
Abstract
BACKGROUND AND PURPOSE: The development of thrombolytic agents for use with compromised cerebral blood flow has made it critical to quickly identify those patients to best treat. We hypothesized that combined diffusion and perfusion MR imaging adds vital diagnostic value for patients for whom the greatest potential benefits exist and far exceeds the diagnostic value of diffusion MR imaging alone.
METHODS: The cases of patients with neurologic symptoms of acute ischemic stroke who underwent ultra-fast emergent MR imaging within 6 hours were reviewed. In all cases, automatic processing yielded isotropic diffusion images and perfusion time-to-peak maps. Images with large vessel distribution ischemia and with mismatched perfusion abnormalities were correlated with patient records. All follow-up images were reviewed and compared with outcomes resulting from hyperacute therapies.
RESULTS: For 16 (26%) of 62 patients, hypoperfusion was the best MR imaging evidence of disease distribution, and for 15 of the 16, hypoperfusion (not abnormal diffusion) comprised the only imaging evidence for disease involving large vessels. For seven patients, diffusion imaging findings were entirely normal, and for nine, diffusion imaging delineated abnormal signal in either small vessel distributions or in a notably smaller cortical branch in one case. In all cases, perfusion maps were predictive of eventual lesions, as confirmed by angiography, CT, or subsequent MR imaging.
CONCLUSION: If only diffusion MR imaging is used in assessing patients with hyperacute stroke, nearly one quarter of the cases may be incorrectly categorized with respect to the distribution of ischemic at-risk tissue. Addition of perfusion information further enables better categorizing of vascular distribution to allow the best selection among therapeutic options and to improve patient outcomes.
In the diagnosis of acute stroke, MR imaging has been used as an objective measure to identify patients at risk for cerebral ischemia progressing to infarction. The development of IV and intraarterially administered thrombolytic agents for use in the earliest phases of compromised cerebral blood flow has made it critically important to quickly identify patients for whom such intervention might be most beneficial. The use of conventional MR sequences is limited because of their relative insensitivity during the initial onset of neurologic deficit (1, 2). Diffusion-weighted MR imaging has been shown to be an early marker for developing infarction (3). In animal models, changes on diffusion-weighted images have become apparent within 1 hour of middle cerebral artery occlusion (4–6). Several studies have verified the ability of diffusion-weighted imaging to identify areas of cerebral ischemia and infarction within hours of presentation, with sensitivity ranging from 94% to 100% (7–10). Thus, diffusion-weighted MR imaging would seem an excellent modality to identify adequately at-risk patients for cerebral infarction in the hyperacute stage.
In parallel, perfusion-weighted or hemodynamically weighted MR sequences were developed and then had application in the evaluation of hyperacute stroke (2, 9, 11–13). Further advance occurred when the two techniques were combined to better understand acute ischemia and developing cerebral infarction (14). When the combined techniques were applied to humans with stroke, it became possible to begin estimation of cerebral tissue viability as the spatial difference between abnormal perfusion and abnormal diffusion signals (9, 14, 15). However, an early tacit assumption remained that patients with unremarkable diffusion-weighted images of their brains were suffering no ischemia. Yet recent isolated reports have identified individual cases of negative diffusion-weighted imaging in patients with evolving deficits or even with completed strokes (8, 9, 16–18). We sought to identify the prevalence of falsely negative diffusion-weighted MR images of humans with hyperacute stroke symptoms. We thus hoped to clarify whether our perfusion sequence was required in addition to the diffusion sequence to identify correctly and sensitively all patients with large vessel ischemia when presenting in the 0- to 6-hour period from symptom onset, the current window of potential intervention. Our hypothesis remains that a combination of diffusion and perfusion MR imaging meets emergency time constraints, adds critical diagnostic value for patients for whom the greatest potential benefits of thrombolytic therapy exist, and far exceeds the diagnostic value of diffusion MR imaging alone.
