
Abstract
SUMMARY: A health care crisis such as the coronavirus disease 2019 (COVID-19) pandemic requires allocation of hospital staff and resources on short notice. Thus, new and sometimes less experienced team members might join the team to fill in the gaps. This scenario can be particularly challenging in endovascular stroke treatment, which is a highly specialized task that requires seamless cooperation of numerous health care workers across various specialties and professions. This document is intended for stroke teams who face the challenge of integrating new team members into endovascular stroke-treatment workflows during the COVID-19 pandemic or any other global health care emergency. It discusses the key strategies for smooth integration of new stroke-team members in a crisis situation: 1) transfer of key knowledge (simple take-home messages), 2) open communication and a nonjudgmental atmosphere, 3) strategic task assignment, and 4) graded learning and responsibility. While these 4 key principles should generally be followed in endovascular stroke treatment, they become even more important during health care emergencies such as the COVID-19 pandemic, when health care professionals have to take on new and additional roles and responsibilities in challenging working environments for which they were not specifically trained.
ABBREVIATIONS:
- COVID-19
- coronavirus disease 2019
- EVT
- endovascular treatment
- ICU
- intensive care unit
The coronavirus disease 2019 (COVID-19) pandemic requires allocation of hospital staff and resources on short notice. As a consequence, new and sometimes less experienced team members might join the team to fill in the gaps. This scenario also applies to endovascular stroke treatment (EVT) workflows in the neuroangiography suite and post-EVT stroke care in the neuro-intensive care unit (Neuro-ICU) and stroke unit. There are several reasons why new members might join EVT teams. For example, stroke team members with ICU experience might be redeployed to an ICU and have to be replaced, or team members might be quarantined because they had close contact with a patient with COVID-19. Integrating new staff into EVT workflows is particularly challenging, given the time-critical nature of the disease, the need for seamless interdisciplinary and interprofessional cooperation, and the highly specialized skill sets of different team members.
This document is intended for stroke teams who face the challenge of integrating new staff into their EVT workflows during the COVID-19 pandemic or any other global health care emergency. It discusses strategies for smooth integration of new stroke-team members into EVT workflows in a crisis situation in 3 different settings: 1) the neuroangiography suite, 2) the Neuro-ICU ward, and 3) the stroke unit. The 4 overarching principles are the following: 1) transfer of key knowledge (simple take-home messages), 2) open communication and a nonjudgmental atmosphere, 3) strategic task assignment, and 4) graded learning and responsibility (Table 1). These 4 principles were developed during discussions among the members of the Emergency Neurovascular Care Committee, Cardiovascular and Stroke Nursing Council, and Telestroke and Neurovascular Intervention Committees and are mainly based on the joint experience of these committees. While it seems intuitively logical that those principles should generally be followed in clinical routine, and particularly when caring for patients with acute stroke, doing so becomes even more critical during health care emergencies such as the COVID-19 pandemic because in such a situation, health care professionals have to take on new and additional roles and responsibilities in challenging working environments for which they were not specifically trained.
Four key principles for integration of new staff in the stroke team during a health care crisis
This document is also intended to encourage and empower working groups and institutions to create a framework for fast decision-making in crisis situations. In the following, we summarize key knowledge, unique characteristics (ie, tasks that are not ideal for new team members), and generic aspects (ie, tasks that lend themselves to new team members because they can extrapolate their experience from their previous working environment) for acute stroke care in 3 different settings: the neuroangiography suite (Table 2), Neuro-ICU (Table 3), and stroke unit (Table 4). We believe that in a crisis such as the COVID-19 pandemic, the focus should be on the generic aspects of stroke care: New team members can build on their pre-existing knowledge and skills and therefore contribute best to guideline-based stroke care.1 Given their greater experience, it might be reasonable to primarily assign stroke and particularly EVT-specific tasks to the “core members” of the stroke team.
