
Abstract
BACKGROUND AND PURPOSE: Although neuroangiography remains the criterion standard standard for the detection of and surgical/interventional planning for cerebrovascular diseases, it usually requires that patients be confined to bed rest for several hours after angiography to prevent local complications. Decreasing catheter size has reduced the risk of hemorrhagic complications associated with early ambulation after angiography. For this study, we prospectively evaluated the clinical feasibility of a 3.3F catheter/sheath system for selective neuroangiography.
METHODS: One hundred seventeen consecutive patients (49 men, 68 women; age range, 18–83 years; mean age, 56.9 years) underwent selective neuroangiography using 3.3F catheters. The exclusion criteria for this study included a subsequent surgical/neurointerventional procedure performed within 18 hours and necessity of arch aortography, which is routinely performed for the first examination of patients with ischemic cerebrovascular diseases. The procedure was evaluated prospectively in terms of success rate, compression time of the arterial puncture site, and periprocedural complications.
RESULTS: Selective catheterization of the intended arteries was performed in 99% of the carotid arteries and 97.4% of the vertebral arteries. No neurologic complications or local hemorrhagic complications were observed. Manual compression time after the procedure ranged from 3 to 7 minutes (mean, 3.7 minutes), and patient bed rest after the procedure ranged from 2 to 3 hours (mean, 2.04 hours).
CONCLUSION: Selective neuroangiography with a 3.3F catheter/sheath system is feasible and enables early ambulation in selected patients.
The clinical usefulness of less invasive vascular imaging techniques, such as MR angiography and CT angiography, has recently been reported (1–3). The imaging quality of these modalities has been advancing rapidly, although neuroangiography remains the gold standard for the detection of, surgical/interventional planning for, and follow-up of cerebrovascular diseases. However, the necessity of prolonged focal compression and bed rest after the procedure, which carries the risk of pulmonary embolism, is a great disadvantage to patients (4–6). A recent comparative study in diagnostic neuroangiography showed that the use of a sheath increased the maneuverability of the catheter and reduced bleeding at the puncture site during the procedure (7). Decreasing the catheter size has reduced the risk of hemorrhagic complications associated with early ambulation after angiography (8–10). The purpose of this study was to evaluate the clinical feasibility of a 3.3F catheter/sheath system for selective neuroangiography.
Methods
Patient Selection
For this study, we selected patients for whom the examination was intended to be diagnostic only, no aortic arch aortography was needed, and follow-up during the ensuring 18 hours was possible. One hundred seventeen patients (71 with cerebral aneurysms, 16 with vascular malformations, 15 with brain tumors, eight with suspected cerebral aneurysms, and seven with cerebral arterial stenosis after percutaneous transluminal angioplasty), after providing informed consent to be part of this study, underwent diagnostic selective neuroangiography using a 3.3F catheter/sheath system. A total of 270 patients underwent diagnostic neuroangiography between June 1, 2000, and February 28, 2001. Eighty-four patients were excluded from the study because interventional or surgical procedures were performed within 18 hours after the diagnostic neuroangiography. Informed consent could not obtained from 37 patients, and they were also excluded.
Aortography with a pigtail catheter is routinely performed during the first examination of patients with ischemic cerebrovascular diseases treated at our institution. Because a 3.3F pigtail catheter was not available, 32 patients with ischemic cerebrovascular diseases were excluded. The characteristics of the patients are summarized in Table 1. The patients included 49 men and 68 women ranging in age from 18 to 83 years (mean age, 56.9 years). The mean patient body size was 57.4 kg (range, 37–100 kg) in weight and 158.5 cm (range, 142–178 cm) in height. Nine of the 117 patients received antiplatelet drugs, and two of them received an anticoaglant. From the blood data obtained several hours before the procedure, the mean prothrombin time was 10.9 seconds (range, 9.5–12.7 seconds), the mean partial thromboplastin time was 30.8 seconds. (range, 29.8–32.4 seconds), and the mean platelet count was 267,000/mm3 (range, 108,000–611,000/mm3).
Characteristics of participants
Instrument and Techniques
The 3.3F catheter that we used (Medikit, Miyazaki, Japan) is made of a polyamide membrane containing a barium and stainless wire mesh that increases its resistance to kinking. The catheter comes in various shapes, including the John-Benson type 1, John-Benson type 2, and Simmons type 2. The 3.3F catheter has a lumen of 0.89 mm, and a 0.032-in guidewire can be inserted through its lumen. It can be accurately observed via fluoroscopy. The maximum injection rate of contrast medium (Iopamidol 370, Schering, Germany) is 6 mL/s at 800 psi in vitro. The 3.3F sheath is 1.58 mm in outer diameter (Medikit).