Methods
The records of all patients who presented at our institution between January 1997 and December 1999 with onset of neurologic symptoms suspicious for acute ischemic stroke and who underwent ultra-fast emergent MR imaging within 6 hours were obtained and retrospectively reviewed. MR images were obtained using a 1.5-T whole body magnet with a 24-mT/m gradient strength, a 300-ms rise time, and an echo-planar-capable receiver (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany). The images included sagittal T1-weighted scout (15/6 [TR/TE]; matrix, 128 × 256; section thickness, 8 mm; field of view, 300 mm; one signal acquired), axial T2-weighted turbo gradient and spin-echo (4480/108; matrix, 132 × 256; section thickness, 5 mm; field of view, 230 mm; one signal acquired), and axial echo-planar diffusion- and perfusion-weighted MR images.
The diffusion-weighted images were obtained with a single shot, gradient-echo, echo-planar pulse sequence with diffusion gradient b values of 0 and 1000 s/mm2, along all three orthogonal axes over 18 axial sections (6000 [TR]; number of sections, 18; section thickness, 7 mm; no intersection gap; matrix, 96 × 128; field of view, 240 mm; one acquisition). Perfusion images were obtained during the first pass of a 0.1 mmol/kg bolus of gadolinium-based contrast material (Omniscan, Nycomed, Oslo, Norway; or Magnevist, Berlex Laboratories, Wayne, NJ) by using a gradient-echo, echo-planar sequence set for a selected 12 of the 18 section positions measured 30 times sequentially. This resulted in a total perfusion imaging time of 1 min and ensured imaging during the entire duration of the first passage of contrast material. Imaging parameters included a per-section image acquisition rate of approximately seven axial images per second, a TR of 1680, 4-mm-thick sections with a 0.5-mm intersection gap, 64 × 128 matrix, and 300-mm field of view with one acquisition. In all cases, diffusion-weighted data were automatically processed to yield trace images (standard isotropic diffusion-weighted images, not the mathematically specific trace of the diffusion tensor) at each section position from the primary data. The perfusion-weighted sequence generated a time-to-peak map for each section position. The total imaging time for all sequences was 3 minutes, and the total time for postprocessing was 3 minutes, yielding a total magnet time of 6 minutes.
A board-certified radiologist with added qualifications in neuroradiology and extensive experience in reading diffusion and perfusion MR images retrospectively reviewed the ultra-fast MR data. Specifically, images were categorized as normal, as having evidence of lacunar disease only, or as showing large vessel distribution ischemia. The latter group was further divided into those with matched abnormalities on diffusion and perfusion MR images and those that showed abnormalities on perfusion MR images only. Imaging information was correlated with patient records regarding ability to detect ischemic lesions and accuracy of categorizing ischemic lesions within a large vessel distribution. Clinical outcome at the time of hospital discharge was recorded and classified as minimal or no disability (allowing discharge to home), moderate disability (discharge to rehabilitation facility), severe disability (discharge to nursing home), or death. All follow-up CT scans or MR images obtained during the hospital course were reviewed and compared with clinical outcomes.
Results
During the period of time included in the study, a total of 62 patients underwent ultra-fast MR imaging to identify potential hyperacute strokes. For 16 (26%) of these patients, hypoperfusion was the best evidence of disease distribution, as evidenced by increased time-to-peak effect on postprocessed perfusion maps (Table). For 15 of the 16 patients, the hypoperfusion comprised the only imaging evidence for disease involving large vessel distributions. For the other patient, the perfusion maps showed involvement of a larger order vessel than that revealed by the diffusion study.