Take-home points for new staff and unique-versus-generic aspects of stroke care in the neuroangiography suite
Take-home points for new staff and unique-versus-generic aspects of stroke care in the Neuro-ICUa
Take-home points for new staff and unique-versus-generic aspects of stroke care on the stroke unit
Neuroangiography Suite
The neuroangiography environment differs from the Neuro-ICU and stroke unit in that the patient with stroke remains there for only a short time. The risk of radiation exposure and handling of thrombectomy equipment is unique to the neuroangiography suite and yields additional challenges for new staff members. Furthermore, the neuroangiography staff has to execute several highly specialized technical tasks, such as positioning of the neuroangiography table and preparing the appropriate catheters and thrombectomy devices. Because chances of good outcome rapidly decrease with increasing time to reperfusion, workflows in the neuroangiography suite need to be maximally time-efficient. Examples of more generic tasks in the neuroangiography suite that would be suitable for new stroke-team members would be managing IV lines and blood pressure monitoring, while management of access-site complications, handling of endovascular devices, and reconstruction and labeling of angiography images should preferably be performed by key staff members (Table 2).
Neuro-ICU and Stroke Unit
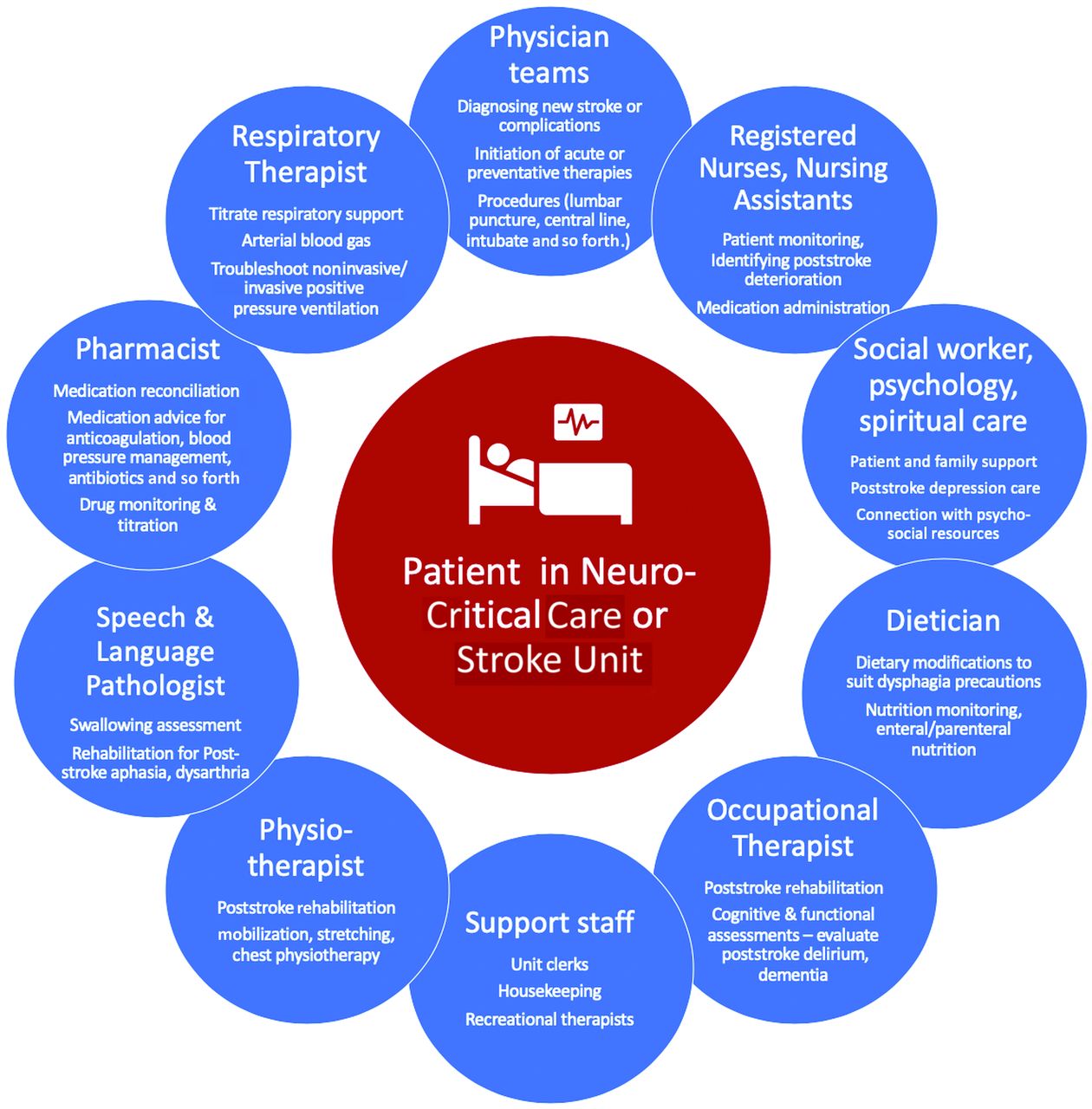
Acute ischemic stroke treatment does not stop once the occluded vessel has been opened. Post-EVT care on the Neuro-ICU and stroke unit is critical to support patient recovery and prevent poststroke complications, which may erase the benefits of EVT.2 Typical Neuro-ICU and stroke units share many similarities, whereas stroke units often represent a “step-down” environment in which patients may be at risk of requiring escalation to critical care. A collaborative multidisciplinary team environment with effective role delegation is the cornerstone of both the Neuro-ICU and stroke unit, with most roles being quite similar (Figure), with the notable absence of respiratory therapists in most stroke units. Neuro-ICU tasks that lend themselves to new team members are, for example, placement of nasogastric and orogastric tubes and Foley catheters, while more ICU-specific aspects such as vasopressor therapy and optimization of positive pressure ventilation parameters should ideally remain with the core team members (Table 3). In the stroke unit, new staff might want to start with managing patients’ routine medication and Foley catheter and IV-lines, while obtaining a detailed neurologic status such as the NIHSS would be a more suitable task for experienced team members (Table 4). Nevertheless, it would certainly be desirable for the newer team members to initiate structured training regarding stroke-specific tasks (eg, NIHSS score) under the guidance of pre-existent staff members as would be the local standard at that institution.