All arteriography was performed via femoral arterial access with local anesthesia by using biplane DSA equipment (Advantx LCN Plus, GE Medical Systems) by two angiographers with 4 or 11 years of experience. Five to 25 mL of nonionic contrast medium (Iohexiol, 300 mg I/mL) was injected at a rate of 2–5 mL/s via the catheter. Selective arteriography was performed using the guidewire technique with a 0.032-in guidewire (Radifocus, Terumo, Tokyo). Heparin was intravenously administered to patients with histories of ischemic cerebrovascular disease or for procedures that were prolonged for more than 40 minutes. Intravenously administered heparin (1000–2000 U; mean, 1233 U) was used in 15 of 117 patients. After completion of angiography, the puncture site was compressed manually for at least 3 minutes, until hemostasis was obtained. We removed the pressure after 3 minutes and observed the puncture site for at least 20 seconds to confirm whether hemostasis was obtained. If hemostasis was not achieved at 3 minutes, manual compression was continued with a check at 1-minute intervals. The puncture sites were compressed with bandages, and the patients were then confined to bed rest, during which their vital signs were monitored. Neuroradiologists and/or neurosurgeons checked the conditions of the puncture sites, including maintenance of hemostasis, at 2 and 18 hours after the procedure. If there were no complications, such as local hematoma, oozing, and/or neurologic deficits, at 2 hours after angiography, it was time for ambulation. If hemorrhagic complications or oozing were observed after 2 hour, bed rest with local compression with a bandage was continued, with checks performed at 30-minute intervals.
The success rate of selective catheterization for the intended arteries and the duration of the diagnostic arteriographic procedures (from initiation of local anesthesia to removal of the catheter) were investigated. The image quality of all angiograms was evaluated by two neuroradiologists and one neurosurgeon using a two-degree grading scale as follows: good (clearly showed the lesion and cerebral arterial branches) and poor (obscured cerebral arterial branches and/or lesions). The time required for manual compression at the puncture site, time to ambulation after completion of angiography, rate of hemorrhagic complications at the puncture site, and neurologic complications during the procedure and for ≤18 hours after the procedure were assessed. A neurologic complication was defined as any new focal neurologic deficit or change in mental status during angiography or during the 18 hours after the procedure.
Results