Clinical patient summary
For seven of the 16 patients, diffusion imaging findings were entirely normal (Fig 1A). For the remaining nine patients, diffusion imaging delineated abnormal signal in either small vessel perforator distributions in eight (Figs 2A and 3A) or in a notably smaller cortical branch in one. Concomitantly, perfusion imaging of the 16 patients uniformly revealed hypoperfused cortical tissue in large vessel distributions (Figs 1A, 2B, and 3B). In all these cases, perfusion maps were accurately predictive of ischemic foci, as confirmed by conventional angiography (13 patients), follow-up CT (two patients) (Fig 2C), or subsequent MR imaging (one patient). Intervention was initiated, ranging from supportive care through intraarterial thrombolysis, for all (Fig 3). Of the 16 patients for whom diffusion-perfusion mismatches were identified and treatments administered, six had achieved full recoveries at 90 days, without significant residual deficit (Barthel 90-day scores of 95–100), and three were discharged from the hospital to rehabilitation units with only mild residual deficits. Two of the 16 sustained large infarcts, and one experienced a large parenchymal hemorrhage while receiving heparin; all three were discharged to nursing homes with significant deficits. The final four died during their initial hospitalization (Fig 1B).

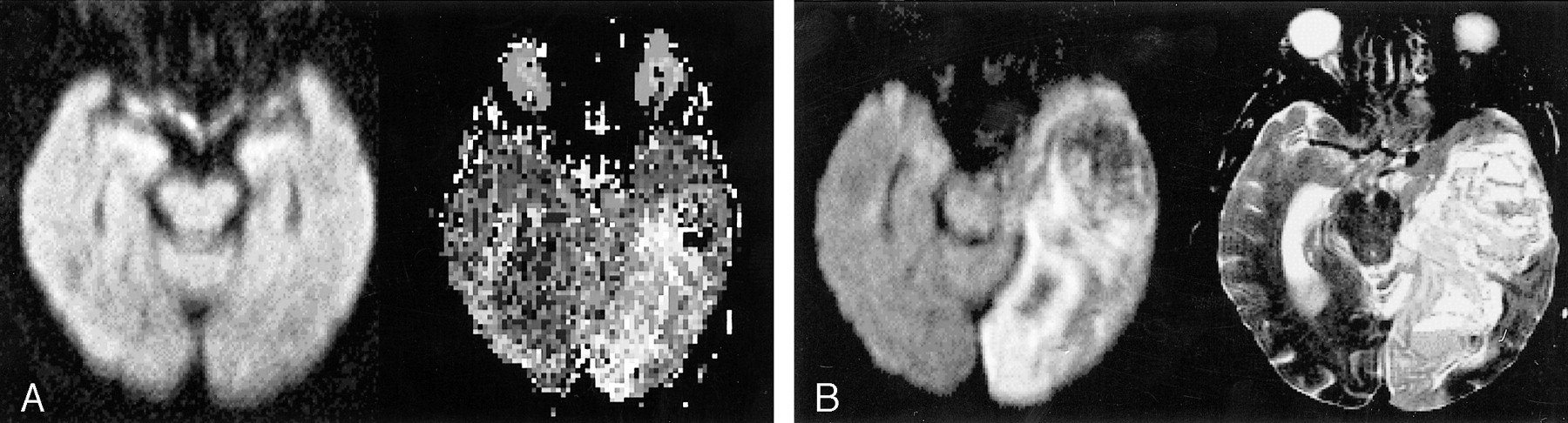
Images from the case of patient 1, an 88-year-old woman.
A, Isotropic trace diffusion image (5900/159/2 [TR/TE/excitations]) shows normal signal (left). Time-to-peak perfusion map (2199/82/35) (right) shows hypoperfusion throughout the left posterior cerebral artery territory. Although these images were obtained within a therapeutic window, no symptoms referable to this distribution were encountered until hours later. The patient was treated “conservatively” in an intensive care unit and received heparin. The results were evident at the 48-hour follow-up examination.