Simulation training (“dry” practice runs with a nurse or mannequin acting as the patient) can help to practice specific workflow steps, identify latent safety threats, and familiarize new team members with their new tasks.3 Simulation team training has also been shown to improve team functioning—communication and cooperation of different members among a medical team.4,5 This is particularly important for workflow in the neuroangiography suite because treatment delays at this stage will lead to delayed reperfusion and thereby directly affect patient outcome. It is important to establish continuous monitoring of treatment quality (eg, reperfusion quality and access site complications such as groin hematomas and infections following endovascular treatment) and workflow times (door-to-needle times, door-to-groin puncture times), particularly in a health care crisis, to ensure that treatment quality is maintained to the best of the ability of the system and to detect problems in EVT workflows and treatment quality early on, which grants the medical team the opportunity to intervene in a timely manner. One might be tempted to think that continuous performance monitoring for complex, multidimensional tasks involving numerous specialties as is the case in endovascular stroke treatment is impractical, but studies have repeatedly shown that team performance in medicine can be validly measured across complex settings and that doing so helps to improve treatment workflow.6
CONCLUSIONS
Endovascular stroke treatment reaches well beyond the neuroangiography suite and encompasses a wide range of specialties (neurology, neuroradiology, neurosurgery, anesthesia, intensive care) and designations (physicians [among them attendings, fellows, and residents], nurses, technologists, pharmacists, therapists, nutritionists, medical students, nurse practitioners, physician assistants), just to name a few. During the COVID-19 pandemic and other major health care emergencies, augmentation of staff from other areas may be required due to staff redeployment, staff exposures/required quarantines, and increased patient demands.7 This carries the risk of decreasing the quality of EVT and post-EVT care.8 Maintaining timely and comprehensive endovascular stroke care at a high quality during a health care crisis such as the COVID-19 pandemic is of utmost importance. Of note, the framework that was outlined in this article for integration of new members into existing stroke teams is based on personal experience of the American Heart Association/American Stroke Association Stroke Council Science Subcommittee members rather than objective data. Nevertheless, we would like to encourage individual stroke teams and their hospitals to collect data from their COVID-19 experience and publish them, because this would provide valuable information to stroke teams and help them to further improve EVT workflows and post-EVT care in similarly challenging situations.