For a review of the results, see Tables 2 and 3. In 115 (98.3%) of 117 patients, 280 of 284 selective catheterizations of the intended arteries were completed with the 3.3F catheter alone (59 common carotid arteries, 124 internal carotid arteries, 22 external carotid arteries, and 75 vertebral arteries). In the two remaining patients, four attempts at catheterization failed. In one of the two patients, catheterization into the left vertebral artery failed because of coiling of the artery at its origin; a 4F catheter was required for selective vertebral arteriography. In the other patient, transfemoral catheterization using a 4F catheter failed because of significant atherosclerotic tortuousness of the iliofemoral artery; the patient then underwent neuroangiography via transradial access. The number of catheters used in each patient ranged from one to two (mean, 1.05 catheters).
Success rate of the selective catheterization
Results during and after procedure
The mean duration of the diagnostic arteriographic procedures using the 3.3F catheter was 24.7 minutes (range, 6–62 minutes). The duration of the study of one or two vessels ranged from 6 to 32 minutes (mean, 17.4 min) and that of the study of more than three vessels ranged from 15 to 62 minutes (mean, 31.9 min).
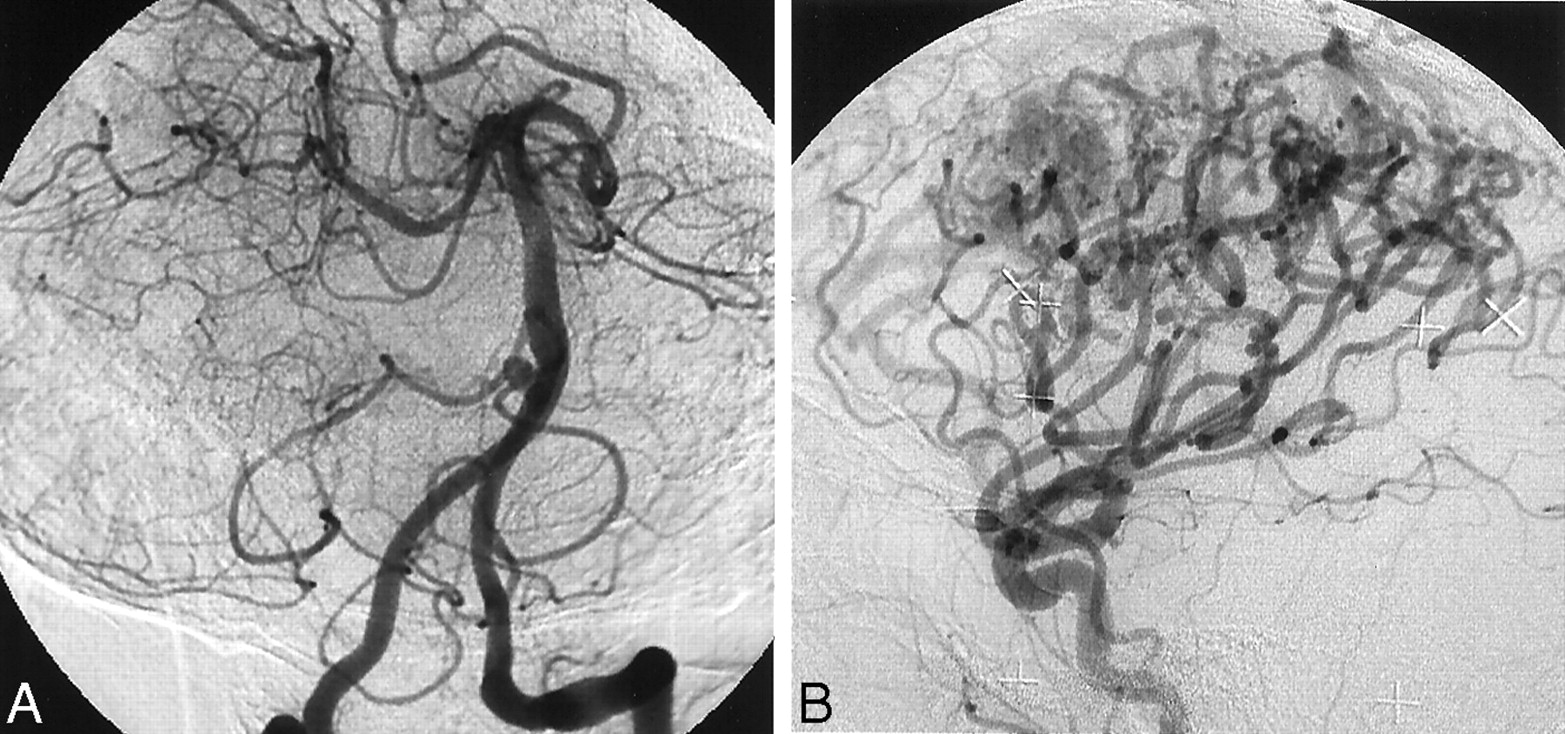
All 280 arteriograms were reviewed and evaluated by two neuroradiologists and one neurosurgeon. All except one of the arteriograms, obtained from a patient with a high-flow arteriovenous malformation, were evaluated as good (99.4%) (Fig 1).

Arteriograms evaluated using a two-degree grading scale of good and poor.
A, Right anterior oblique arteriogram of the left vertebral artery was evaluated as good. A small aneurysm of the right vertebral-basilar junction can be seen. Note a retrograde flow to the opposite vertebral artery.
B, Lateral arteriogram of the common carotid artery in a patient with a high flow arteriovenous malformation was evaluated as poor. Peripheral branches of the cerebral arteries are not well visualized.
The required manual compression time after the procedure ranged from 3 to 7 minutes (mean, 3.7 minutes) in patients for whom the 3.3F catheter/sheath system alone was used (n = 115). The time to ambulation after the procedure ranged from 2 to 3 hours (mean, 2.04 hours). One hundred eight (94%) of 115 patients walked at 2 hr after the procedure, five walked at 2.5 hours, and two walked at 3 hours because oozing at the puncture sites was noted at 2 or 2.5 hours after the procedure.
No hemorrhagic complications at the puncture sites were observed within 18 hours after ambulation. No neurologic complications, including transient ischemic attack, were observed in any of the patients. In one patient, a transient rash in the face and chest was observed 6 hours after the procedure, which was probably due to delayed allergic reaction to the contrast medium.