B, Repeat isotropic trace diffusion image shows the progression to infarct rather than ischemia in the left posterior cerebral artery territory (left). A T2-weighted (3500/96/1) image (right) reveals not only infarct but also hemorrhage, with mass effect presumably from the combination of infarct and heparin

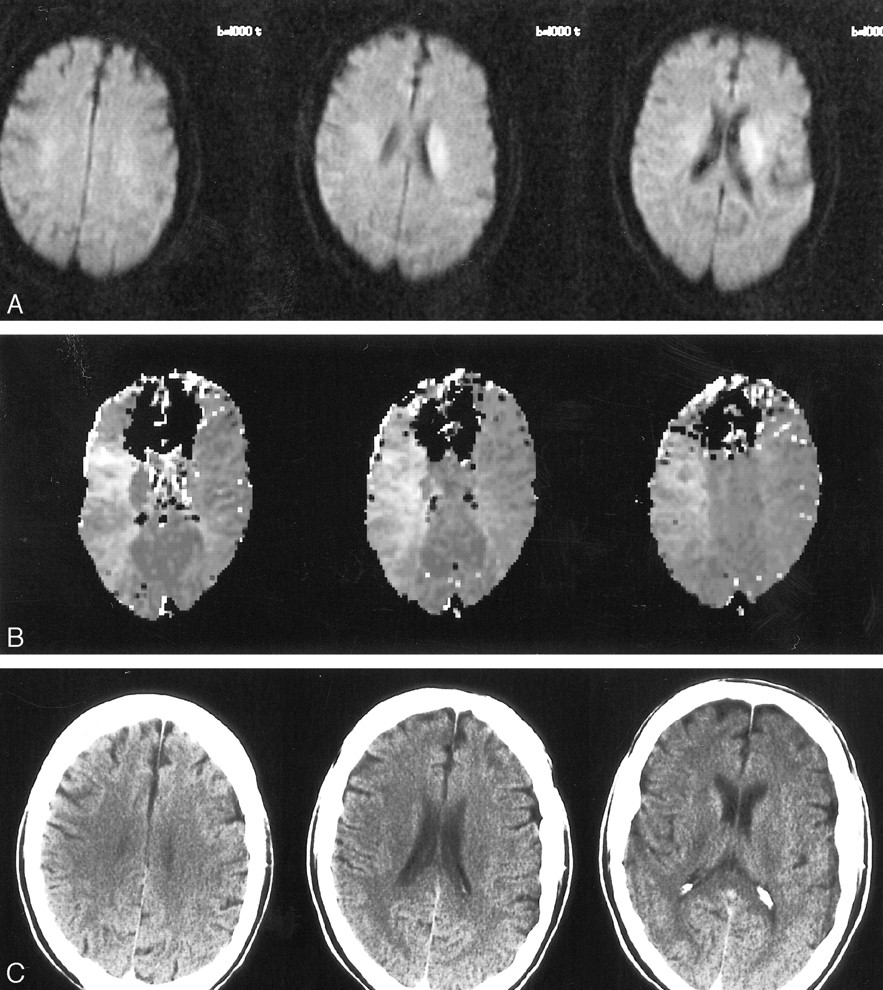
Images from the case of patient 3, a 71-year-old man.
A, Three sections of isotropic trace diffusion images (5900/159/2) show abnormal increased signal in a contiguous 2-cm region of the left corona radiata, without any associated signal change in cortical regions.
B, Three time-to-peak perfusion maps (2199/82/35), obtained immediately after the diffusion images and at the same section positions, show slight hyperperfusion in the distribution of the abnormal diffusion signal shown in A. In addition, they show the otherwise unseen hypoperfusion throughout the left middle cerebral artery territory.
C, Representative sections from follow-up CT of the head, obtained 5 hours after the IV administration of thrombolytic therapy, show no infarct and no hemorrhage. The patient had no residual symptoms at the 48-hour follow-up examination

Images from the case of patient 5, a 75-year-old woman.
A, Three sections of isotropic trace diffusion images (5900/159/2) show abnormal hyperintensities limited to the left corona radiata and deep frontal white matter.
B, Three time-to-peak perfusion maps (2199/82/35), obtained immediately after the diffusion images and at the same section positions, show marked hypoperfusion in the territory of the posterior division of the left middle cerebral artery.
