
Abstract
Summary: Although absence of the common carotid artery (CCA) is a rare anomaly, the specific configuration in our case makes it extremely rare. Clinical, angiographic, ultrasonographic, and embryologic correlations of this anomaly are discussed after the case report.
Absence of the CCA is rare. Fewer than 25 cases have been reported in the literature, with only five angiographically proved cases. Only one case had ultrasonographic correlation (1). To the best of our knowledge, in all reported cases, the ECA originated proximal to the ICA, which makes our case an extremely rare occurrence (2–15). Absence of the CCA has no side or sex preferences (5), can occur bilaterally (5, 9), and is asymptomatic unless associated with other conditions. Among reported associations are cervical aortic arch, double aortic arch, right-sided aortic arch with aberrant left subclavian artery, and persistent trigeminal artery (5). Although in our case, the right ICA had no significant stenosis, symptomatic stenoses have been reported in association with this anomaly (11).
Case Report
Bilateral cerebral angiography was performed on a 72-year-old female patient with a medical history of hypertension, hypercholesterolemia, recent silent myocardial infarction, left hemispheric transient ischemic attacks, and a family history of stroke and coronary artery disease. The CCA was absent on the right side, but unlike the usual configuration of separate internal carotid artery (ICA) and external carotid artery (ECA), in our case, the right ICA originated proximal to the right ECA (Figs 1 and 2). No significant stenoses were found on the right side. Other findings were tortuosity of the right ICA at the level of C3–C4 (Fig 2) and hypoplasia of the A1 segment of the right anterior cerebral artery. High grade, short segment ostial stenosis of the ICA was found on the left side. The results of the examination were otherwise unremarkable. The patient then underwent stent placement of the stenotic left ICA. As part of post-stent placement workup, a bilateral carotid Doppler examination was performed, which showed satisfactory peak systolic velocities of the stented left ICA and normal pattern of spectral waveforms for the right ICA and ECA.

Right brachiocephalic angiogram. Digital subtraction angiogram obtained in a right anterior oblique projection. The ICA (I) arises proximally from the right brachiocephalic artery (B). The ECA (E) arises distal to the ICA. The right vertebral artery (V) and right subclavian artery (S) are also seen.