A model of patient-centered multidisciplinary care in the Neuro-ICU or stroke unit that is both helpful and reassuring for new staff members. The model is quite similar in both the neuro-critical care and stroke units with the notable exception of respiratory therapists who are often not part of medical stroke units. While this model is, of course, generalizable to nonstroke settings as well, some specific examples are illustrated to show how different members of the team may synergistically address a stroke-related problem. For example, in a patient with dysphagia, the nursing or physician team may be the first to notice a poststroke deterioration with the patient choking or coughing during a simple trial. This prompts the team to involve the speech and language pathologist who confirms poststroke dysphagia and recommends a temporary nasogastric tube, which is inserted by a nurse (perhaps with a new nursing team member observing this common task), with the dieticians then helping ensure that the nasogastric feed provided meets the patient’s feeding requirements, potentially monitoring for a refeeding syndrome. These changes may be overwhelming for the patient and family, prompting the team to involve psychology to assess poststroke depression as well as social work and spiritual care to connect the patient and family to key resources.
Footnotes
Disclosures: Aravind Ganesh—UNRELATED: Consultancy: MD Analytics, My Medical Panel, Adkins Research Group, and Genome BC; Grants/Grants Pending: Rhodes Trust, Wellcome Trust, the University of Calgary, Alberta Innovates, the Canadian Cardiovascular Society, and the Canadian Institutes of Health Information; Payment for Lectures Including Service on Speakers Bureaus: National Health Service Health Education England; Patents (Planned, Pending Or Issued): a provisional patent application (US 63/024,239) for a system to deliver remote ischemic conditioning or other cuff-based therapies; Stock/Stock Options: SnapDx, TheRounds.ca, and Advanced Health Analytics; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: University of Calgary; OTHER RELATIONSHIPS: unpaid membership in the editorial boards of Neurology, Neurology: Clinical Practice, and Stroke. Andrew Southerland—RELATED: Consulting Fee or Honorarium: Legal Expert Consultation, paid to the University of Virginia Physicians Group on his behalf. UNRELATED: Board Membership: Neurology Podcast, Comments: I served as past section editor of the journal Neurology Podcast; I completed the paid role in 2018; Consultancy: NeurovView Diagnostics, Comments: unpaid consultancy, work completed; Employment: University of Virginia Health System; Expert Testimony: legal expert consultation, Comments: I provide expert legal review for vascular neurology and stroke cases, both plaintiff and defense work*; Grants/Grants Pending: Diffusion Pharmaceuticals, Comments: Principal Investigator, PHAST-TSC Trial, https://clinicaltrials.gov/ct2/show/NCT03763929*; Patents (Planned, Pending or Issued): US Patent Application No. 14/910,890 (iTREAT), US Provisional Patent Application No. 62/620,096 (BANDIT), Comments: patents pending. Peter Panagos—RELATED: Grant: National Institutes of Health/National Institute of Neurological Disorders and Stroke*; UNRELATED: Employment: Washington University. Norma McNair—UNRELATED: Board Membership: American Board of Neuroscience Nursing, Comments: reimbursement for travel expenses only, no payment. Kevin N. Sheth—UNRELATED: Consultancy: Ceribell, ZOLL; Grants/Grants Pending: National Institutes of Health, American Heart Association, Biogen, Bard, Novartis, Hyperfine; Stock/Stock Options: Alva. *Money paid to the institution.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received August 7, 2020.
- Accepted after revision August 21, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.