C, Angiographic frames obtained before (left) and after (right) the intraarterial administration of thrombolytic therapy. Note the wedge of absent posterior vessels (to the right of the left image) compared with the addition of three large branches after therapy (white arrows).
D, Isotropic trace diffusion images, obtained at the 24-hour follow-up examination, reveal only scattered subcortical white matter hyperintensities (thin white arrows), without evidence for cortical infarct.
E, Follow-up perfusion maps obtained at the same levels show normal symmetrical time-to-peak effects
Discussion
We reviewed our MR imaging data on patients presenting with hyperacute stroke symptoms before potential treatment and identified 15 (24%) of 62 patients for whom the perfusion time-to-peak maps were the only MR imaging indication of large vessel ischemic disease, even in comparison with isotropic diffusion trace images. For an additional patient, the perfusion map showed an increased order of vessel occlusion compared with diffusion images. These data initially seem to contradict those presented in previous reports of 88% to 100% sensitivity for diffusion images to detect acute cerebral infarcts (7, 8, 18–20). Our findings most likely represent the decreased sensitivity of diffusion imaging during the most hyperacute period when ischemia may be present before more advanced cellular damage or tissue infarction. Recent reports have previously identified isolated cases of hyperacute stroke with negative diffusion-weighted images and abnormal perfusion data (16, 17). Our study confirms these observations and, on a larger scale, shows that if only diffusion imaging is used in assessing hyperacute stroke, nearly one quarter of the cases may be incorrectly categorized with respect to the large vessel distribution of ischemic at-risk tissue. Furthermore, if therapeutic triage were based on the diffusion images alone, treatment would incorrectly be withheld from these patients who harbor the largest volumes of penumbra or ischemic brain that may be salvaged from infarction.
Diagnostic imaging in acute stroke continues to evolve. Initially, previous work focused on an apparently high sensitivity and specificity of diffusion-weighted MR imaging in diagnosing hyperacute stroke. Although this modality has been well studied during the acute (1–2 days) period (14, 17, 19), experience during the hyperacute stage (0–6 hours), during which time thrombolytic therapy is thought to be of maximal benefit, is more limited. Of 11 patients studied by Sorensen et al (9), two patients had negative diffusion-weighted imaging findings but resolution of symptoms within 48 hours. Other investigators have reported sensitivities between 98% and 100% and a 100% specificity of diffusion MR imaging in cases of hyperacute stroke. (7, 8, 17, 20). Reviewing data on 151 patients, Lovblad et al (8) reported an 88% stroke detection sensitivity using diffusion-weighted imaging within 6 hours, whereas negative findings were observed for all 14 patients without stroke. In a review of more than 700 patients with stroke symptoms evaluated from 0.5 to 38 hours from symptom onset, Ay et al (19) reported the cases of 27 patients with normal diffusion-weighted imaging results. After further clinical or radiologic follow-up, they thought that 17 of these patients had cerebral infarction or ischemia. This would represent an overall false-negative rate for diffusion imaging of 17 per 782, or 2%. Most recently, Oppenheim et al (21) reported a 6% false-negative rate for diffusion-weighted images obtained within 48 hours of symptom onset and further noted that the majority (six of eight) were found in posterior circulation. In comparison, we found seven completely normal diffusion images despite large areas of hypoperfusion among our 62 patients and the preponderance of anterior circulation lesions, an 11% false-negative rate, again likely reflecting our very early time of imaging relative to onset of symptoms (all within 6 hours and within the therapeutic window for thrombolysis). We encountered no complete false-positive perfusion maps, although for one patient (patient 7), angiography revealed a distal carotid embolus with intact collaterals across the anterior communicating artery. For this patient, abnormal diffusion signal was shown in the perforator territory only.