Discussion
Neuroangiography carries some risks during and after the procedure. Neurologic complications of neuroangiography are rare but can be serious. Several studies using large samples have reported neurologic complication rates ranging from 0.54% to 2.3% (11–14). Hemorrhagic complications, such as groin bleeding or hematoma, are common (7, 12, 13). Because these local complications, as compared with neurologic complications, less frequently cause serious results, less attention has been paid them (15). However, these local complications and/or prolonged groin compression to prevent them cause patients undue burden. Further, prolonged groin compression may increase the risk of pulmonary embolism from femoral venous thrombosis (4–6). The size of the catheter/sheath system, compression time, and ambulation time are important factors associated with hemorrhagic complications. Decreasing the size of the catheter/sheath system may reduce the rate of hemorrhagic complications and may allow for early ambulation. Several reports by cardiologists have presented findings on catheter size and local complications. Hematomas after cardiac catheterization were observed in 10–15% of patients for whom a 7F or 8F catheter was used and in 3.5–8% of those for whom a 5F catheter was used (8–10). In our study, by performing neuroangiography using the 3.3F catheter/sheath system, reduction of local complications and early ambulation (mean, 2.04 hours) were achieved. The use of an arterial sheath may affect hemorrhagic complications after the procedure. Sheaths have an outer diameter that is slightly larger than that of the catheters placed through them. Some angiographers do not routinely use the arterial sheath because of the cost of the sheath and because they think that its use increases the risk of bleeding after the procedure. Moran et al (7) reported the value of the sheath in a randomized controlled study using diagnostic neuroangiography with a 5F catheter for a large sample. In their study, the incidence of hematoma after the procedure was not significantly different between groups (11.4% in the sheathless group versus 11.9% in the sheath group), and the incidence of bleeding at the puncture site during the procedure was lower in the sheath group (1.7%) than in the control group (35.6%).
Transbrachial and transradial approaches have been used for selective neuroangiography. One benefit of these techniques is the reduction of restrictions on a patient’s activity after angiography. Although a high success rate (similar to that of the transfemoral approach) of selective catheterization by these techniques has been reported, some reports of transbrachial angiography have described a relatively higher occurrence of significant local complications, such as brachial artery thrombosis and dissection (16, 17). Percutaneous transradial neuroangiography has recently been reported (18–20). The occurrence of significant local complications associated with this approach is lower than that associated with the transbrachial approach. A recent report of transradial cerebral angiography in 166 cases showed excellent results; selective angiography was completed without major vascular complications in all patients except 12 who were poor candidates for this procedure (20). However, in that study, angiography of the common carotid artery was very frequently performed and selective angiography of the internal and/or external carotid arteries was infrequently (20–21%) performed, in comparison with our study (50–55%).
In one patient in our study, selective neuroangiography was completed via a transradial approach after the transfemoral approach failed. However, patients should be selected before angiography, based on confirmation of the collateral blood supply to the hand from the ulnar artery by using Allen test. In our experience with transradial neuroangiography in 40 patients selected by using the Allen test, all procedures succeeded without any significant complications, although two minor complications (one radial spasm and one radial pulseless) were encountered and this technique is more complicated than the transfemoral approach (unpublished data). Because early ambulation (within 2 hours for most patients) after transfemoral neuroangiography using the 3.3F catheter/sheath system was achieved in this study, transbrachial or transradial neuroangiography would be useful, especially for patients in whom the transfemoral route is not feasible or is difficult.
The potential problems of a small catheter are poor maneuverability and poor arterial opacification. Prolongation of the procedure due to poor maneuverability of the catheter increases the risk of neurologic complications during neuroangiography. Notably, duration of the procedure in this study (mean, 24.7 minutes) was not longer than that in previously reported studies by using 5F or larger catheters (4, 13). No neurologic complications were observed in this study, although it must be noted that this study includes a relatively small number of patients and that the rate of neurologic complications can be affected by several factors, such as the presence of the ischemic cerebrovascular diseases, prolongation of the procedure, and experience of the surgeon.
Regarding the limitations of the use of a 3.3F catheter for neuroangiography, arch aortography cannot be performed because the 3.3F pigtail catheter is no longer available. Arch aortography is sometimes necessary to search for aberrant vessels, stenosis of the vessels at the origin, and aortic diseases such as aortic dissection. More recently, Komiyama et al (21) showed the technical feasibility of a 3.2F catheter with a 0.68-mm inner diameter for diagnostic cerebral angiography of 30 patients. In their study, a 98.9% success rate of selective cerebral angiography was achieved. They also performed arch aortography of 10 patients with the same catheter with an injection of 10 mL of contrast material at the rate of 5.6 mL/s. Because we have thought that enough opacification of contrast material in each brachiocephalic vessel for obtaining a sufficient diagnostic image in arch aortography requires an injection rate of >10 mL/s, we excluded 32 patients with ischemic cerebrovascular diseases who needed arch aortography from this study. If sufficient aortograms are obtained with these small catheters, application of the 3.3F catheters used in this study will be expanded to include these cases. Further investigation, including a larger number of arch aortograms obtained with these small catheters, is necessary for assessment of the feasibility of the small catheters for cerebral angiography in patients who need arch aortography. Therefore, at this moment, the 4F catheter should be used for the initial examination of patients with suspected ischemic cerebrovascular or aortic disease.
Conclusion
The results of this study show that the 3.3F catheter/sheath system is a safe and less invasive technique for neuroangiography in selected patients.
Acknowledgments
We thank Toshihiko Iwano and Kazuaki Horinouchi for assistance in this study.
References
- Received June 5, 2001.
- Accepted after revision December 3, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}