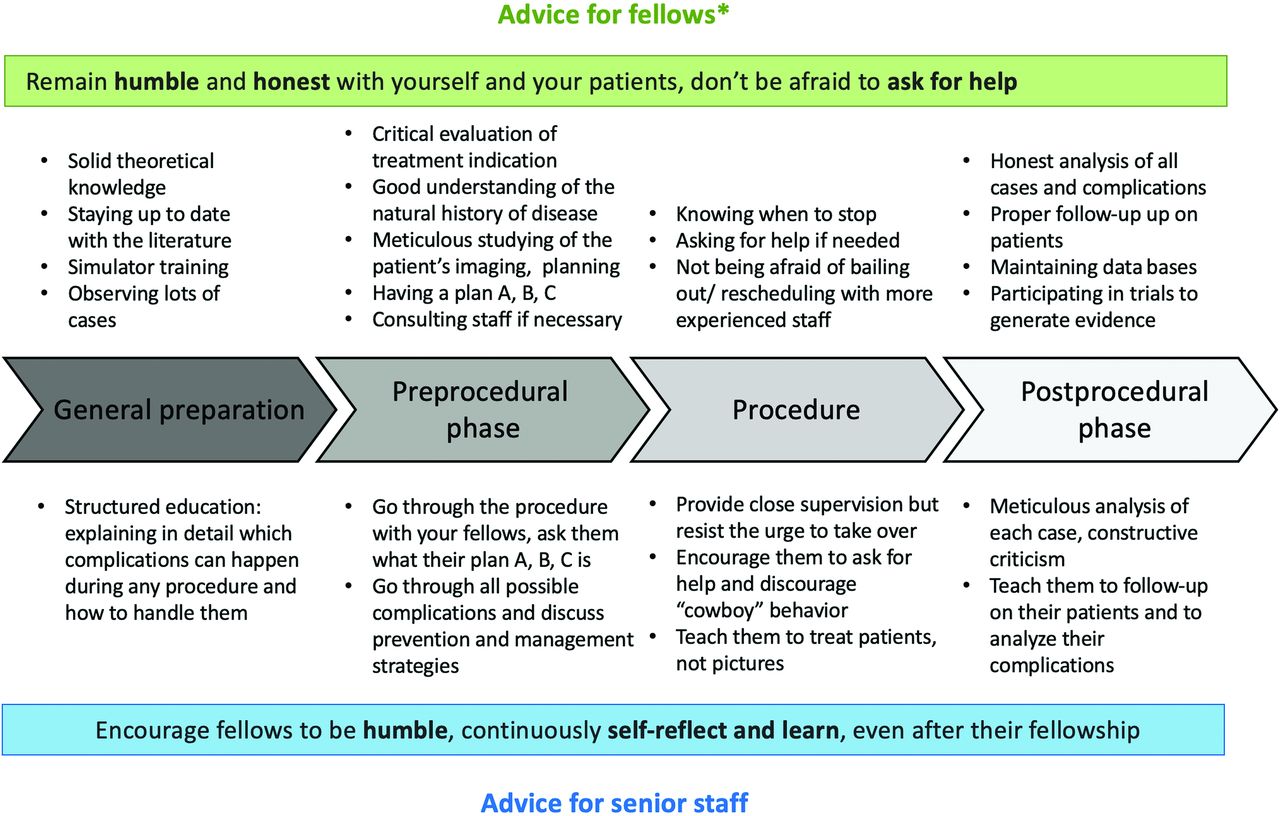
Key recommendations for fellows and senior staff on how to avoid complications in endovascular treatment of unruptured intracranial aneurysms regarding general preparation, preprocedural, intraprocedural, and postprocedural phases. The asterisk indicates that this advice also applies to junior staff.
Asking for Help
Neurointerventional skills are learned progressively, and a realistic and honest appraisal of one’s own skillset and limitations was considered crucial by most respondents. Fellows should know when to refer a case to a more experienced colleague and never be hesitant to reach out to colleagues for help and advice; not doing so means putting the patient at risk.
Many responses emphasized the importance of honestly discussing and revisiting complications and their management in an open and nonjudgmental environment,2 be it in morbidity and mortality rounds,3 interaction with colleagues,4 or professional society meetings.
Treatment Indication
Ensuring successful treatment requires picking the right patients in the first place. Participants advised fellows to perform a thorough risk-benefit analysis before every treatment decision. Knowing which cases not to treat in the early years of practice was considered key knowledge for fellows.5 Proper review of noninvasive imaging to anticipate and prevent potential complications and planning of alternative strategies, “having a plan A, B, and C” as one of the respondents stated, was thought to be essential to handle unexpected events.
The goal is to ensure that patients receive the best possible treatment, be it endovascular, surgical, or conservative (“watch and wait”), and this will require an open and unbiased discussion among physicians from different medical specialties, including diagnostic and interventional neuroradiology, neurosurgery, and neurology.
Simulation Training and Standardized Procedural Steps
Simulation training constitutes a safe environment to practice technical skills.6-10 Physicians believed that fellows should train as much as possible in a simulation environment to learn basic catheter skills before performing real cases. Standard operating procedures for every procedure step, close adherence to protocols for the management of intraprocedural complications, and choosing the simplest treatment approach possible were additional points physicians considered of high importance.11
Safety
Using a few devices well was thought to be much wiser than the use of a wide variety of new devices, for which safety and efficacy data are often limited: “keeping it as simple and safe as possible,” as many of them put it. Accepting imperfection and avoiding unnecessary and dangerous perfectionist steps toward the end of a procedure were perceived crucial for fellows: “If you think that you can put one more coil, this is [the] time to stop.”
Humans make mistakes, and they make them frequently. Neurointervention is no exception to this rule, and the stakes are high. The advice summarized in this article (see the Figure for key recommendations for fellows and senior staff) is intended to help fellows and junior staff “to be wise” as Roy H. Williams put it—that is, to learn from the mistakes of their more experienced colleagues.
Footnotes
Disclosures: Mayank Goyal—RELATED: Consulting Fee or Honorarium: Mentice, Comments: advice on acute stroke intervention; UNRELATED: Consultancy: Stryker, Medtronic, MicroVention; Patents (Planned, Pending or Issued): GE Healthcare, Comments: licensing agreement for systems of acute stroke diagnosis. Jens Fiehler—UNRELATED: Consultancy: Acandis, Cerenovus, Medtronic, MicroVention, Stryker, Penumbra; Grants/Grants Pending: Acandis, Cerenovus, Medtronic, MicroVention, Stryker, Route94*; Stock/Stock Options: Tegus; OTHER RELATIONSHIPS: CEO Eppdata. Wim van Zwam—UNRELATED: Payment for Lectures Including Service on Speakers Bureaus: Cerenovus, Stryker,* John H. Wong—UNRELATED: Stock/Stock Options: Fluid Biotech Inc, Comments: Cofounder and CEO of Fluid Biotech Inc. Johanna M. Ospel—UNRELATED: Grants/Grants Pending: Gottfried und Julia Bangerter Rhyner Stiftung, University of Basel Research Foundation, Freiwiliige Akademische Gesellschaft Basel, Comments: research scholarships. *Money paid to the institution.
References
- Received June 12, 2020.
- Accepted after revision July 31, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.