The use of perfusion data to generate additional information regarding tissue at risk of ischemia had been well recognized (22–25). Although potentially time consuming and requiring the administration of contrast material, it has been previously shown that the addition of perfusion data obtained during the first passage of contrast material using a time-efficient processing algorithm involves an average imaging and processing time of only 3 minutes (1). Accurate categorization in the hyperacute stroke setting is critical to better triage patients for thrombolytic therapy, considering the costs and potential complications of such therapies (26). Mismatches between perfusion- and diffusion-weighted images in cases of hyperacute stroke have been well recognized, and it has been hypothesized that subtraction of the area of diffusion abnormality from the area of perfusion deficit can provide an estimate of the ischemic penumbra (9, 27). This is consistent with observations that the critical threshold of cerebral blood flow in animals below which membrane pump failure and cytotoxic edema occurs is below the threshold of flow at which EEG suppression is apparent (17, 28–32). Thus, the brain under hypoperfusion may be symptomatic at the levels of abnormal cerebral blood flow where EEG suppression occurs, whereas regions of restricted diffusion may not appear until the lower thresholds for edema and pump failure are crossed. Therefore any “false-negative” diffusion-weighted images are more likely to be seen early in the disease process, as the cerebral blood flow falls but before entry into the lowest ranges.
The use of perfusion MR imaging in addition to diffusion MR imaging allowed early accurate depiction of a patient population at extreme risk for whom we were able to intervene to improve outcomes. Despite the acuity of these patients and despite large areas of hypoperfusion, six patients were successfully rescued by thrombolysis and were able to survive without any significant clinical deficit. An additional three patients sustained relatively mild deficits after successful thrombolysis in one and mechanical clot disruption in another. This allowed discharge to rehabilitation centers with expectation of a reasonable quality of life despite the initial potential insult. Three other patients survived but with sufficient deficits to require entry to nursing homes. This left the final four mortalities, a rate of 25% despite attempts at revascularization, among our patients who had normal or near-normal diffusion imaging findings with large areas of hypoperfusion. This shows that large volumes of perfusion deficits during the hyperacute period, even in the absence of diffusion changes, are predictive of a high risk for poor outcome. Perhaps most strikingly, we have also shown that aggressive early intervention can improve outcomes compared with the natural history of an 88% mortality rate among patients with occlusion of distal internal carotid or proximal middle cerebral arteries (33). In our series, although we had a more mixed population of large vessel lesions, our overall mortality rate was considerably less, and only one of 10 patients presenting with hypoperfusion resulting from internal carotid or middle cerebral artery occlusions died.
Conclusion
In summary, although abnormal diffusion data in the setting of hyperacute stroke may provide an estimate of the extent of tissue infarction, in our experience, normal or near-normal diffusion data do not preclude the presence of a large ischemic penumbra of at-risk tissue. Thus, addition of perfusion information increases the sensitivity for detecting ischemic at-risk tissue and categorizing its vascular distribution to enable the best selection among therapeutic options. Furthermore, accurate early depiction of these potentially devastating lesions can permit aggressive intervention to significantly improve patient outcomes.
Footnotes
1 This work was presented in part at the 1999 Annual Meeting of the Radiological Society of North America and the 2000 Annual Meeting of the American Society of Neuroradiologists.
↵2 Address reprint requests to Jeffrey L. Sunshine, MD, PhD, Department of Radiology, University Hospitals of Cleveland, 11100 Euclid Avenue, Cleveland OH 44106.
References
- Received October 4, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Emerging impact of CTA/perfusion CT on acute stroke thrombolysis in a community hospital
- Management of Stroke in Infants and Children: A Scientific Statement From a Special Writing Group of the American Heart Association Stroke Council and the Council on Cardiovascular Disease in the Young
- Neuroimaging applications of multislice CT perfusion
- Guidelines and Recommendations for Perfusion Imaging in Cerebral Ischemia: A Scientific Statement for Healthcare Professionals by the Writing Group on Perfusion Imaging, From the Council on Cardiovascular Radiology of the American Heart Association
- Quantification of Perfusion Using Bolus Tracking Magnetic Resonance Imaging in Stroke: Assumptions, Limitations, and Potential Implications for Clinical Use