Frontal view digital subtraction angiogram.
A, Course of the right ICA in the neck. Note the tortuosity at the C3–C4 level (arrowhead).
B, Course of the right ECA in the neck.
Discussion
Angiography
When absence of the CCA occurs on the right side, the ECA usually arises proximally from brachiocephalic artery and the ICA arises distally from the subclavian artery proximal to the origin of the vertebral artery (5). In the presence of subclavian artery stenosis between the ICA and vertebral artery, steal syndrome can occur. When the anomaly occurs on the left side, both the ECA and the ICA arise from the aortic arch, with the ECA proximal to the ICA (5). Practical consequences of this anomaly are technical difficulties in performing brachiocephalic angiography. This anomaly can be missed during selective ICA angiography when it is presumed that the catheter tip is introduced into the ICA above the presumed level of CCA bifurcation. Unlike all reported cases, in our case, the ICA arose proximal to the ECA.
Ultrasonography
Ultrasonography is usually the first test with which to detect the possibility of an absent CCA when the sonographer cannot find normal carotid bifurcation in the neck. Intrathoracic bifurcation of the CCA also can cause the same problem. No significant difference has been reported in resistive indices of ICA and ECA in this anomaly and in normal cases, indicating that the resistive indices and spectral waveforms of the ICA and ECA are mainly determined by their supplied organs and not the CCA (1, 16).
Embryology
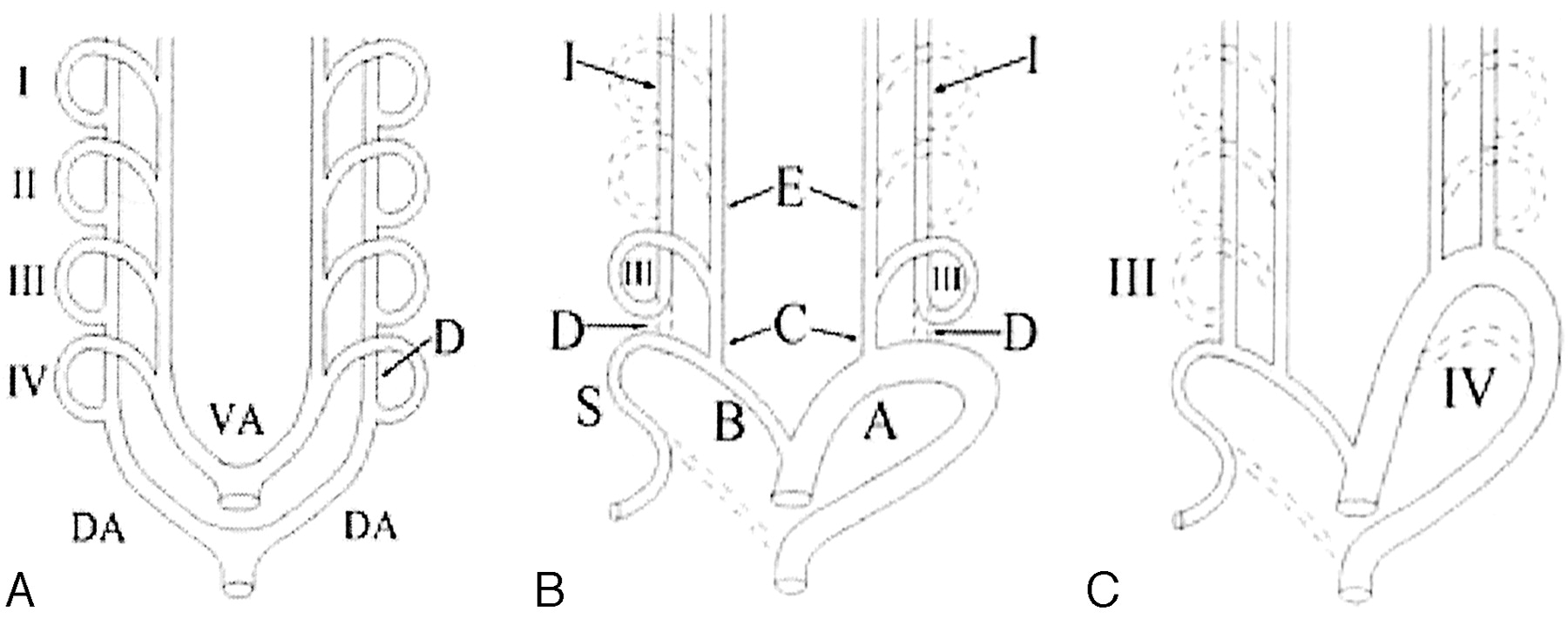
In a 12- to 14-mm embryo, the ductus caroticus, which connects the third and fourth branchial arches, dorsally involutes and the proximal portion of ECA forms the CCA, the third branchial arch forms the carotid sinus and the proximal portion of the ICA, and the fourth branchial arch forms a portion of the main aortic arch on the left side and a portion of SCA on the right side (Fig 3A and B) (17). The usual form of absent CCA with the ECA proximal to the ICA occurs either because of persistence of the ductus caroticus and regression of the third branchial arch or because of regression of the fourth branchial arch with resultant cervical aortic arch (Fig 3C). In our case, however, it is likely that an extra twisting of the separate ICA and ECA occurred, causing the ECA to be distal to the ICA.

A, Simplified diagram shows the ventral aorta (VA) and dorsal aorta (DA), with four pairs of branchial arches (I, II, III, and IV) in a 2- to 4-mm embryo. The fifth and sixth arches are not shown. The part of dorsal aorta between the third and fourth branchial arches is called the ductus caroticus (D).
B, In a normal 12- to 14-mm embryo, the ductus caroticus (D) and most of the first, second, fifth, and sixth arches involute. The proximal portion of the ECA (E) forms the CCA (C). The third arch (III) forms the carotid sinus and proximal portion of the ICA (I). On the left side, the fourth arch forms the aortic arch (A), and on the right side, it forms the brachiocephalic artery (B) and subclavian artery (S).
C, Absence of the CCA may occur if the third branchial arch (III) involutes and the ductus caroticus persists (right) or, alternatively, if the fourth branchial arch (IV) involutes and the persistent third branchial arch forms a cervical aortic arch (left).
Conclusion
Absence of the CCA is rare. It is usually incidentally found at autopsy or during workup for other clinical problems; however, it may cause significant practical diagnostic and therapeutic challenges. Unlike other reported cases of an absent CCA with the ECA arising proximal to the ICA, in this case, the ICA arose proximal to the ECA. Reviewing the reported cases of absence of the CCA reveals that the supplied organs of the ICA and ECA and not the presence of the CCA are the main determinants for the shape of resistive indices and frequency of plaque formation and stenosis in these arteries.
- Received April 28, 2002.
- Accepted after revision May 4, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Republished: A rare case of absent left common carotid artery with bovine origin of the left external carotid artery
- A rare case of absent left common carotid artery with bovine origin of the left external carotid artery
- Congenital absence of the common carotid artery in a patient with a ruptured anterior communicating artery aneurysm